
Abstract
Background
Acute confusional migraine (ACM) is a rare migraine variant, primarily documented in paediatric populations. Its presentation in geriatric patients is extremely rare and can mimic acute ischemic stroke.
Case
We report on an 84-year-old male presenting with acute hemicrania followed by confusion and dysarthria. Despite initial systemic thrombolysis for suspected stroke, symptoms only resolved after sleep. Extensive diagnostics were unremarkable, leading to the diagnosis of ACM based on a 20-year history of stereotyped attacks.
Conclusion
This case represents the oldest reported patient with ACM to date. It highlights the importance of including ACM in the differential diagnosis of stroke mimics in the elderly to avoid unnecessary interventions.
Introduction
Acute confusional migraine (ACM) is a rare subtype of migraine. Due to its infrequency, it has not yet been included as a distinct entity in the International Classification of Headache Disorders-3 (ICHD-3).1–3 As a unique state of confusion flanked by juvenile migraine, the clinical picture was first described by Gascon and Barlow in 1969 and after further cases eight years later introduced into paediatrics as an independent clinical picture under the term ACM by Ehyai and Fenichel.4,5 Due to its rare occurrence in adulthood, ACM was initially thought to be a purely paediatric condition. However, in recent years, reports of ACM in adults have been increasing – currently up to the age of 62 years.6,7 The characteristic features of ACM are a migraine-like headache, followed by confusion in the sense of a qualitative change in consciousness, which lasts for up to 72 h and is completely resolved after a longer period of sleep. Occasionally, visual (32.5%), sensory (19%) or speech and motor symptoms (39%) may also occur. 8 Diagnostic workups typically yield no pathological findings in laboratory tests, cerebrospinal fluid (CSF) analysis, or morphological imaging. During an ACM attack, occasional transient cerebral hypoperfusion may occur on single photon emission computed tomography or frontal intermittent rhythmic delta activity on electroencephalography.9,10 As the disease is self-limiting, there is no established acute therapy; however, valproate and topiramate have been used with varying success for prophylaxis. 10
The aim of this case report is to highlight that ACM can manifest in geriatric patients ‒ potentially as a stroke mimic ‒ and to discuss the diagnostic challenges amidst the differential diagnosis of acute confusion. This study is reported in accordance with the CARE guidelines for case reports.
Case report
An 84-year-old male was admitted to the Emergency Department due to the acute onset of confusion and dysarthria, which developed within 10 min following the onset of left-sided hemicrania. The patient's wife contacted emergency medical services due to the acute and distressing nature of the symptoms; specifically, the severe dysarthria and prominent confusion were highly alarming. Because of his acute confusion, the patient was unable to communicate his medical history, prompting the emergency team to follow standard stroke protocols. Given the sudden focal deficits, a stroke was suspected. Initial stroke imaging, including computed tomography (CT) and CT perfusion, as well as laboratory diagnostics, was unremarkable. However, due to the functionally relevant deficit (National Institutes of Health Stroke Scale - 4) and the presentation within the therapeutic time window, systemic thrombolysis was administered. Despite the i.v. thrombolysis, there was no clinical improvement within the first 12 h. The patient remained disoriented to time, place, and situation. He exhibited pronounced motor restlessness and agitation, necessitating temporary restraint to prevent self-harm. No further focal neurological deficits were identified. Interestingly, after eight hours of sleep, the patient made a full recovery. Upon awakening, he was calm and fully oriented. Figure 1 shows the time course of prodrome, acute phase and resolution.
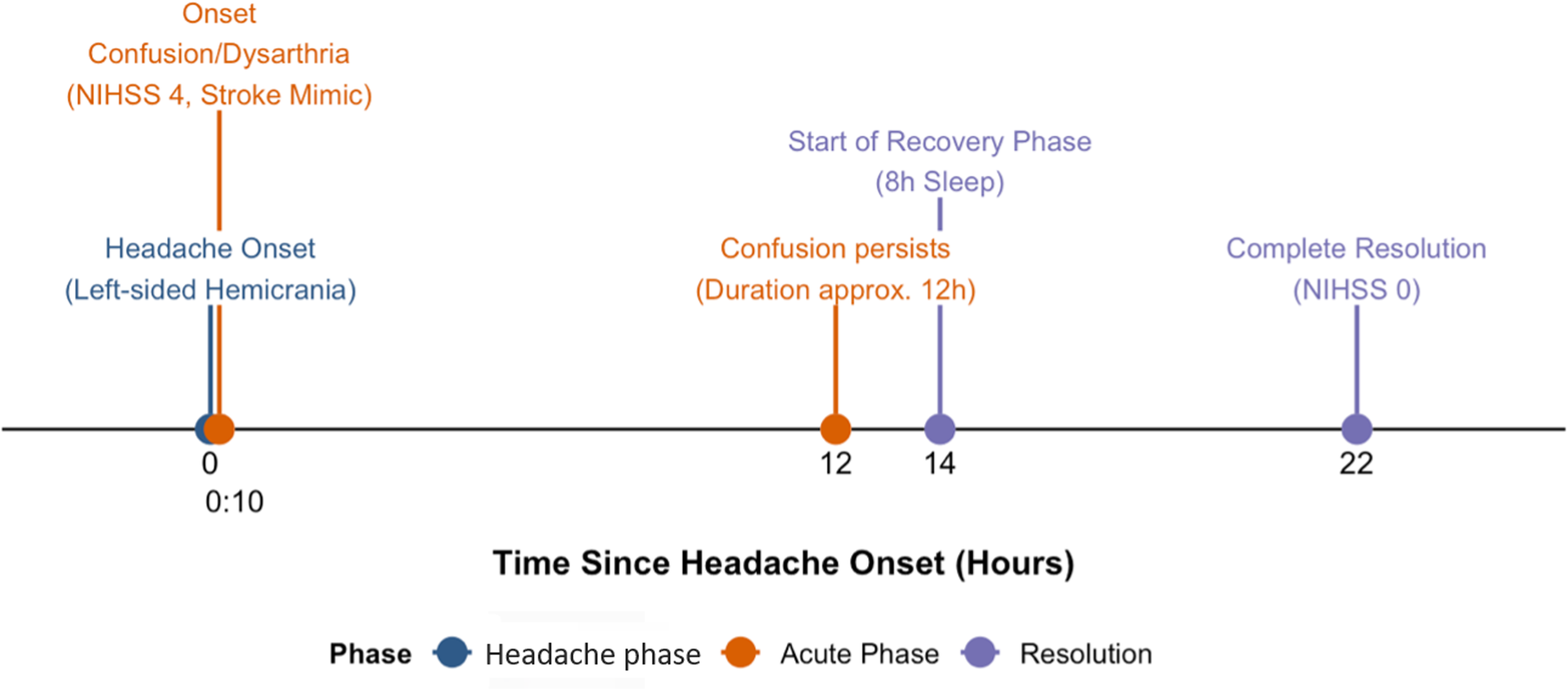
Schematic overview of the time course since headache onset in hours with headache phase (blue), acute phase (orange) and resolution (purple).
Both the patient and his wife reported a history of similar episodes spanning over 20 years. The first episode occurred when the patient was approximately 64 years old, representing a notably late onset for migraine. Childhood stomach issues or similar symptoms pointing to an early onset were not reported. Cognitive function was exceptionally good between episodes, with full orientation at all times. The semiology was consistent: Symptoms typically began with a left hemispheric headache, described as pulsating and accompanied by mild photophobia and nausea, without phonophobia or vomiting. Following this headache phase, approximately 10 min later, a qualitative change in consciousness and dysarthria emerged, primarily observed by his wife. Over the past two decades, the frequency of these specific ACM attacks has been approximately 1‒2 times per year. The patient did not report experiencing isolated migraine attacks without the subsequent confusional phase. These episodes of confusion generally persisted for 12–14 h and, along with the headache, resolved completely after an average of 8 h of sleep. The patient's medical history was otherwise significant for a prior cholecystectomy and prostate carcinoma. A review of the patient's medical records confirmed recurring admissions with identical symptoms dating back to 2009. Over five documented hospitalizations (2009, 2018, 2019, 2023, and 2024), initial working hypotheses included micturition syncope, meningitis, and migraine with atypical aura. Extensive diagnostic evaluations during these stays ‒ including CSF analysis, brain magnetic resonance imaging (MRI), extra- and transcranial Doppler/duplex sonography, electroencephalogram, and comprehensive laboratory panels ‒ yielded no pathological findings. Consequently, specific diagnostic formulations were previously abandoned in favour of descriptive diagnoses. During the current hospitalization, repeat cranial MRI, EEG, vascular ultrasound, long-term monitoring, and extensive laboratory diagnostics again revealed no pathologies. Based on the clinical presentation and exclusion of other causes, a diagnosis of ACM was made. We recommended prophylactic treatment with topiramate or valproate, therapeutic options the patient had not yet trialed. He was discharged in a fully recovered state (Figure 1).
Conclusion
Diagnosing ACM poses a significant challenge, particularly in the geriatric population where the differential diagnosis for acute confusional states is broad. Clinicians must carefully distinguish ACM from critical conditions such as acute ischemic stroke, transient ischemic attacks, non-convulsive status epilepticus, and metabolic or infectious encephalopathies, including Delirium. Delirium is often a primary consideration in elderly patients presenting with acute confusion. However, in our case, comprehensive diagnostic workups ruled out infectious, metabolic, toxic, and non-convulsive epileptogenic causes. Furthermore, the highly stereotyped nature of the episodes over 20 years, the preceding unilateral headache, and the rapid, complete resolution after a period of sleep are highly atypical for standard delirium but pathognomonic for ACM. Another crucial differential diagnosis is migraine with brainstem aura. According to the ICHD-3 criteria, this requires the presence of at least two fully reversible brainstem symptoms. A decreased level of consciousness in brainstem aura typically manifests as somnolence or stupor. In contrast, our patient exhibited hyperactive confusion, disorientation, and pronounced motor restlessness, which are cortical phenomena and the hallmark of ACM.
As illustrated in this case, ACM can present as a convincing stroke mimic, leading to acute interventions such as thrombolysis. The diagnostic complexity is compounded by the absence of ACM in the current ICHD-3 and the prevailing misconception that it is exclusively a paediatric condition. The pivotal factor in establishing the diagnosis in this case was the detailed medical history provided by the patient and his wife, revealing a stereotyped pattern of attacks over decades. This underscores the critical importance of hetero anamnesis in patients with transient confusion.
In conclusion, this case demonstrates that ACM is not limited to childhood and should be considered in the differential diagnosis of transient acute confusional states in elderly patients, provided that vascular, infectious, and metabolic causes are rigorously excluded. We advocate for the development of standardized diagnostic criteria for ACM and its formal inclusion in future iterations of the ICHD-3. Furthermore, increased awareness among neurologists and emergency physicians regarding adult-onset ACM is essential to optimize patient management and prevent unnecessary invasive treatments.
Clinical implications
ACM should be considered a potential stroke mimic even in the geriatric population.
Detailed hetero-anamnesis is the key to identifying long-standing stereotyped attack patterns.
Standardized diagnostic criteria and inclusion of ACM in the ICHD-3 are needed to improve diagnostic accuracy.
Footnotes
Ethical considerations
As this is a single case report involving standard diagnostic procedures, formal ethics committee approval was not required according to local institutional guidelines.
Consent to participate
Written informed consent was obtained from the patient for the publication of this case report and any accompanying images.
Consent for publication
The authors agree to publish with Cephalalgia Roberts, if the article is accepted.
Author contributions
The first two authors contributed equally to the article while the remaining five authors provided writing and editing support.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.