
Abstract
A 31-year-old male patient presented with the complaint of progressive vision loss in his left eye. Slit-lamp examination showed posterior embryotoxon, iris hypoplasia, and iridocorneal adhesion in both eyes, corectopia in the right, and peripheral inferior thinning and ectasia in the left eye. Corneal topography showed slightly asymmetric bowtie pattern in the right eye and crab-claw pattern in the left eye. Topographic examination was compared with his previous topography. The comparison showed 1.6-D steepening of maximum keratometry (Kmax) and 22-µm decrease of thinnest corneal pachymetry. Corneal crosslinking treatment was performed on the left eye. At the postoperative 28-month follow-up visit, Kmax decreased from 54.1 to 53.0 D and corrected distance visual acuity improved to 20/20 with scleral lens. This is the first reported a case with Axenfeld–Rieger syndrome and pellucid marginal degeneration association. We suggest that corneal crosslinking can be useful for management of pellucid marginal degeneration and longer follow-up might be needed in order to corroborate the effectiveness of the corneal crosslinking procedure.
Introduction
Axenfeld–Rieger syndrome (ARS) is an autosomal-dominant disorder in which structures of the anterior segment of the eye are improperly developed as a result of impaired neural crest cell migration and differentiation during embryonic development. 1 ARS patients present with a spectrum of anterior segment anomalies including a prominent and anteriorly displaced Schwalbe’s line (posterior embryotoxon), iridocorneal adhesions, and iris anomalies like policoria, corectopia, hypoplasia, and ectropion uveae. Patients with ARS have an approximately 50% risk of developing glaucoma. Systemic anomalies may also accompany to ARS like the abnormality of the cardiovascular outflow tract, craniofacial abnormalities that consist of tissues of neural crest origin, and dental and skeletal anomalies. 2
Pellucid marginal degeneration (PMD) is a usually bilateral, progressive ectatic corneal disorder involving the inferior cornea. The thinning extends 1–2 mm away from the limbus and the cornea above the thinned out area is ectatic. Patients usually present with reduced visual acuity caused by high irregular astigmatism. Corneal topography shows characteristic crab-claw pattern representing inferior steepening with flatter vertical corneal meridian. 3 Inferior keratoconus, in which the cone is localized away from the corneal center and a crab-claw pattern is seen on the sagittal topographic map, is often confused with PMD. 4 However, both prognosis and management of PMD and keratoconus are different, and PMD should be distinguished from keratoconus. 5 Inferior keratoconus does not show the classic band-like inferior thinning that is best demonstrated by a full coverage (12-mm) corneal thickness map. Therefore, analyzing only the anterior corneal surface without additional information is not sufficient in the differential diagnosis of inferior keratoconus and PMD.
Although corneal disorders like megalocornea 6 and keratoconus7,8 were reported in patients with ARS, PMD was not reported yet. In this case report, we aimed to present the results of corneal crosslinking (CXL) treatment in a case with ARS and unilateral progressive PMD.
Case report
A 31-year-old male patient of Turkish Caucasian origin presented to hospital with the complaint of slow but progressive vision loss in his left eye. There were not any history of previous intraocular surgery and symptoms of atopy and eye rubber. Corrected distance visual acuity (CDVA) was 20/20 in the right eye and 20/200 in the left eye. Slit-lamp biomicroscopic examination showed posterior embryotoxon, iris hypoplasia, and iridocorneal adhesion in his both eyes, corectopia in the right eye, and peripheral inferior thinning and ectasia in the left eye (Figure 1(a) and (b)). Intraocular pressure measured by a Goldmann applanation tonometer was 13 mmHg in the right eye and 16 mmHg in the left eye. Gonioscopy revealed multiple broad iris processes and prominent Schwalbe’s line. The dilated fundus examination showed normal maculas and no evidence of any retinal anomaly. In addition, no glaucomatous changes were detected in the optic disk and retinal nerve fiber layer analysis. Anterior sagittal curvature map (Pentacam HR; Oculus) showed a slightly asymmetric bowtie pattern in the right eye and a crab-claw pattern in the left eye, and the bell sign was seen in the full coverage (12-mm) corneal thickness map in the left eye (Figure 2(a) and (b)). Scheimpflug imaging of the patient also confirmed the peripheral thinning of the left cornea, while the right cornea was unremarkable (Figure 3(a) and (b)). No systemic abnormalities were reported.

Slit-lamp examination revealed posterior embryotoxon, iris hypoplasia, and iridocorneal adhesion in the right (a) and left (b) eyes.
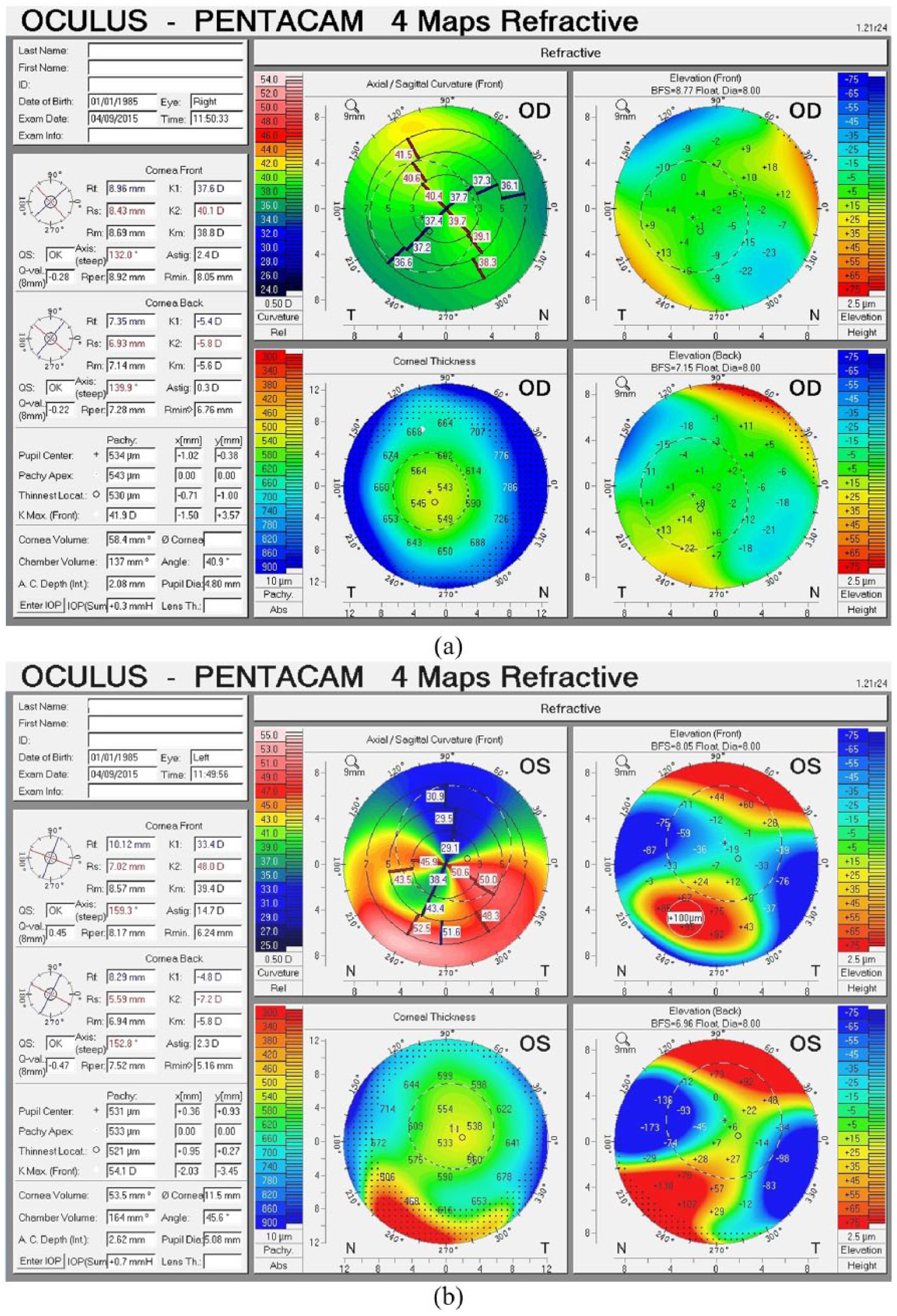
Anterior sagittal curvature map shows a slightly asymmetric bowtie pattern in the right eye (a) and a crab-claw pattern in the left eye (b). The bell sign was seen in the full coverage (12-mm) corneal thickness map in the left eye (b).

Scheimpflug imaging shows the normal thickness of the right cornea (a) and the peripheral thinning of the left cornea (b).
Topographic examination was compared with a previous (6 months earlier) topographic examination (Pentacam HR) which was evaluated in a different medical center. The comparison showed 1.6-D steepening of maximum keratometry (Kmax) and 22-µm decrease of thinnest corneal pachymetry. Therefore, corneal CXL was performed on the left eye. Corneal epithelium was removed mechanically in an 8-mm area which was slightly decentralized through the inferior region. Iso-osmolar 0.1% riboflavin solution was instilled to the cornea every 3 min for 30 min. Ultraviolet A (UVA) irradiation at 3 mW/cm2 was applied for 30 min.
The follow-up period was 28 months. Visual acuity, Kmax, and corneal thickness were evaluated during the postoperative period. At the 28th month of follow-up, topographic evaluation showed 1.1-D flattening of Kmax and 88-µm decrease of thinnest corneal pachymetry (Figure 4) compared to preoperative topographic findings and CDVA improved to 20/20 with scleral lens (Figure 5). No intraoperative and postoperative complications occurred.
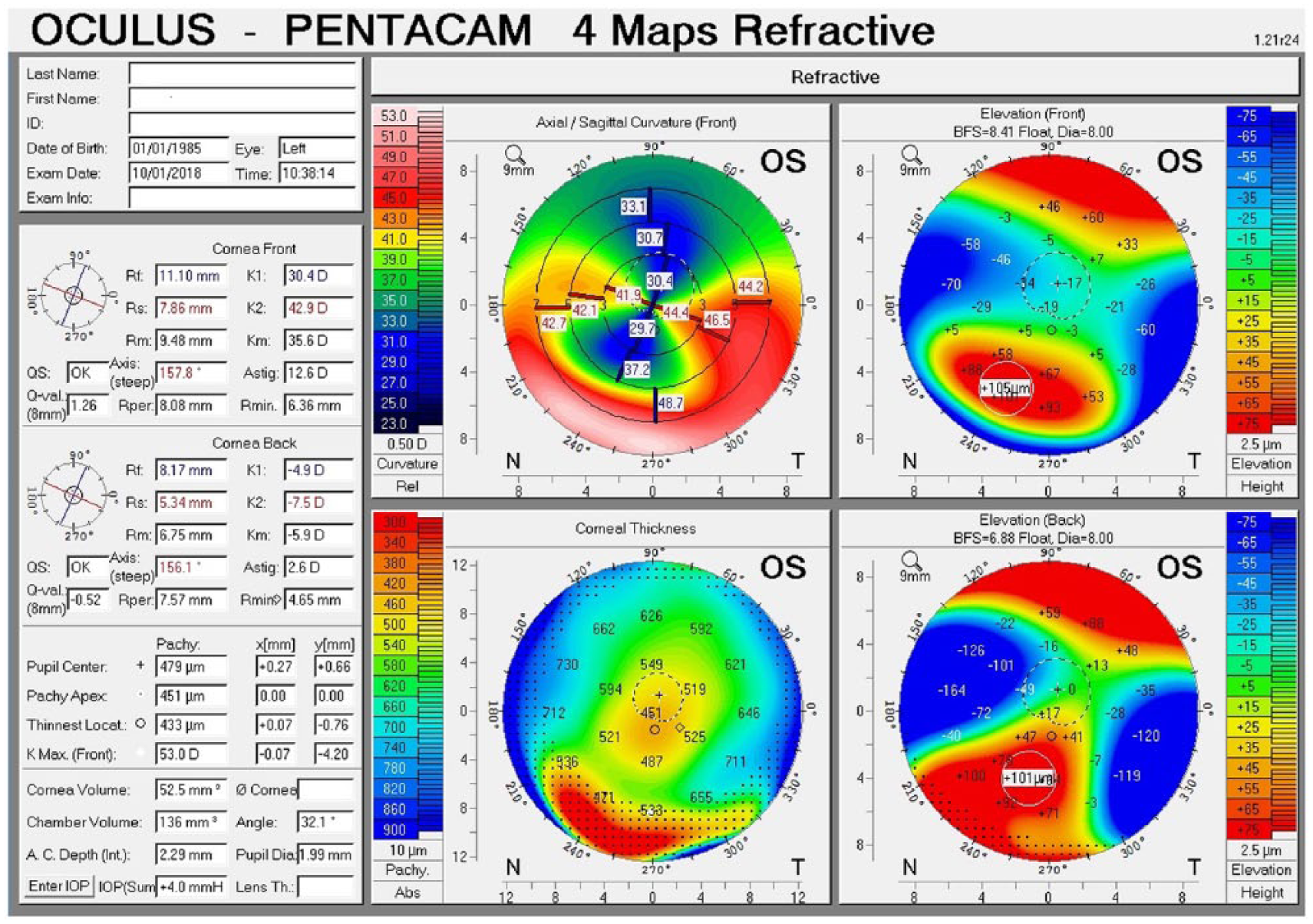
Anterior sagittal curvature and full coverage corneal thickness map at the postoperative 28th month after corneal CXL in the left eye.

Biomicroscopic image of the left eye with scleral lens.
Discussion
ARS develops as a result of improper neural crest cell migration and differentiation of the anterior segment structures. It is an autosomal-dominant disorder. 1 Two major genes involved in the pathogenesis of ARS are PITX2 and FOXC1. 2
In addition, Micheal and colleagues 9 also found a mutation in the PRDM5 gene in ARS. These genes demonstrate full penetrance and variable expressivity. PMD is characterized by thinning of the corneal stroma. Like most of the anterior segment structures, corneal stroma also originates from neural crest cells. However, any genetic basis is not defined yet for PMD. 10 In our case, ARS was bilateral but PMD was unilateral. PMD is a mostly bilateral disorder, and unilateral PMD is rare. 11 Therefore, it is unlikely that the PITX2 and FOXC1 mutation itself is responsible for the PMD findings. The PMD and ARS association in this case is most likely coincidental.
Corneal CXL is useful for halting the progression of corneal ectatic disorders like keratoconus, PMD, and post-LASIK ectasia.12,13 The literature concerning the results of corneal CXL in PMD is limited. While corneal CXL has been found to be effective in stopping PMD progression, improving CDVA and reducing irregular astigmatism in numerous case reports,13–16 there is no randomized prospective study evaluating larger groups of patients. Tuffaha and colleagues 17 reported a case of progressive PMD treated with corneal CXL after a previous unsuccessful implantation of intracorneal segments. After 1-year follow-up, an increase in corneal biomechanical properties accompanied by an improvement in CDVA was observed. Also Kymionis and colleagues 18 present a case of progressive PMD treated by simultaneously photorefractive keratotomy and corneal CXL. At 12 months postoperatively, uncorrected and best-corrected visual acuities improved and corneal topography revealed a significant improvement. Mamoosa and colleagues 19 evaluated visual acuity, refractive errors, and topographic outcomes 6 months after corneal CXL in 21 eyes of 15 patients with PMD and their results demonstrated a significant reduction in keratometry values, an improvement in CDVA at the 6th month of follow-up. Bikbov and colleagues 20 evaluated the clinical effectiveness of corneal CXL in 16 eyes of 9 patients with PMD and reported that uncorrected and best-corrected visual acuities improved and corneal topography revealed a significant improvement in 1-year follow-up. Only, Steppat and colleagues 16 reported a progression of PMD after corneal CXL in 1 of their 13 cases. Also, Uysal and colleagues 8 reported that a case with ARS and keratoconus developed sterile keratitis after accelerated corneal CXL (9 mW/cm2). There were no complications after accelerated corneal CXL in our case report.
In conclusion, unilateral PMD and ARS were present in our case, which had not been reported previously and PMD progression halted via corneal CXL treatment. This case showed that corneal CXL can be useful for management of PMD.
Footnotes
Acknowledgements
M.K., P.K., M.I., and K.T. performed the medical practices; M.K., P.K., M.I., and K.T. conceived the concept of this study; M.K., P.K., and M.I. performed data collection or processing; M.K., P.K., M.I., and K.T. performed the analysis or interpretation; M.K. and K.T. performed the literature search; M.K., P.K., M.I., and K.T. wrote the manuscript. This case report was partially presented in the 51st National Ophthalmology Congress of the Turkish Ophthalmology Association (24–29 October 2017; Antalya, Turkey).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Conflict of interest statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Informed consent
A written informed consent was obtained from the patient to publish medical data and images.