
Abstract
The WHO Intersectoral Global Action Plan (2022–2031) emphasises the importance of scaling up healthcare services to enhance access to care for patients with neurologic diseases. In Sub-Saharan Africa, most patients with neurological conditions, including headache, receive care in primary healthcare services. Here, they are often underdiagnosed and poorly managed, primarily due to the inadequate training of healthcare providers. Through its Regional Outreach Programme (ROPE), the International Headache Society (IHS) partnered with a local primary healthcare programme – the Disease Relief through Excellent and Advanced Means (DREAM) programme – to deliver two structured, in-person training courses to local clinicians in Blantyre, Malawi (in 2022 and 2025). These courses provided primary care providers with practical skills in diagnosing and managing primary and secondary headaches. The programme also included local field-based mentorship periods and a ‘train-the-trainer’ model. The training output indicates that partnerships between international scientific societies, such as the IHS, and established local healthcare programmes, like DREAM, facilitate effective task shifting among primary healthcare providers. This helps to bridge the huge diagnostic and treatment gap for headaches in Sub-Saharan Africa. ROPE represents a successful, replicable model for improving access to care for people with headaches in underserved regions.
Keywords
Introduction
The global recognition of neurology as a healthcare priority has been firmly established through the World Health Organisation's (WHO) Intersectoral Global Action Plan (IGAP) on epilepsy and other neurological disorders (2022–2031). 1 This initiative highlights the urgent need for action on non-communicable diseases (NCDs), drawing attention to the disproportionate burden of neurological conditions in low-income (LIC) and low-to-middle-income (LMICs) countries. 2 Headache disorders, particularly migraine, are leading causes of disability worldwide, 3 and Sub-Saharan Africa (SSA) is no exception, with migraine ranking among the most disabling conditions in the region.4,5
Despite this, access to headache care in SSA remains largely insufficient due to a critical shortage of neurologists and inadequate healthcare infrastructure. 6 Malawi, with a population of ∼22.2 million in 2025 and a very young median age (∼17 years), remains largely rural (> 80%) and lightly urbanized (< 20%), 7 is highly reliant on international aid – over half of its healthcare financing – and offers widespread, free public healthcare under its universal health coverage framework; however, gaps persist in financial protection and healthcare delivery.8,9 In this country, for example, only two adult neurologists serve the entire population. Hence, headache patients are mainly managed by general practitioners or, more often, by non-physician clinicians (NPCs, see Table 1), also known as clinical officers (COs) in Malawi, who often lack sufficient neurology training. 10
Meet the clinical officer.

In situations where academic education is only accessible to a very small proportion of the population due to financial issues and where part of the healthcare workforce is attracted abroad or to the private system, 11 there is a strong need for quality training initiatives aimed at equipping primary healthcare workers with the specific competences and skills required for headache management from diagnosis to treatment and prevention. Medication overuse headache, for example, is a major entity on the rise in SSA12,13 due to the combination of better wealth and better access to healthcare, as well as a near-complete lack of education or pharmacovigilance at the level of pharmacies, and so on. Therefore, quality training initiatives aimed at equipping primary healthcare workers would facilitate a transition from specialist-centred to NPC-centred headache care delivery, representing a crucial step in enhancing health coverage for this highly debilitating yet preventable neurological condition. Task shifting 14 refers to the redistribution of healthcare responsibilities from higher-trained specialists to non-specialist providers, and it has been shown to be effective in many areas of medicine.15–18 Headache medicine is amenable to a similar approach to bridge the existing access-to-care gap.
One of the International Headache Society's (IHS) main objectives is to provide high-quality education in headache management to a worldwide audience via different modalities (congresses, e-learning, visiting professorships, etc.). However, these initiatives may have limited penetration and impact at the primary care level, particularly in low-resource settings such as SSA. Hence, the idea is to develop bottom-up initiatives to promote neurology at the primary care level in collaboration with well-established local healthcare programmes that can provide insights, structures, local personnel, and a network to effectively deliver such education and training programmes.
Here, we present the promising outcomes of a multi-year headache education programme in Malawi, an SSA country, led by the IHS in collaboration with the Disease Relief through Excellent and Advanced Means (DREAM) programme, a local primary healthcare initiative.
Methods
For this initiative, the IHS and its Regional Outreach Programme (ROPE) partnered with the DREAM programme to deliver two structured in-person teaching and training courses in Blantyre, Malawi, in 2022 and 2025. DREAM has been active in SSA since 2002 (https://www.dream-health.org/). Initially created to address HIV care, it now operates in 10 SSA countries, integrating HIV care with that of other NCDs. More than 500,000 patients are under the regular care of local healthcare professionals, and since 2008, a telemedicine platform has enabled local clinicians to seek specialist advice remotely. 19 Continuous educational programmes for DREAM and governmental health-care providers are at the core of the DREAM programme and are aimed at expanding neurologic knowledge among non-specialist care providers, particularly NPCs (see Table 1). 10
Firstly, we ran a survey focusing on the main needs, experiences, and availability to participate in a training course among local clinicians attending other educational programmes in Blantyre. The vast majority work in the public sector and with local non-governmental organisations (NGOs). We then put together a faculty of IHS experts with a specific interest in African education, who worked together with DREAM governance to tailor the approach and create educational material that would equip COs with the fundamental skills needed for diagnosing primary headaches, understanding treatment principles, identifying red flags for secondary headaches, and to properly addressing the risk of medication overuse.
Two structured, in-person teaching and training courses were conducted. The first two-day course was delivered by IHS faculty members in 2022. The curriculum included foundational knowledge in headache medicine, with an emphasis on practical, case-based learning and interactive discussions. The second course was delivered in 2025 by a faculty that included five DREAM NPCs. These were selected based on successful completion of the first edition of the course and past education and practice in other neurological conditions, such as epilepsy and stroke prevention. This approach was well established in DREAM and was also used by the IHS-ROPE to foster peer-led education and the programme's sustainability within the local healthcare system.
The courses were designed to be highly interactive. The second edition also incorporated hands-on training, particularly in recognising secondary headaches and discussing clinical cases.
After the completion of the second course, two IHS neurologists (DM and ML) spent a week in the field in different DREAM centres to share daily work with the clinicians. Course participants were given opportunities to observe and engage in clinical practice alongside experienced neurologists. This component involved supervised patient interactions, allowing trainees to apply diagnostic and treatment principles in their actual healthcare settings. Observational assessments were conducted to gauge the effectiveness of training in clinical decision-making and patient management.
Participation in the courses was free of charge to all clinicians.
To assess the effectiveness of the educational intervention, we used a pre- and post-training evaluation test with 33 multiple-choice questions that covered (Supplemental Material 1):
Headache-related neuroanatomy. Neurological examination techniques. Diagnostic criteria for primary headaches. Secondary headache disorders and the differential diagnosis. Treatment principles and management strategies.
In addition, a structured feedback survey was administered to participants to evaluate the overall quality of the training sessions. These included assessments of content relevance, teaching effectiveness, and applicability to clinical practice.
Descriptive statistics were used to analyse the data with SPSS software. Pre- and post-course test scores were compared to assess knowledge acquisition. Median and standard deviation values were computed for each section of the test. A Shapiro-Wilk test was run for normality and, consequently, unpaired t-tests or Mann-Whitney tests were conducted to evaluate knowledge improvement comparing pre- and post-scores. A passing threshold of 60% was established for the test, reflecting the minimum level of knowledge deemed sufficient.
Additional qualitative feedback from course evaluations was analysed to refine future iterations of the programme and presented as an average of the scores.
Results
Baseline general survey
A total of 51 primary healthcare workers (23 women; median age 37 years; median education duration 3 years) participated in the initial survey, run in summer 2021. Of these, 26 were NPCs, six were nurses, five were physicians, and 14 had other roles. All of them provided care to patients at their healthcare facilities. All the healthcare workers agreed on the need to improve their headache education, yet 84% had never attended a headache course. During their graduation path, none had received formal neurology or headache training, except for very few lessons at the university, usually taught by senior NPCs.
As regards their experience with headache patients, they reported that only 2% of those patients are referred to doctors, while the majority are managed by NPCs (57%) or local healers (27%) (Supplemental Material 2).
Headache training courses
The first headache course took place in Blantyre, Malawi, in November 2022. This two-day course was attended by 34 NPCs (10 women; 24 men; median age 33 years) from both the DREAM programme and the Malawi Government healthcare services. Neurologists from Italy, Great Britain, Turkey, and Ghana delivered the training.
A second course was organised in February 2025. It lasted 3 days to meet the suggestions received during the first edition. Thirty NPCs participated, 17 were women with a median age of 37 years. Five of them had attended the previous course and were engaged as lecturers alongside IHS neurologists from Italy and Ghana.
Clinical experience and patient load
More than half (55%) of the participants worked in rural settings and had been practising medicine for a minimum of five up to more than 15 years; 62% of the participants saw over 100 patients daily. Before training, NPCs estimated that they encountered weekly 10–15 pure headache patients, probable primary headaches, including approximately five with migraine and fewer than two with tension-type or cluster headache. Participants also reported that in addition to primary headaches, up to 80% of their patients complain of headache in the context of other locally prevalent conditions as malaria, HIV, arterial hypertension, stroke, epilepsy, tuberculosis, hormonal contraception, and others, highlighting a critical need to improve their headache education. Due to limited training and pharmacological treatment options, clinicians also reported that ∼10.3% of patients turn to non-medical sources such as local healers, driven by frustration over the lack of effective and sustained headache care.
Knowledge assessment and improvement
Baseline assessments in neurology, anatomy, neurological examination, headache diagnostics, differential diagnosis, and management revealed substantial knowledge gaps. Median pre-course scores were 39.4% in 2022 and 45.5% in 2025, with no significant difference between editions. Post-training scores improved significantly, most notably in 2025, with a median increase of 18 points, compared to the initial evaluation (45.5%–63.6%, p < 0.001). Final scores in 2025 were also significantly higher than those in 2022 (median 63.6% vs. 50%, p = 0.017) since the improvement after the first course was more modest (from 39.4% to 50%, 11-point gain, p < 0.001).
In 2025, the greatest improvements were observed in neurological examination (from 67% to 83%, + 17 points, p = 0.015), diagnosis of primary (from 40% to 60%, + 20 points, p = 0.015) and secondary headaches (from 36% to 55%, + 18 points, p < 0.001), and treatment (from 50% to 67%, + 17 points, p = 0.001).
A score of 60% was established as the minimum threshold to indicate sufficient knowledge acquisition. In the second edition, 17 out of 30 participants (56%) achieved a post-training score above this threshold, compared to eight out of 34 participants (24%) in the first edition. Further details are presented in Figure 1.
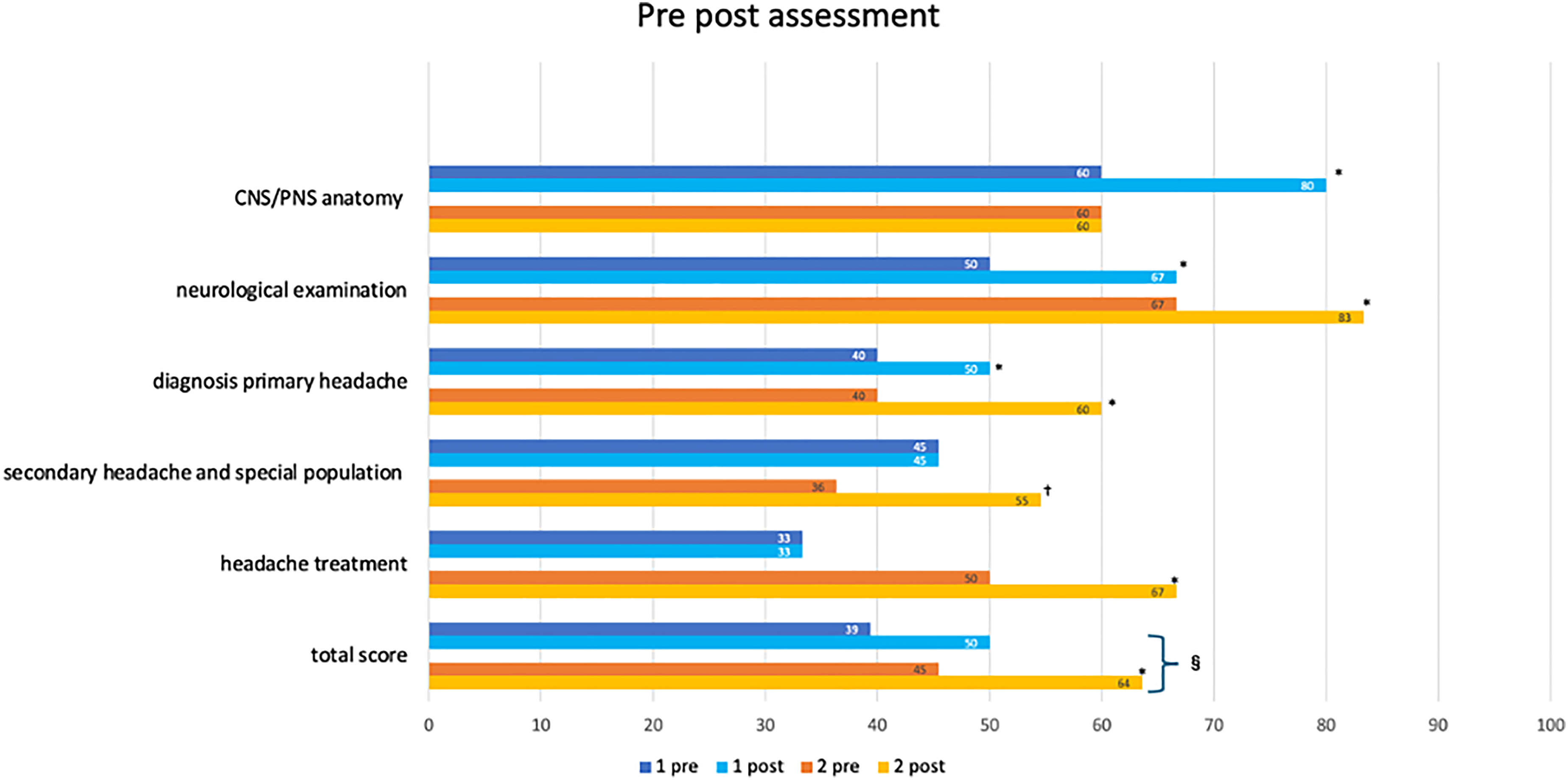
Results of a pre- and post-test, showing the median percentage scores achieved in the evaluation conducted twice, in 2022 and 2025, to assess the impact of the training courses. The displayed data represent the median percentage of correct answers achieved in each category before and after the course. Specifically, ‘1 pre' and ‘1 post' represent the median scores for the 2022 evaluation, while ‘2 pre' and ‘2 post’ represent the corresponding scores for the 2025 evaluation. No statistical difference was observed in general neurological knowledge or headache-specific knowledge before the course. In both the 2022 and 2025 editions, there was a statistically significant increase in the percentage of correct responses from the pre-test to the post-test (p < 0.001). This indicates that the course had a positive impact on overall performance in both editions. Following indications and feedback received after the first edition, the second edition was developed, which had a positive impact on several outcomes. The second edition demonstrated improved performance, with 56.7% of participants achieving a passing score of at least 60% (representing the minimum acceptable level of knowledge), compared to 25% in the first edition of the programme (p = 0.01). CNS = central nervous system; PNS = peripheral nervous system. †p < 0.05 from the t-test comparing the pre- and post-scores, for each single chapter. *p < 0.05 from the Mann-Whitney test comparing the pre- and post-scores, for each single chapter. §p < 0.05 from the t-test comparing the post score of the first vs the second edition of the course.
Participant satisfaction and feedback
Trainees expressed high satisfaction with the courses (overall score 4.6 out of 5 in both editions), valuing both the lectures and the practical insights provided. Following the first course, participants suggested extending the course duration and increasing the content on neurological examination and secondary headache disorders. These recommendations were implemented in the 2025 course. Many participants expressed a commitment to changing their clinical approach to headache patients. More details are available in Figure 2(A) and (B).
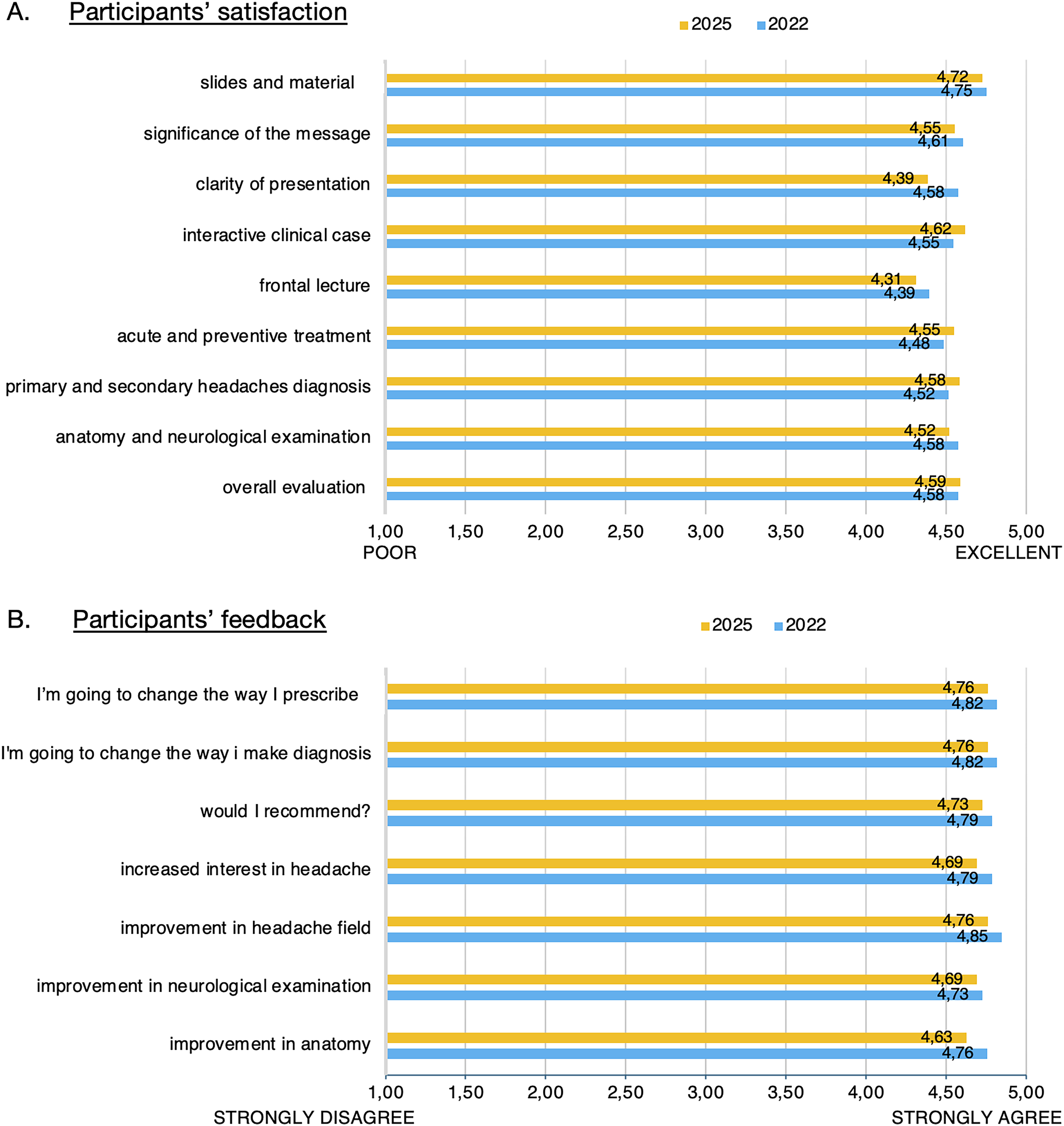
Participants’ satisfaction and feedback. (A) Evaluation of the quality of the two editions courses. 1 = poor; 5 = excellent. (B) Evaluation of the impact of the two editions of the courses. 1 = strongly disagree; 5 = strongly agree.
Discussion
Neurological care inequities represent a microcosm of broader health disparities, reflecting systemic failures in access, funding, and prioritisation. 20 Therefore, investing in primary care neurology is crucial because it ensures early diagnosis, timely intervention, and equitable access to treatment, particularly in low-resource settings. 21 This is important for a wide range of diseases that account for a significant proportion of disability across all age groups. Strengthening primary care yields has the greatest impact on reducing the global burden of neurological diseases, and aligns with WHO IGAP priorities. 2 Headache disorders are a leading cause of disability 3 and are underdiagnosed and undertreated in LIC-LMICs, particularly in SSA, where there are very few neurologists (e.g. in Malawi, in 2025, there are 0.014 neurologists per 100,000 inhabitants, in the context of a basic nationwide universal healthcare coverage), and the treatment gap for neurological conditions remains very high. 22 On the other hand, our programme's NCPs, before specialised training, conservatively estimated that only ∼10.3% of headache patients seek non-medical care. This figure contrasts sharply with the ∼50% subsumed use of traditional healers reported in broader LIC/LMIC mental health studies, 23 which often subsume neurological conditions like headache. This discrepancy likely reflects (i) framing and case-mix of patients attending the NCPs clinics, with headache often managed syndromically within HIV, malaria, tuberculosis, hypertension, or other high-burden conditions; (ii) clinician prioritization of life-threatening presentations, reducing detection/documentation of primary headaches; and (iii) patient reporting behaviour is shaped by system constraints (limited trained personnel for correctly identify the cases and scarce effective pharmacological options) and by local norms; in the absence of accessible, effective services, patients may not disclose headache or may pursue parallel care without telling clinicians. This under-reporting is supported by a recent primary-care study in Malawi, where >80% of people with HIV had headaches when systematically assessed, yet only a small minority had previously reported the symptom to their clinicians (Leone et al. 24 ; personal unpublished observations, available upon request). Finally, the reported lower rates are based on reports from biomedically oriented clinicians (course attendees). Accordingly, the 10.3% should be viewed as a conservative lower bound, underscoring the need for prioritising the primary care services with targeted training, dependable access to first-line acute/preventive therapies, and patient education that validates headache as a condition warranting assessment and follow-up.
NGOs can cover up to 50% or more of health and education services, especially in poor, remote SSA areas. 25 The encouraging results obtained with this initiative suggest that the partnership between scientific societies, which deliver high-quality education, and local NGO, providing structures, local personnel, networks, and resilient healthcare programmes for chronic disease, is instrumental in ensuring high-quality and contextually adapted training to primary care operators in SSA. By targeting the primary-care workforce, this initiative has the potential to effectively provide headache patients in regions where neurological expertise is poor and inequalities are huge at the primary care level.
The applied teach-learn-teach approach, involving the sequential delivery of two courses where the second was shaped by experience and feedback from the first, has been successful in improving competence and satisfaction among participants.
Although classroom-based education is very important, it must be reinforced through practical sessions. A key strength of the ROPE initiative has been providing follow-up to trained COs in their daily practice. Following the initial course in 2022, NCPs at DREAM centres in Malawi received five on-site visits from experienced neurologists, who spent several weeks each time, sharing daily work, visiting patients, and discussing cases with them. In addition, a tele-neurology system facilitates communication between local NCPs and remote neurologists, enabling local NCPs to access specialised teleconsultation. Another component of the continuous education process is web-based meetings.
Mentorship ensures that theoretical knowledge is sustainably translated into clinical competency and facilitates the integration of headache management with other highly prevalent conditions. Observing and guiding trainees in real-world settings strengthens their ability to independently manage headache disorders independently and fosters confidence in decision-making.
Integrating trainees into the faculty is another strength of the IHS-DREAM approach, consolidating its sustainability and enabling education to be scaled up to other geographic areas over time.
The two teaching and training courses delivered are probably insufficient to optimally manage the disease for everyone in need, as other aspects of care (e.g. the availability of disease-specific drugs and neuroimaging) cannot be addressed through training alone and require more extensive and structured collaboration with local and international stakeholders. However, this endeavour will certainly improve healthcare delivery for a large number of people suffering from headaches, given that the trainees serve a population of 90,000. Importantly, the DREAM education approach, based on regular visits by voluntary neurologists to share daily work with local NPCs, will ensure that what the trainees learned during the courses can be retained and further refined. Additionally, the teleconsultation system enables local clinicians to maintain continuous communication with remote specialists. Overall, this approach greatly increases the resilience of the knowledge and skills delivered through short, standalone courses.
Recognising that training courses alone are insufficient for advancing headache medicine in LIC-LMIC, IHS has implemented multiple initiatives. The organisation's commitment to establishing a global framework for headache medicine is evident through its collaborations, educational initiatives, and advocacy for equitable access to neurological care and effective treatment. Within this framework, the IHS has developed simplified yet evidence-based practice guidelines based on a two-tier approach – essential versus optimal – that enables adaptation to various resource settings.26,27 This ensures that, even in the most constrained environments, healthcare providers can make informed clinical decisions. Other initiatives are ongoing and their out will be soon available (see e.g. https://www.who.int/groups/expert-committee-on-selection-and-use-of-essential-medicines/25th-expert-committee-on-selection-and-use-of-essential-medicines).
Conclusion
Promoting headache care at a primary care level through task shifting represents an effective strategy for expanding access to care in LIC-LMICs.
Partnerships between international scientific societies and local healthcare providers may be a sustainable model for effectively implementing this approach, as academic institutions alone cannot address this need. These collaborations can utilise the expertise, resources, and networks of international societies to develop educational programmes that are relevant to the local context and responsive to the local healthcare landscape. The success of our programme provides a solid foundation for future expansion, ensuring that access to neurological care becomes a global standard rather than a privilege.
Public health relevance
Headache disorders are underdiagnosed and poorly managed in Sub-Saharan Africa's primary care systems.
Training non-physician clinicians enables broader, faster access to effective headache care in low-resource settings.
Collaborations between international societies and local health programmes offer sustainable, context-adapted solutions.
Former trainees now serve as trainers, strengthening local health systems from within.
Supplemental Material
sj-pdf-1-rep-10.1177_25158163251396915 - Supplemental material for The Regional Outreach Programme of the International Headache Society: A WHO IGAP-oriented initiative in partnership with DREAM to improve healthcare for people with headache in Sub-Saharan Africa
Supplemental material, sj-pdf-1-rep-10.1177_25158163251396915 for The Regional Outreach Programme of the International Headache Society: A WHO IGAP-oriented initiative in partnership with DREAM to improve healthcare for people with headache in Sub-Saharan Africa by Daniele Martinelli, Massimo Leone, Freda Dodd-Glover and Cristina Tassorelli in Cephalalgia Reports
Supplemental Material
sj-pdf-1-rep-10.1177_25158163251396915 - Supplemental material for The Regional Outreach Programme of the International Headache Society: A WHO IGAP-oriented initiative in partnership with DREAM to improve healthcare for people with headache in Sub-Saharan Africa
Supplemental material, sj-pdf-1-rep-10.1177_25158163251396915 for The Regional Outreach Programme of the International Headache Society: A WHO IGAP-oriented initiative in partnership with DREAM to improve healthcare for people with headache in Sub-Saharan Africa by Daniele Martinelli, Massimo Leone, Freda Dodd-Glover and Cristina Tassorelli in Cephalalgia Reports
Footnotes
Author note
Acknowledgements
The authors gratefully acknowledge Prof. Majit Matharu (UK) and Prof. Derya Uluduz (Turkey) for their contribution as IHS lecturers during the first edition of the course. We also thank the Community of Sant’Egidio, represented by Dr Giovanni Guidotti, and the local DREAM team in Malawi, with special appreciation to Mathambo Lowole and Dr Victor Tamba Tolno for their invaluable support in organising and delivering the training activities.
Ethical considerations
All participants in the course were provided with an informed consent form and signed prior to participation.
Consent to participate
The participants were provided informed written consent.
Consent for publishing
All authors consent to publishing this submission with Cephalalgia Reports.
Author contributions
Daniele Martinelli: conceptualisation, methodology, literature search, coordination, and writing of the original draft. Massimo Leone: conceptualisation, methodology, data collection and analysis, writing of the original draft, and critical revision. Freeda Dodd-Glover: writing of the original draft and critical revision. Cristina Tassorelli: conceptualisation, methodology, coordination, and preparation of the final draft.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was fully funded by the International Headache Society (IHS), which supported all training activities and related logistical costs.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Data supporting the findings of this study are available from the corresponding author upon reasonable request.
Open practices
Not applicable.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.