
Abstract
Purpose:
To evaluate the primary anatomic and physiological success of scleral buckling surgery for rhegmatogenous retinal detachment and factors influencing its outcomes.
Methods:
This is a prospective analytical study of 92 eyes that underwent scleral buckling at the Lumbini Eye Institute and Research Center, in Lumbini, Nepal. Parameters evaluated which could influence the outcome of the surgery included the lens status, duration of symptoms, locations of breaks, the extent of retinal detachment, and preoperative proliferative vitreoretinopathy.
Results:
A total of 92 eyes from 88 patients with rhegmatogenous retinal detachment were evaluated; 68 (74%) eyes were of male and 24 (26%) were of female. The mean time of presentation was 4.71 ± 8.45 months. The overall primary anatomical and physiological success was achieved in 79 (84.9%) and 68 (73.9%) of the cases at 6 months. Sixteen cases developed re-detachment (mean duration of 2.8 ± 1.8 months). Eleven of the cases had a successful anatomical outcome and five of the patients had persistent detachment despite second surgery. In phakic patients, the primary success rate was 92.7% whereas in pseudophakic it was 71.4%. Proliferative vitreoretinopathy 10 (63%) was the most common cause of surgical failure. Bilateral buckling at the same setting was done to two patients—both achieving primary success.
Conclusion:
Scleral buckling is a very good surgical option for rhegmatogenous retinal detachment and represents a surgical technique worth being trained, performed, practiced, and continued despite advancements in modern vitreoretinal surgical devices and preference for vitrectomy and tamponade agents. It may also be successfully tried in cases of bilateral rhegmatogenous retinal detachment if a doubt regarding compliance for follow-up and surgery for the fellow eye exists.
Keywords
Introduction
Retinal detachment refers to the detachment of the neurosensory retina from the underlying retinal pigment epithelium (RPE). Among the three types of retinal detachment, rhegmatogenous, exudative, and tractional, the rhegmatogenous form of detachment is the most frequently occurring type, in which a retinal tear allows liquefied vitreous humor to pass underneath the retina. Liquefied vitreous being the major culprit in the majority of the cases. 1
The first description in retinal detachment was made by James Ware in 1805 and he also attempted the first operation for the same and suggested the drainage of subretinal fluid by puncturing the sclera with a knife.2–4 Helmholtz then made an accurate and reliable clinical diagnosis on rhegmatogenous retinal detachment (RRD) in 1850. 5 Meanwhile, Von Graefe 6 in 1863 modified the method of surgery by also puncturing the retina and creating a second hole for the drainage of the subretinal fluid into the vitreous cavity. In 1920, Jules Gonin coined the main cause of retinal detachments was the presence of retinal break and sealing of this breaks to be the prime factor responsible for successful reattachment of the retina after surgery. He also performed the first successful treatment of retinal detachment by sealing the retinal break to the underlying RPE and the choroid.7–9 Thus, the basic concept of retinal detachment surgery includes mechanical or scar-induced sealing of the hole in the retina. 1
From 1920 to 1965, various modifications in retinal detachment surgery were made. And it was in 1965, Brockhurst and colleagues described the classic scleral buckling (SB) technique of lamellar dissection, diathermy of the scleral bed, and the use of silicone buckling materials with an encircling band to close the breaks.10,11 Later in 1965, Lincoff recommended non-drainage procedures and changed diathermy to cryotherapy for retinopexy. 12 Currently, three main techniques are used to treat RRD: (1) scleral buckle surgery, (2) pars plana vitrectomy with retinopexy and intravitreal tamponade, and (3) pneumatic retinopexy.13–15
The principle of SB operation is to seal off retinal break, decreasing vitreoretinal traction and providing external as well as an internal tamponade to the break which is achieved by scleral indentation is achieved by placing a permanent episcleral explant/buckle at a location corresponding to the retinal break. Buckle materials contain silicone sponge and hard silicone of various shapes and sizes. Buckle-induced scleral indentation lowers the severity of vitreous traction, modifies the direction of vitreous traction, and decreases the flow of vitreous fluid through the break into the subretinal space. The placement of a buckle on its own does not prevent a retinal break. Using either externally applied cryotherapy or laser photocoagulation, permanent adhesion between neuro-retina and RPE is achieved. 16
Starting from the success rate of 50% in Gonin’s era, the surgical procedure has been evolving to reach the success rates of 90% or higher. But, to date, none of the techniques have been proven to be superior over the other. The decision of surgery depends largely on the experience and choice of the surgeon, the existence, length, and degree of the RRD, the number, location, extent, and type of retinal break, and the presence of any associated features.17–19
Materials and methodology
This is a prospective noncomparative consecutive interventional case series performed at Lumbini Eye Institute and Research Center, Lumbini, Nepal, from April 2017 to May 2018. A total of 88 consecutive patients were analyzed prospectively. The research has been approved by the ethics committee and the institutional review board and has adhered to the tenets of the declaration of Helsinki.
Several parameters including the age, the time from onset of symptoms to the presentation, lens status, number of breaks, type, and locations of breaks, the extent of retinal detachment, preoperative proliferative vitreoretinopathy (PVR) were examined. The primary success rate was defined as anatomic success being stable over a period of at least 6 months after surgery. The physiological success was defined as a gain in two lines from baseline from Snellen’s visual acuity chart. Approval from the institutional review board was taken and written informed consent was obtained from each patient enrolled for the treatment.
Inclusion criteria included patients with RRD. Exclusion criteria included any previous medical or surgical vitreoretinal procedures, extensive PVR mandating vitrectomy, retinal detachments due to perforating or penetrating injuries with or without an intraocular foreign body, tractional retinal detachments, glaucomatous cupping, uveitis, and macular hole.
Results
A total of 92 eyes of 88 patients with RRD who underwent SB surgery were evaluated. The patients had a median age of 40 years (10–80 years); 68 (74%) were male and 24 (26%) were female (male:female 1.7:1). The mean time of presentation after symptoms developed was 4.71 (±8.45) months. Forty-eight patients had RRD in the right eye, 38 in the left eye, and 2 patients in both the eyes. The most common causes of RRD were idiopathic, trauma, post-cataract surgery, and myopia (Table 1).
Baseline demographics and ocular characteristics of patients with RRD.

RRD, rhegmatogenous retinal detachment; SD, standard deviation.
The overall primary anatomical and physiological success was achieved in 79 (85%) and 68 (73.9%) of the eyes at 6months. Sixteen (17.3%) of the eyes with an initially attached retina after SB had a re-detachment (mean duration of 2.8 ± 1.8months) following SB surgery.
All of the cases of re-detachment underwent pars plana vitrectomy (PPV) with silicone oil tamponade. Eleven (70%) of the cases with re-detachment had a successful anatomical outcome and 5 (5.4%) of the patients had persistent detachment despite surgery (Table 2).
Primary surgical and physiological success rates in patients undergoing scleral buckling surgery.

PL, perception of light.
The postoperative visual acuity was found to have an inverse correlation with the duration of the presentation. Patients who presented with a mean duration of 3.45 months of symptoms (95% confidence interval (CI): 0.47–6.42, p < 0.05) were found to have good postoperative visual acuity while those who presented after mean duration of 4.43 months or more (95% CI: 3.49–10.3, p < 0.05) had poorer visual outcomes (Table 3).
Post operative visual acuity of patient presenting at different durations since symptoms and undergoing scleral buckling surgery.

CI, confidence interval; PL, perception of light.
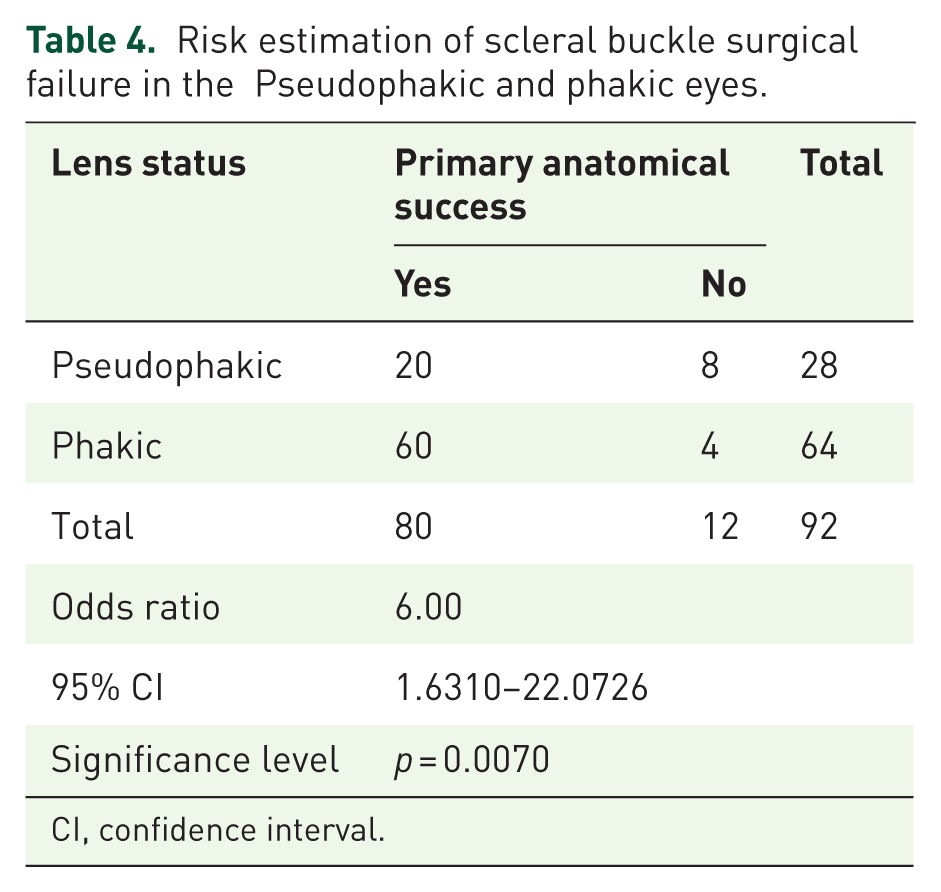
Risk estimation of scleral buckle surgical failure in the Pseudophakic and phakic eyes.
CI, confidence interval.
We analyzed this association using linear regression estimator which also confirmed that patients who presented with longer duration of symptoms had poorer outcomes in comparison to those who presented earlier (p = 0.027) (Figure 1).

Linear regression analysis eliciting worse visual outcomes with increasing duration (0: 6/6–6/18; 1: <6/18–6/60; 2: 6/60–3/60; 3: <3/60–PL).
There were 64 phakic eyes (69.6%) and 28 (30.4%) pseudophakic eyes (phakic: pseudophakic ratio of 2.28:1). A direct comparison between the phakic and the pseudophakic eyes showed that pseudophakia had a greater chance of having a primary surgical failure (odds ratio (OR): 6.00, 95% CI: 1.63 -22.07, p = 0.007) (Table4).
The primary success rate was 92.7% in phakic eyes whereas in pseudophakic patients (n = 28, 30.4%) a primary success rate was 71.4%. With re-surgery via pars plana, the success rate increased by 1.2% (93.9%) in the phakic patients and 24% (95.4%) in pseudophakic eyes (p < 0.05)
PVR (10 of the 16) Grade C (p > 3, with or without A) was by far the most common cause for re-detachment. Only two of the cases which had re-detachment due to PVR have new breaks. Other causes included breaks located closer to the equator (6 of 16 detachment cases), and detachment of more than three consecutive quadrants (5 of 16 re-detachment cases). Bilateral buckling at the same setting was also done to two patients—both of whom achieved primary success.
Discussion
SB surgery has been considered as the conventional ‘gold standard’ for uncomplicated RRD, young high myopic eyes, and most importantly in phakic eyes due to its lesser risk in the development of postoperative cataract. 20 With the rapid development of PPV techniques along with upgrades in vitrectomy machines, SB has slowly started losing its glory days and has started becoming a lesser chosen surgical approach in the treatment of RRD.21,22 However, due to the requirement of costly equipment such as a microscope, viewing system, and vitrectomy machine along with trained manpower, it is usually not accessible to all setup. This factor also makes SB the choice of treatment in most RRD in developing and less privileged part of the world because of its comparable outcome over PPV, low cost, and extra ocular approach. Besides these, SB is still recommended in RRD of young phakic patients with non-liquefied vitreous or in patients with minimal PVR.23,24
In our study, primary anatomical success was obtained in 84.9% and functional success was obtained in 73.9% at 6months postoperative period with a mean duration of the success of 4–5 months. Shankar and colleagues 22 in their retrospective study of 65 patients who underwent scleral buckle surgery for repair of RRD report a primary anatomical success rate of 90.77% and success rate after second surgery was 98.46%. In their study, time of presentation was 1 day to 3 months with 32% cases with macula-off. In our study, the mean duration of the presentation was 4.71 (±8.45) months; 92.7% of the patients had ‘macula-off’ at presentation and 77.6% of patients at the time of presentation had visual acuity <3/60 preoperatively.
Similarly, Khan and colleagues 21 on their prospective study on 50 eyes of 50 patients with uncomplicated RRD reported the primary anatomic success of 82% was achieved by single procedure with success rate increasing to 94% following PPV. In our study, the overall success increased to 96% following vitrectomy and tamponading with silicon oil which is comparable with both of the above.
Shankar and colleagues 22 reported that re-detachment in six cases was secondary to PVR grade C with vitreous hemorrhage and formation of a new break in one of the cases. Whereas in our case, we had 16 cases of re-detachment at a mean duration of 2.8 ± 1.8 months from surgery. The cause of re-detachment was shorted to be PVR changes, break near the equator and break involving more than three consecutive quadrants.
It is also well known from various studies that the final visual outcome is dependent on the duration of the macula-off RRD.25–27 We analyzed this relation and found similar findings. Patient who presented within mean duration of 3.45 months of symptoms (95% CI: 0.47–6.42, p < 0.05) were found to have good postoperative visual acuity (6/18) or more while those who presented after mean duration of 4.43 months or more (95% CI: 3.49–10.3, p < 0.05) had visual outcomes ranging from 6/60 to 3/60. Patients presenting at a mean duration of 7.19 months (95% CI: 5.12–13.6, p < 0.05) had very poor visual prognosis despite successful anatomical outcomes with visual acuity ranging from 3/60 to perception of light. We analyzed this association using linear regression estimator which also confirmed that patients who presented with longer duration of symptoms had poorer outcomes in comparison to those who presented earlier (p = 0.027).
Heimann and colleagues 13 in their multicenter study have reported better anatomical and visual outcome in phakic eyes. We report similar finding from our study where primary success rate in the phakic eye was 92.7% and in the pseudophakic eye was 71.7%. There were 64 (69.6%) phakic patients and 28 (30.4%) pseudophakic patients (phakic: pseudophakic ratio of 2.28:1). A direct comparison between the phakic and the pseudophakic eyes showed that pseudophakia had a greater chance of having a primary surgical failure (OR: 6.00, 95% CI: 1.63–22.07, p = 0.007). With re-surgery via pars plana, the success rate increased by 1.2% in the phakic patients and 24% in pseudophakic eyes (p < 0.05).
PVR is often considered the main cause of anatomical failure of RD surgery.28–32 Similarly, in our study, 10 of the 16 (62.5%) cases of re-detachment were primarily due to PVR. Other causes included breaks located closer to the equator (6 of 16 detachment cases), and detachment of more than three consecutive quadrants (5 of 16 re-detachment cases).
Conclusion
Despite the development of modern techniques and technologies as vitrectomy machines, lasers, and tamponading agents, SB can still be considered as a very good surgical option for RRD. It can still be considered a gold standard in phakic and young patients with minimal PVR. It can also be considered in pseudophakic eyes with comparable results. In cases of failures, a timely second surgery can still yield good anatomical outcomes; however, the duration for which the retina has remained detached remains an important prognostic indicator for visual outcome.
The limitation of this study is—it is a single center study. Outcomes of buckle surgery from various other centers and from multiple surgeons would add further value to our findings.
Footnotes
Ethical clearance
The research has been approved by the ethics committee and the institutional review board of Lumbini Eye Institute and Research Centre, Lumbini, Nepal and has adhered to the tenets of the declaration of Helsinki. Ethics approval code: 1279/017/018.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Conflict of interest statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Recommendations
Scleral buckle is a surgical technique that is worth training, performing, practicing, and reviving the art lost in vitreoretinal surgery.