
Abstract
Azithromycin is used widely in clinical practice and recently it is available in topical solution for ophthalmic use. The purpose of the current publication is to summarize the newest information on azithromycin’s clinical usefulness over ocular diseases. A PubMed (National Library of Medicine) and a ScienceDirect search was conducted using the key phrases ‘azithromycin’, ‘meibomian’, ‘blepharitis’, ‘trachoma’, ‘toxoplasmosis’ from 2010 to 2017. Articles were limited to articles published in English or at least having an English abstract. There were no restrictions on age, ethnicity, or geographic locations of patients. Topical azithromycin was found effective and safe in various ocular surface infections, in meibomian gland dysfunction and in trachoma. Also, it may substitute fluoroquinolones in corneal UV cross-linking. The World Health Organization targets for trachoma elimination are being reached only after 3 years of annual mass drug administration. Oral azithromycin can participate in combination regiments for toxoplasmosis, mainly because of its very good safety profile and may play a significant role in toxoplasmosis in pregnancy. Azithromycin is one of the safest antibiotics, well tolerated, and with special pharmacokinetic properties. Also, it is characterized by a broad antimicrobial spectrum. Azithromycin is efficacious for the treatment of a lot of ocular diseases and may be included as monotherapy or in combination therapy in new treatment protocols for more ocular infections. However, more research is needed to determine this.
Introduction
Azithromycin (AZM) is the first azalidic antibiotic, a class of macrolide antibiotics, which has derived from erythromycin. 1 It is widely used in clinical practice, not only for respiratory diseases and sexually transmitted infections but also for ocular diseases. 2 It has bacteriostatic properties against a wide spectrum of both gram-positive and gram-negative bacteria, atypical bacteria, and some protozoa.1,3 Although it was synthesized already in the early 1980s, it is still being investigated for the treatment of various diseases. In 2007, it was approved as the first ophthalmic solution (AZM 1.0%) to treat bacterial conjunctivitis. 4 Previously, it was prescribed (mainly orally) for a number of very important and frequent eye infections, such as trachoma, as well as for diseases with ocular manifestations. In recent years, it has received increasing attention because of its supplementary effects on host defense reactions and chronic human diseases. Its immunomodulatory effects are under investigation and are considered of significant clinical importance. 5 This review summarizes the newest information on AZM’s clinical usefulness over ocular diseases.
The special pharmacokinetic properties (Table 1) of AZM are the main reason for the continued interested in the drug. In short, these are as follows: a wide antimicrobial spectrum, long half-life, excellent tissue penetration and extensive tissue distribution, high drug concentrations within cells (including phagocytes), and considerable immunomodulatory effects. In comparison with earlier macrolides, it shows enhanced stability in acidic media while it expresses increased antimicrobial activity at alkaline pH. Moreover, because AZM is metabolized slowly and produces inactive metabolites, does not affect the P450 cytochromes, so it does not interact with medications being metabolized by P450.1–4
Azithromycin’s pharmacokinetic properties.
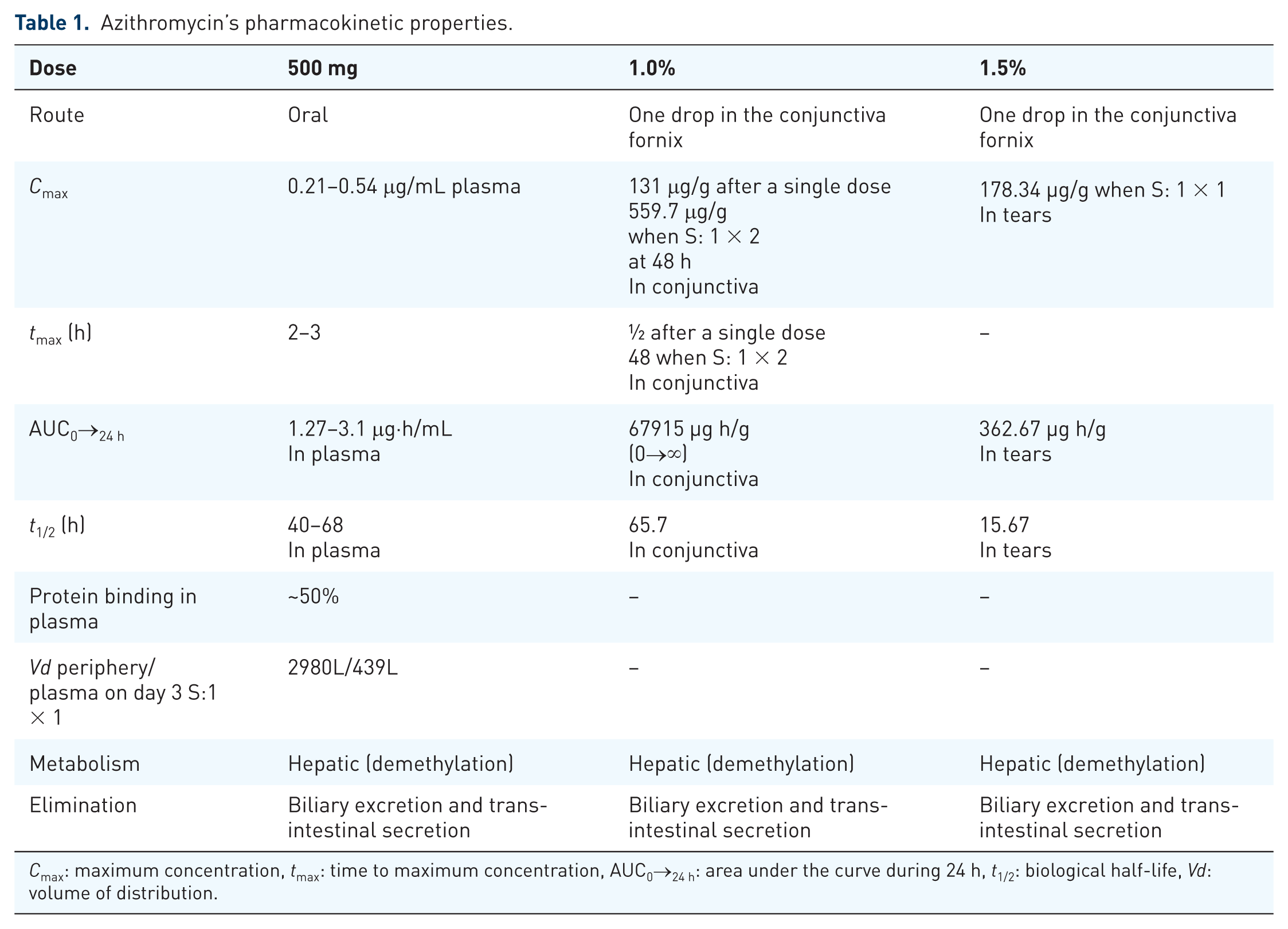
Cmax: maximum concentration, tmax: time to maximum concentration, AUC0→24 h: area under the curve during 24 h, t1/2: biological half-life, Vd: volume of distribution.
Its absolute oral bioavailability extends to 35–42% in healthy individuals and people suffering from cystic fibrosis and its extensive uptake in tissues (10- to 100-fold higher than mean serum concentrations) principally contribute to its extended half-life. 2 The widespread location of fibroblasts renders them to be considered as a reservoir for AZM, which also accumulates to other cells such as epithelial cells, hepatocytes, and phagocytic cells (polymorphonuclear leukocytes and macrophages). Intracellularly, it is localized in lysosomes. 4 Phagocytes accumulate high amounts of AZM, up to 200 times higher intracellular than extracellular concentrations. This the main reason of high AZM’s accumulation in the site of inflammation. There are two mechanisms of AZM’s delivery to the site of infection. In the first mechanism, AZM is directly uptaken by tissues, mainly by fibroblasts and phagocytic cells, while in the second, the drug is released during phagocytosis to achieve high concentrations in the exact site of inflammation.3,4,6 AZM penetrates poorly cerebrospinal fluid and peritoneal fluid but crosses the placenta.2,3
After topical installation of an ophthalmic solution of AZM (1.0% or 1.5%), the drug is not detectable in the blood of patients at the applauded dose (detection limit: 0.0002 µg/mL of plasma). It achieved persistent concentration in tissues above MIC90 in ocular surface and eyelids. Half-life of topical administration is equivalent to its systemic administration (approximately 65.7 h). But a sole dose of AZM 1.5% ophthalmic solution in healthy volunteers had a mean elimination half-life of 15.67 h. The pharmacokinetics of AZM ophthalmic solution appear to be dose dependent. Interestingly, polycarbophil as an excipient raises the higher AZM’s concentrations in the lacrimal functional unit. This was attributed partly to the longer contact time.5,6 Topical administration achieved far less lower concentrations than the MIC90 in the aqueous humor, similar to the systemic administration of the drug. 7
AZM has demonstrated immunomodulatory and anti-inflammatory effects. It decreases NF-κB, IL-6, IL-8, 4 and MMP-2 activity, 5 while it increases TGF-β1. 8 Moreover, it reduces the main symptoms of ocular inflammation, conjunctival and lid redness and edema, mucous secretion, and macrophage infiltration. 9 In an acute cornea inflammation, it diminished the number of leukocytes, enhanced IL-10, and reduced the produced amount of TNF-α, IL-1β, and ICAM-1 in the site of inflammation. 10 AZM has been found to interfere in a lot of other inflammatory modulators [e.g. MMP-1, 9, 10, and 13; GM-CSF; MAPK kinase (ERK, JNK, p38); GRO-α; MPO; AP-1; IL-12; CD40; and CD86 of MIC II, COX-1, and COX-2]. 5 Because of the augmented levels of the previous immune modulators, AZM might have a noteworthy role in chronic inflammatory ocular disorders. Finally, sustained concentrations of AZM may provoke a gradual bactericidal outcome. 6 The molecule binds to the 50S ribosomal unit and inhibits the protein synthesis by blocking the assemblance of ribosomal unit. The enhanced efficacy against gram-negative bacteria is explained by the basicity of AZM, which enables proper dissemination through outer membranes. 5 It has been found to be active against staphylococci, streptococci (especially Streptococcus pneumoniae and Streptococcus pyogenes), Neisseria gonorrhoeae, Moraxella catarrhalis, Clostiridium perfringens, Escherichia coli, Salmonella and Shigella species, Haemophilus influenza, Haemophilus parainfluenzae, Pseudomonas aeruginosa, Legionella, Chlamydia spp., Campylobacter jejuni, Helicobacter pylori, Toxoplasma gondii, Cryptosporidium, and Plasmodium species, Mycobacterium avium-intracellulare, and Borrelia burgdorferi.1,6,9
A PubMed (National Library of Medicine) and a ScienceDirect search was conducted using the key phrases ‘azithromycin’, ‘meibomian’, ‘blepharitis’, ‘trachoma’, ‘toxoplasmosis’ from 2010 to 2017. Articles were limited to articles published in English or at least having an English abstract. There were no restrictions on age, ethnicity, or geographic locations of patients.
Blepharitis and meibomian gland dysfunction
Blepharitis, a chronic inflammatory disorder of the eyelids, is being commonly categorized into anterior and posterior. Anterior blepharitis refers to inflammation of the area surrounding the basis of the eyelashes and could be accompanied by squamous debris or collarettes, while posterior blepharitis is related inflammation of the meibomian glands and their orifices. It could be a consequence or the origin of meibomian gland dysfunction (MGD). Infectious or allergic conjunctivitis and rosacea are other common causes of posterior blepharitis. MGD is a diffuse disorder of the meibomian glands, causing prevention of their secretions, alterations in the quality of the tear film, and finally, increased tear evaporation, leading to dry eye. Even though posterior blepharitis and MGD are not identical terms, they are often inaccurately used interchangeably.11,12 Currently, there are no established therapeutic guidelines for either blepharitis or MGD, and most cases are addressed by eyelid hygiene, compresses and gland expression, lubricants, topical antibiotics, and steroids.11–15 Many recent studies have addressed the topical and systemic AZM’s place in therapy in blepharitis and MGD. Because of lack in understanding of the underlying mechanisms of blepharitis, and the fact that the role of bacterial colonization is controversial, 16 AZM’s anti-inflammatory, immunomodulatory, and broad antimicrobial characteristics propose this drug as a candidate in a new optimal treatment management (Table 2).
Comparison of clinical efficacy and safety of azithromycin versus other drugs for the treatment of the same disease.
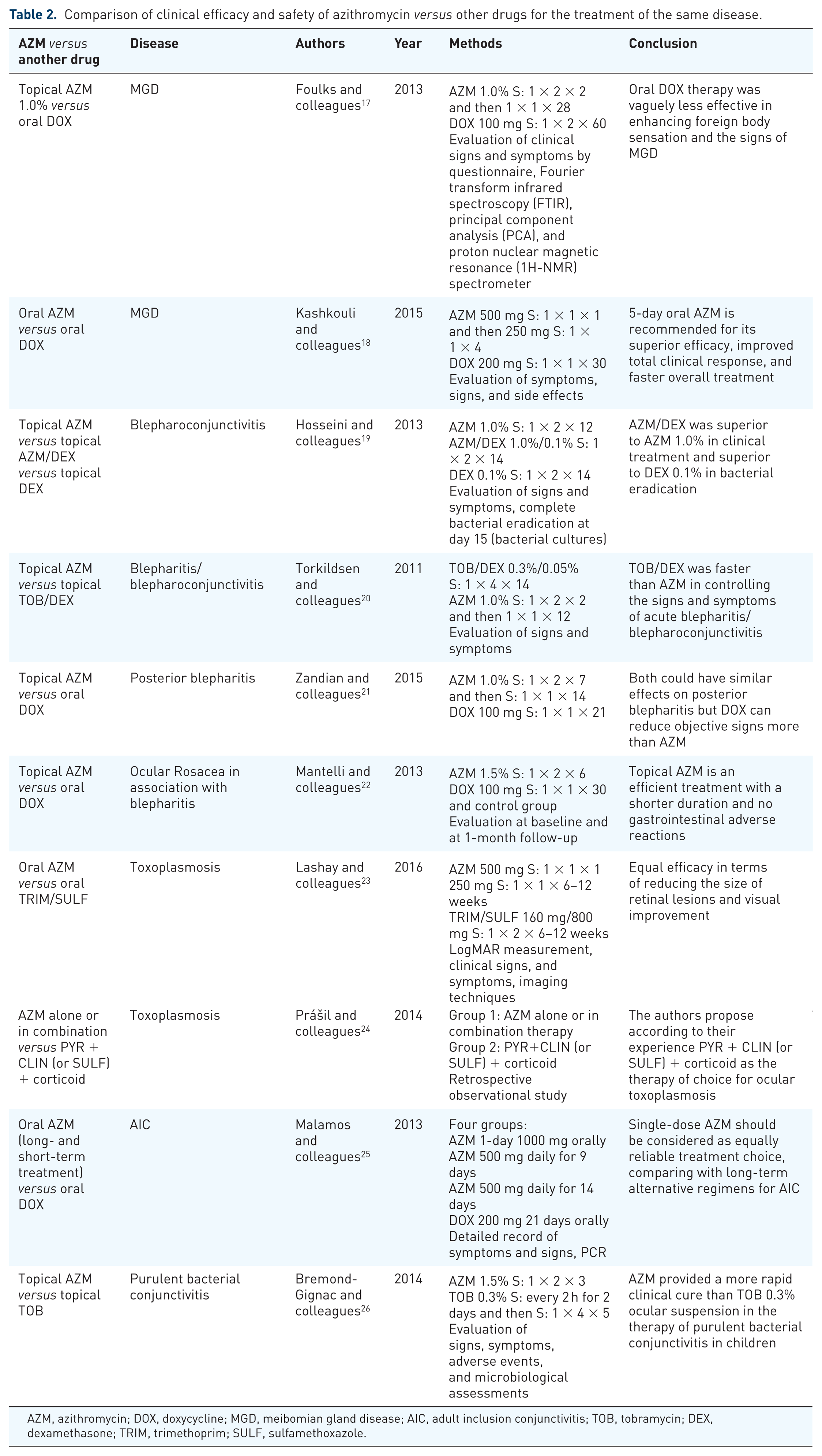
AZM, azithromycin; DOX, doxycycline; MGD, meibomian gland disease; AIC, adult inclusion conjunctivitis; TOB, tobramycin; DEX, dexamethasone; TRIM, trimethoprim; SULF, sulfamethoxazole.
The efficacy of AZM in blepharitis has been tested in different treatment protocols (Table 2). Treatment which lasted for 1 month seemed to be superior to shorter treatments. The treatment of chronic blepharitis with topical AZM 1.5% ocular suspension b.i.d. for the first 2 days followed by single administration each day for 28 days (Group A) versus for 12 days (Group B) demonstrated improved and more sustained outcomes in favor of Group A. Both groups were monitored before the beginning of their eyedrops administration, at the end of the accomplishment of each treatment protocol and 4 weeks later. In addition, Tear Break-Up Time (TBUT) values and Schirmer test were performed. 27 Similarly, Fadlallah and colleagues conducted a clinical study between two groups of patients suffering from moderate to severe blepharitis. Both groups were administered topical 1.5% AZM b.i.d. for 3 days and were instructed to perform lid hygiene twice daily (warm compresses and lid cleaning with soap), although Group II continued topical installation of AZM 1.5% only once every night for 27 more days. Patients’ signs and symptoms were documented and then sorted in accordance with severity. In conclusion, Group II showed better improvement than Group I. No safety issues were reported. 28 Moreover, after a month-long treatment with azithromycin 1.0% ophthalmic solution, blepharitis signs and symptoms were significantly improved, which persisted 4 weeks posttreatment. Eyelid margin culture exhibited significant decreases in microbial load but no changes were observed in tear cytokine concentrations. 29
As far as the AZM ophthalmic solution efficacy compared with other treatments for blepharitis/blepharoconjunctivitis is concerned (Table 2), recent research finds the combination of antibiotic plus a steroid in ophthalmic solution superior to the AZM drops alone, without severe adverse events. Specifically, in three groups of patients suffering from blepharoconjunctivitis and treated with AZM and dexamethasone (DEX) (Group I), 1.0% AZM (Group II), and 0.1% DEX, Group I was found superior to Group II as far as the treatment’s efficacy is concerned and superior to Group II in bacterial load suppression both deductions referring at results from day 15. Patients in Group I achieved a faster clinical resolution rate compared with the other two groups. Adverse events were equally distributed among the three study groups 19 (Table 2). Correspondingly, the combination of a topical AZM solution 1.0% with corticosteroid (DEX 0.1%) was found superior in the comprehensive treatment of blepharitis after 2 weeks. The combination was also found well tolerated. 30 In addition, the combination of another topical antibiotic solution (tobramycin, TOB) with corticosteroid was also found superior in the treatment of blepharitis/blepharoconjunctivitis. Namely, TOB/DEX ocular solution 0.3%/0.05% proved to be more efficacious at day 8 and reached quicker inflammatory relief than AZM 1.0% alone. Yet, the dosage scheme of eyedrops administration would be a worthwhile element to further evaluation of the above results as TOB/DEX was administered higher than the usual treatment dose (q.i.d. for 2 weeks) and AZM b.i.d. for 2 days and then once daily for 12 days. 20
Likewise, other two clinical studies proved the efficacy of AZM in the remedy of posterior blepharitis, while a third compared the clinical effects of oral doxycycline (DOX) to topical AZM and finds them similar. The administration of oral AZM 500 mg once a day for three subsequent days in three turns with a week gap between two successive turns and the administration of AZM 1.0% ophthalmic suspension b.i.d. for 2 days, then once a day in the evening a month-long, were found to be effective for the treatment of posterior blepharitis.31,32 Moreover, in the first half of patients treated with warm eyelid compress and massage three times a day for 3 weeks was administered AZM 1.0% ophthalmic solution b.i.d. for 1 week and then once a day for 2 weeks, and in the other half orally DOX 100 mg for 3 weeks. Even though both treatments relieved signs and symptoms after 3 weeks, topical AZM was found more efficacious in alleviating eye redness, while oral DOX proved to be more potent in decreasing corneal staining and in the cure of meibomian glands plugging 21 (Table 2). AZM is widely prescribed for MGD although it remains off-label, presumably to suppress the MGD-associated posterior blepharitis, the associated conjunctival inflammation, and growth of lid bacteria. Indeed, recent data widely support the use of AZM in MGD ± dry eye disease. AZM was found to have a direct effect on meibomian gland epithelial cells [human meibomian gland epithelial cell (HMGECs)] to incite their function,33,34 while the MGD treatment of choice, which is oral tetracyclines do not exhibit similar properties. 35 Topical AZM has been found effective in treating MGD 36 and slightly more effective to DOX in improving foreign body discomfort and the signs of plugging and secretion. 17 In addition, it may represent a synergistic treatment to oral DOX for ocular rosacea, and their combination may severely enhance the efficacy in treating MGD, as their mechanism of action may differ signifficantly.22,36 Oral AZM has been found preferable to the use of oral tetracyclines.18,37 More in detail, a retrospective case note audit in 11 patients (9 diagnosed with MGD/rosacea and 4 with dry eye syndrome) showed an important improvement in their symptoms (73%) and signs (82%) and no compliance issues. Because of our current poor comprehension of the fundamental mechanism of blepharitis, the previous percentages show a reasonable response in the treatment of MGD ± dry eye. Moreover, almost two thirds (73%) of these 11 patients had been administered oral tetracyclines in the past. With poor overall satisfaction because of the common reasons referring to tetracycline administration, such as severe side effects and compliance issues partly provoked by side effects and partly by long treatment’s duration. The 11 patients were administered 500 mg AZM per os once a day every day for only 3 days. For reasons of comparison, we shall notice the rather extended treatment period of tetracyclines (2–3 months). 37 Another study, a randomized double masked open label trial, proposed favorably a 5-day oral AZM (500 mg on the first day and then 250 mg each following day) in contrast to a month treatment with oral DOX, 200 mg per day. It was found that oral AZM had considerably fewer adverse effects and was more advantageous in improving the signs of the illness. As far as the symptoms were concerned, oral AZM also proved relatively better, as there was no statistical significance between the corresponding results. Besides, the total cost of remedy with oral AZM is notably decreased, as well as treatment’s duration, compared to oral DOX. 18
Finally, AZM has been proven effective against ocular rosacea, which is a comorbid condition of both blepharitis and MGD. Topical administration of AZM 1.5% eyedrops b.i.d. for 6 days was compared with the prescription of oral DOX 100 mg/day for 1 month and was found effective in the management of patients with ocular involvement in acne rosacea also providing less side effects (no gastrointestinal disturbances were reported). 22
Trachoma
Trachoma is a major cause of preventable blindness worldwide. The disease is caused by an intracellular epithelial gram-negative bacterium, Chlamydia trachomatis. The principal initial clinical manifestation is a follicular conjunctivitis that may lead to conjunctival scarring, entropion, trichiasis, corneal thinning, and ulceration. Some patients develop corneal scars that lead to loss of vision. 38 AZM’s very good safety profile without any serious side effects in combination with its relatively unique pharmacokinetic properties enables high efficacy only by a single oral dose, particularly in bacteria of specific interest, such as against C. trachomatis, rendered it the drug of choice against trachoma. By contrast, the other three most likely treatment alternatives, which are tetracyclines, erythromycin, and sulfonamides, while effective, share severe disadvantages. Explicitly, they require long duration of drug administration and demonstrate severe side effects. Tetracyclines are contradicted in children, which is the dominant age group suffering from trachoma, and sulfonamides are related to Stevens–Johnson syndrome. Moreover, the above lead to poor compliance, which rises the percentage of treatment failure. 39
Contemporary World Health Organization (WHO) guidelines recommend mass treatment to eliminate follicular trachoma in endemic areas (prevalence 10% or more in children 1–9 years old) by administering a single dose of AZM in everyone over 6 months (MDA, Mass Drug Administration) for a minimum duration of 3 years and suggested coverage at least 80%. 39 It has been estimated next to 3–7 years of MDA every year in 71 formerly hyperendemic populations in Tanzania that, for populations with initiating trachoma prevalence of 50% and treatment coverage of 75% each year, minimum 7 years were indispensable to achieve prevalence of less than 5%. In addition, they found: (a) a linear relationship between prevalence of clinical trachoma and years of treatment and (2) no populations afterward 3 years of treatment had reached the WHO goal of <5% prevalence of follicular trachoma. 40 Even in populations with baseline follicular trachoma prevalence of 20% or more, there was no proof to cease MDA prior to the accomplishment of the first three annual administrations. 41 As a matter of fact, a report from a cross-sectional prevalence survey that was performed in the trachoma endemic Car-Nicobar Island reports that the disease has not been abolished from the study population in accordance with the current WHO recommendations after three annual MDA. 42 This suggests the imperative value of uninterrupted, prolonged programs in hyperendemic districts.
Moreover, increasing coverage to over 90% did not seem to provide any further benefit. 41 However, it has been calculated using a mathematical transmission model that there is an 89% [standard deviation (SD) 5.6%] possibility of trachoma elimination, provided a prolonged (10 years) and 95% coverage of MDA yearly. When coverage levels of 90%, 80%, 70%, and 60% were assumed, we found the probability of elimination was 81.8% (SD 8.8%), 59.6% (SD 14.8%), 34.7% (SD 17.5%), and 16.4% (SD 14.3%), respectively. Using the same model, it was estimated that the effective field efficacy of antibiotic in an individual to be 67.6% [95% confidence interval (CI): 56.5–75.1%]. 43 Here, it should be noted that after MDA, nasopharynx bacteria cause signs of TF (follicular trachoma), affecting the interpretation of impact surveys. 44
It may seem logical that the frequency of medication administration correspondingly influences the rate of elimination, but there are no supportive data available. Biannual treatment may accelerate elimination endeavors but does not affect prevalence after a few years. 45 From another study was reported that biannual treatment of children was noninferior to drug administration once a year in the whole community. 46 Missing an annual MDA is a risk factor [odds ratio (OR) 2.49, 95% CI: 1.02–6.05] for chlamydial infection in endemic aerias. 47
The need for recurrent annual MDA in endemic arias evokes the question of AZM efficacy pitfalls. However, no relevant evidence has been found.47,48
Recently, there was a lot of interest in using eyedrops of AZM instead of oral AZM in treating trachoma in endemic areas. In 2010, Amza and colleagues 49 reported that AZM 1.5% ocular suspension was viable, safe, and effective to treat massively active trachoma. A longitudinal cohort study was conducted to determine for the first time the role of a single cycle of topical AZM in preventing long-term trachoma complications in children from an area with endemic trachoma. About 1.5% AZM ocular solution was administered b.i.d. for 3 days and were followed up for 3 years. None of the patients developed trachoma-related ocular complications during the study period. 50 In conclusion, a single cycle of topical AZM could be possibly used as an effective and safe option for treating active trachoma in children in endemic areas and also prevents trachoma-related ocular complications.
Toxoplasmosis
Ocular infection by the protozoan T. gondii is the most common origin of posterior uveitis, typically manifested by retinochoroiditis. In our therapeutic armamentarium stand primarily pyrimethamine and sulfadiazine. When sulfonamides are contradicted, for example, in patients with hypersensitivity, pyrimethamine is used in elevated doses or is used in combination with clindamycin, clarithromycin, AZM, or atovaquone. Other various combinations, including spiramycin, AZM, trimethoprim plus sulfamethoxazole, atovaquone, tetracycline, and minocycline, are also commonly used.51,52 No evidence is available to prove the superiority of any antibiotic regimen, so any choice needs to take highly into consideration its safety profile. 53
To ameliorate the treatment of ocular toxoplasmosis, there are a lot of issues to be addressed. Toxicity remains to be decreased and so the minimum therapeutic concentrations in the brain and eye. Total treatment’s duration is still too long and very expensive for use in deprived areas of the world and tissue cysts still need to be effectively eliminated. Finally, there are still considerable burdens to overcome concerning the safety in pregnancy. 54
AZM was found to be an acceptable alternative to trimethoprim/sulfamethoxazole in terms of reducing the size of retinal lesions and improving vision. 23 Pyrimethamine and AZM in comparison with pyrimethamine and sulfadiazine were of similar efficacy, but the safety profile (frequency and severity of side effects) was significantly better in the regiment which contained AZM. 55 Likewise, the triple combination of trimethoprim/sulfamethoxazole and AZM was found safe, effective, and it seemed to hasten the resolution of inflammation. Both inflammation’s clinical manifestations and its overall recession seemed to be accelerated. 56
On the other hand, another study finds pyrimethamine + clindamycin (or sulfadiazine) + a corticoid superior to AZM or a combination of AZM with a corticoid or a corticoid alone. 24 A case report states a patient who was primarily administered per os pyrimethamine, sulfadiazine, AZM, and prednisolone without any success. However, he responded dramatically good to intravitreal clindamycin (1 mg/0.1 mL). 57
In a mouse study, AZM in combination with Chlorella vulgaris, which is a single-cell green algae, seemed to be an effective treatment option than AZM alone, particularly in patients who are difficult to treat with common methods or in patients with immunosuppression. 58
A recent retrospective clinical study concludes that during pregnancy, postpartum period, or lactation, any remedy must be addressed individually, directed by the gestational age and the location of the active lesion. To sum up, possible treatment options are as follows: pyrimethamine 25 mg/sulfadoxine 500 mg (Fansidar) and prednisone, topical steroidal or nonsteroidal ocular solution, and spiramycin or AZM per os. 59 Acetyl spiramycin in combination with AZM was also found clinically effective in the treatment of pregnant toxoplasmosis. 60
SPAf, which is a combination of AZM (300 mg/kg), pyrimethamine (100 or 50 mg/kg), sulfadiazine (100 or 75 mg/kg), and folinic acid (15 mg/kg), was reported to be less effective than AZM alone in treating rodents infected with T. gondii. In females, AZM reduced the number of the pathogenic protozoa in the brain, and no protozoa were detected in the eyeballs of their fetuses in contrast with the SPAf group where parasites were found in the fetuses’ eyes, suggesting the high potency of AZM as a different treatment option for toxoplasmosis during pregnancy. 61 In addition, it was found that treatment of human trophoblastic BeWo cells with AZM could regulate effectively the infection and replication of parasites. 62 AZM was also found an effective alternative drug of pyrimethamine, sulfadiazine, and folinic acid to control T. gondii infection in human villous explants, at the fetal–maternal interface. 63
Other diseases
AZM can be very helpful in treating human ocular pythiosis. Antibacterial administration alone completely resolved pythium keratitis of a patient- the first case successfully managed nonsurgically. The patient’s treatment consisted of topical AZM 1.0% ocular solution and topical linezolid 0.2% ocular solution both every hour, topical atropine sulfate ocular solution every 8 hours and oral AZM 500 mg once a day for 3 days each week, recurrently until resolution of growing lessions. 64 In an in vivo study, synergistic interactions were optimized with a combination therapy of AZM/minocycline and AZM/clarithromycin against Pythium insidiosum. Moreover, AZM seemed effective in treating subcutaneous pythiosis in an animal model. 65
Apart from ocular pythiosis, it was found in a three-dimensional (3D) corneal tissue model that AZM and DOX may be effective adjuvants to standard antiacanthamoebal chemotherapy 66 and AZM was effective in complete resolution of keratitis caused by susceptible strains of P. aeruginosa. 67 AZM was reported as a viable option for treating ocular bartonellosis. 68 Parenteral and oral cephalosporin and AZM therapy leaded to complete recovery of a patient suffering from purulent keratoconjunctivitis due to N. gonorrhoeae and C. trachomatis coinfection. 69 A single-dose AZM of 1000 mg has been proved efficient in treating patients with adult inclusion conjunctivitis (AIC). It showed equal efficacy with extensive treatment regiments of oral AZM and oral DOX. 25
Topical 1.5% eyedrops of AZM were found to be effective in treating phlyctenular keratoconjunctivitis complicating childhood ocular rosacea. 70 Also, topical 1.0% AZM eyedrops were effective in the acute management of middle to severe inflammatory pterygium. In case of grave inflammation of the eye, topical steroids or any other potent anti-inflammatory therapy may be needed. 71 AZM 1.5% eyedrops provided a faster treatment than topical TOB 0.3% ocular solution regarding purulent bacterial conjunctivitis in children, with a more suitable b.i.d. dosing plan for 3 days instead of a 7-day treatment with TOB. 26 In patients suffering from contact lens–related dry eye, a notable extension in subjective pleasant contact lens usage durability was reported throughout the period of the clinical trial (4 weeks). However, total wear time, low contrast visual acuity, or tear osmolarity were found without any significant variations. 72
Topical AZM drops have been proposed to be used instead of fluoroquinolones before corneal cross-linking by UV light because fluoroquinolones are known to be phototoxic to the skin and lens. These effects may contribute to some of the procedure’s complications. Corneas treated with AZM before UV radiation showed normal histology, no staining for apoptosis, and no increased production of apoptosis markers by polymerase chain reaction. 73 Finally, AZM was proposed as an alternative immunosuppressant agent with broad spectrum antibiotic properties in combination to glucocorticoids after routine lamellar and perforating corneal transplantation. This could allow the dosage of steroids to be reduced, avoiding commonly occurring adverse reactions as lens opacification and escalation of the intraocular pressure. 74
Safety and tolerability
AZM ophthalmic solution is well tolerated. Its most frequent side effects were correlated to ocular discomfort, burning, itching, and stinging upon installation. Headache and eye pain were also reported. Frequencies of each previous adverse event are less than 2%. However, frequencies of adverse events increase when treatment protocols outrun 14 days. Then ocular discomfort reached 15%, hazy vision 5–15%, ocular irritation 2–5%, itching 4–8%, ocular discharge 4%, and burning 4%.4,9
Oral AZM is also well tolerated. Nevertheless, it often causes gastrointestinal disturbances, headache, and dizziness and in 1.5% of patients raised transaminases. More serious incidents are hearing loss and QT prolongation. QT prolongation may result to death in specific circumstances. Hearing loss has been observed in a diminutive percentage of individuals but there are case reports to confirm this severe side effect after short-term administration of oral AZM.3,75
A recent systematic review and meta-analysis to evaluate the effect of AZM on risk of death found that contemporarily suggested dosing (within 1–5 days of treatment) was related to greater risk of death among the elderly with mild degree of heterogeneity [hazard ratio (HR) 5: 1.64 (95% CI: 1.23–2.19), I2 = 4%] in contrast to younger population [HR 5: 0.85 (95% CI: 0.66–1.09), I2 = 0%]. 76 A large retrospective cohort study of patients prescribed a 5-day course of AZM found that cardiovascular deaths increased compared with ciprofloxacin, amoxicillin prescription, or lack of any drug administration. 77 The previous study was based on the evidence that AZM may lengthen the QT interval, which is a principal risk factor for torsades de pointes, arrhythmias, uncompensated heart failure, congenital long QT syndrome, or other relevant diseases. AZM was much safer than either erythromycin or clarithromycin, as it causes QT prolongation to a lesser degree.2,3,78 Several other studies disagree with the results of the previous study. According to a nationwide cohort study conducted in Denmark, there is no increased risk of cardiovascular death of current AZM use relative to penicillin V in young and middle-aged adults (rate ratio 0.93, 95% CI: 0.56–1.55), 79 according to a systematic review of 12 randomized controlled trials, there is no increased risk for mortality or for cardio-vascular events related to AZM treatment in contrast to placebo, 80 and, according to a large observational study including more than 70,000 individuals, there is no increase in arrhythmias. 81 But still, the evidence about AZM’s cardiovascular safety is inconsistent. AZM can affect cardiac function; however, cardiovascular side effects have been mainly observed in patients already suffering from cardiac illnesses. So, awareness in AZM’s prescription is justified in patients with pre-existing QT prolongation or risk factors for it, such as hypomagnesemia, hypokalemia, and co-administration of other drugs causing QT prolongation.2,82
Consequently, greater awareness of the co-prescription of AZM and other drugs prolonging the QT interval is paramount. Special consideration should be taken to possible interactions after the cessation of AZM’s administration, for the reason that long half-life characterizes the latter. Clinically significant drug interactions include warfarin—excessive anticoagulation, everolimus—reduces its clearance, digoxin (AZM may potentiate its toxicity), colchicine (AX< may increase its concentrations), statins (AZM may increase the risk of rhabdomyolysis), and antacids (aluminum, magnesium), which may decrease the highest achieved concentration of AZM.3,83
To summarize, a study associated AZM with the inducement of acute myocardial infarction but was severely criticized because its group of patients generally suffered from higher comorbidity. 82
Resistance
Resistance genotypes in macrolides exhibit variant spread between and within different countries. Resistant strains of bacteria to AZM increase with AZM use. 5 In children, who participated in a cluster-randomized clinical trial, the mean prevalence of resistant S. pneumoniae strains after MDA escalated from 3.6% at baseline (95% CI: 0.8–8.9%) to 46.9% (95% CI: 37.5–57.5%) after a year (p = 0.003).The above results are fully compatible and attest the broadly acknowledged theory: the more susceptible bacterial strains are eliminated due to antibiotic administration, the more rapid is the expansion of the possibly remaining resistant strains. 84 Moreover, in another study, the percentage of resistant to macrolides nasopharyngeal S. pneumoniae strains reached the high percentage of 76.8% (95% CI: 66.3–85.1%) in Ethiopian children (1–5 years old) following 6 biannual MDA of AZM to eliminate trachoma. Interestingly, resistance declined to 30.6% (95% CI: 18.8–40.4%, p < 0.001) and to 20.8% (95% CI: 12.7–30.7%, p < 0.001), correspondingly after a year and after 2 years subsequently to the accomplishment of the final drug administration. The key deduction of this large study was that macrolide resistance subsides afterward the interruption of antibiotic administration, which is by far hopeful regarding apropos of the current WHO strategy to eliminate trachoma. 85
Intense antibiotic use is well known to promote the proliferation of existing resistant bacterial strains. Generally, ‘survival of the fittest’ against macrolides suppresses outcomes in the basis of the following pathways: activation of an active pump mechanism to extrude the drug’s molecule; alterations in key metabolic pathways such as chromosomal mutations modifying a 50S ribosomal subunit protein, found mainly in Campylobacter species, Bacillus subtilis, mycobacteria, and gram-positive cocci; and methylase conferring resistance by the expression of erm(A), erm(B), erm(C), which leads to the production of methylase enzymes that alter the receptor resulting in considerably lower ligand-binding affinity. Another mechanism refers the rapid drug’s degradation by esterases produced by Enterobacteriaceae, which hydrolyze the drug’s molecule, thus resulting in loss of its potency.1,86 Strains that are inherently resistant to AZM include Corynebacterium spp., Enterococcus faecium, P. aeruginosa, and Acinetobacter. 9 In a recent study on commensal Staphylococcus aureus in European countries, apart from penicillin, it was found that AZM exhibited the maximum documented resistance (from 1.6% in Sweden to 16.9% in France). 87 As usage of AZM has increased, resistance is simultaneously developing in various subjects. Therefore, AZM should be prescribed in the setting of all related situations, nonetheless with particular concern due to its values and jeopardies, which is, of course, a general consideration that applies to the prescription of every antibiotic. 5
Conclusion
AZM is a one of the safest antibiotics, well tolerated, and has special pharmacokinetic properties. Moreover, it has a broad antimicrobial spectrum. AZM is efficacious for the treatment of a lot of ocular diseases and may be included as monotherapy or in combination therapy in new treatment protocols for more ocular infections. However, more research is needed to determine this.
Footnotes
Conflict of interest statement
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by the Private Practice Trust Fund of the Townsville Hospital, Queensland, and by James Cook University.