
Abstract
Background
Migraine is the most common primary headache disorder in children and adolescents. Abnormal neuronal hyperexcitability is thought to play a role in the pathophysiology of migraine. This study aimed to evaluate the clinical features and EEG (electroencephalogram) findings in pediatric patients with migraine.
Methods
Between January 2016 and December 2023, the electronic medical records of 3740 patients who presented with headache complaints at the Pediatric Neurology Clinic were reviewed retrospectively. The ICD-10 code (R51) for headache was used to identify the patients. From this group, 172 patients were diagnosed with migraine. A total of 148 patients, aged 6–18, diagnosed with migraine according to the ICDH-3 beta criteria, with complete clinical and EEG records, and followed for at least 6 months, were included in the study.
Results
Out of the 148 patients, 81 (54.7%) were girls, and the female-to-male ratio was 1.21. The mean age of the patients was 11.6 ± 3.04 years. Twenty (13.5%) patients had migraine attacks with aura. Twenty-seven patients (18.2%) had abnormal EEGs, with 9 showing focal and 18 showing generalized abnormalities. Sixty-six patients (44.6%) have a family history of migraine and/or epilepsy. A statistically significant relationship was found between family history and EEG abnormalities (p = 0.000). Migraine with aura (20/148) showed more EEG abnormalities and a higher incidence of positive family history compared to migraine without aura (p < 0.001). EEG abnormalities were significantly higher in recordings taken during a headache attack (p = 0.000). The rate of starting migraine preventive treatment was higher in patients with abnormal EEGs (21/27).
Conclusion
Pediatric migraine diagnosis is based on clinical evaluation. In patients with a family history of migraine/epilepsy and those with migraine with aura, especially EEG recording is performed during a headache attack may play a role in the differential diagnosis and in guiding its management EEG, especially in pediatric migraine patients, considering the challenges of expression at a young age, may be used more frequently in follow-up.
This is a visual representation of the abstract.
Introduction
Migraine is the most frequent primary headache disorder in children and adolescents. Approximately 1 in 10 children suffer from recurring migraines, which can have a profound impact on their academic performance and overall quality of life.1,2 The overall prevalence varies from 3% in children aged 3 to 7 years to 23% in adolescents. 3
Migraine is a complex neurological disorder characterized by recurring episodes of severe, one-sided headaches that typically last between 4–72 h. These episodes are often accompanied by nausea, vomiting, and increased sensitivity to sensory stimuli, as well as a range of additional symptoms affecting the senses and cognitive function. 4 The International Classification of Headache Disorders, 3rd edition (ICHD-3) diagnostic criteria note that certain features of migraine in children may differ from typical features in adults. In children and adolescents, attacks may last 2–72 h.4–6
Despite extensive research on the topic, many aspects of the pathophysiology of migraine headaches are still not fully understood. 7 The mechanism underlying migraines seems to involve a primary dysfunction of neuronal activity, leading to heightened sensitivity to a variety of stimuli. Genetic factors can predispose individuals to an acute migraine attack, which is influenced by the balance between excitatory and inhibitory processes in the nervous system. 8
Moreover, electrophysiological methods are valuable for investigating the underlying mechanisms of migraines. 9 Although routine electroencephalogram (EEG) is not particularly necessary for the clinical evaluation of migraine, it can be useful in understanding the nature of migraine and its relationship with comorbid neurological diseases. 10 On rare occasions, migraine and tension-type headaches may completely overlap with epileptic activity, leading to a clinical condition known as ‘ictal epileptic headache.11,12
Although epileptiform discharges detected by EEG are primarily indicative of epilepsy, they are not exclusive to this condition. Similar abnormalities may be identified in other neurological disorders and, on occasion, in individuals without any clinical manifestations of seizures. In pediatric patients with a confirmed epilepsy diagnosis, the likelihood of detecting epileptiform patterns on EEG ranges from 60% to 90%
EEG abnormalities, including slow waves, sharp waves, spikes, and an increased photoparoxysmal response, have been observed in children with headaches.15–19 Piccinelli et al. found that 12.8% of children with headaches had EEG abnormalities. The prevalence of EEG abnormalities among children with headaches was 43.5% for migraines with aura and 5.4% for migraines without aura. 17 The prospective study by Özkan et al. suggests that electroencephalogram abnormalities are especially common in migraine patients, particularly during headache attacks. 19 In children, EEG may play an important role in the differential diagnosis of migraine and in guiding its management.
Due to the relatively limited number of EEG studies conducted in children diagnosed with migraine, this study aims to evaluate the clinical features and EEG findings in pediatric migraine patients, and, if possible, to determine the clinical significance of these abnormalities.
Materials and methods
Study population
Between January 2016 and December 2023, the electronic records of 3740 patients who presented with headache complaints at the Zeynep Kamil Training and Research Hospital Pediatric Neurology Clinic were retrospectively reviewed using the ICD-10 code (R51) for headache. There were 172 patients diagnosed with migraine. Due to limitations such as age-related communication difficulties, time constraints from limited outpatient visit durations in our country, and other challenges in routine clinical practice, EEG has been used to support clinical assessment and assist in the differential diagnosis. In our clinic, routine EEG monitoring is preferred for children diagnosed with migraine during follow-up evaluations. A total of 148 patients aged 6–18, diagnosed with migraine according to the ICHD-3 beta diagnostic criteria, with complete clinical and EEG records, and followed for at least 6 months, were included in the study, and their data were analyzed retrospectively. Exclusion criteria were: 1) a history of disorders that could lead to EEG abnormalities, such as epilepsy, encephalitis, or cognitive impairment, 2) ongoing medication use for any chronic illness, 3) the presence of pathological findings in neurological examination, 4) current use of prophylactic medications for headache. Twenty-four out of the 172 patients were excluded from the study for these reasons.
We reviewed the medical record databases of our center to gather information on the demographic characteristics of children (age, gender), clinical features of migraine, aura types, and both personal and family medical histories. Family history in first- and second-degree relatives was considered positive.
Finally, ocular refractive errors and other accompanying problems (asthma, obesity, depression, anxiety disorder, attention deficit and hyperactivity disorder) were analyzed. The patient's history of febrile seizures and the presence of benign paroxysmal vertigo of childhood were asked.
EEGs were performed in all patients diagnosed with migraine during follow-up. The patients’ headache diaries and awake-sleep EEGs were examined. Patients complaining of headache during EEG recording were also recorded. Routine EEG examinations were performed using the 18 channels digital Nihon Kohden and the International 10–20 system of electrode placement, including a full wake and sleep cycle for all patients. EEGs have been recorded both during migraine attacks and during headache-free periods and records corresponding to the headache episode were also noted. Three minutes of hyperventilation and photic stimulation with frequencies ranging from 1 to 30 Hz were conducted. EEG recordings were considered abnormal if they showed excessive diffuse or focal slowing, or epileptic activity, either focal or generalized.
All children and adolescents with migraine received patient education and counseling on lifestyle measures to help prevent attacks. These measures included maintaining good sleep hygiene, engaging in regular exercise, following a routine meal schedule, ensuring adequate fluid intake, and managing migraine triggers. The decision to start migraine preventive treatment was made through mutual discussions with the patient and their family, based on the patient's headache diary and frequency of school absences. The choice of medication was determined according to the presence of comorbid conditions (such as obesity, asthma, anxiety disorders, depression, etc.) and EEG findings.
Valproate was preferred for prophylaxis only in patients where epileptiform abnormalities (generalized/focal) were detected on EEG. In patients with normal EEG or those showing focal/generalized slow waves, the choice of medication was made based on the patient's comorbid conditions, rather than EEG findings.20,21 Beta-blockers were avoided in patients with asthma and orthostatic hypotension, while topiramate was preferred in those with obesity, and fluoxetine was chosen for patients with anxiety disorders.
Ethical approval
This study was approved by the decision of the Health Sciences University Zeynep Kamil Gynecology and Children's Diseases Training and Research Hospital Ethics Committee dated 20/01/2021 and numbered 14. With the additional decision of the ethics committee, the date range for patient recruitment was extended until December 2023. The informed consent for EEG recording and the use of the data for scientific purposes has been obtained from the patients.
Statistical analyses
Statistical analyses were performed by using SPSS version 23 (IBM SPSS Statistics, Chicago, IL). Data were expressed as numbers, percentages, and mean ± standard deviation, as needed. Categorical variables were analyzed using χ² test. A p-value <0.05 was considered statistically significant.
Results
In our study, a total of 148 patients, 81 (54.7%) were girls, and the female-to-male ratio was 1.2. The mean age of patients was 11.6 ± 3.04 years (range: 6–17 years). Fifty-seven patients (38.5%) were in the 5–10 age range (female/male:0.9), while 91 patients (61.5%) were in the 11–18 age range (female/male: 1.46).
Pain localization was frontal (49.3%), temporal (27.7%), orbital (10.8%), diffuse (6.8%), referred to vertex (3.4%) and occipital (2%). In 96 (64.9%) patients, the headache was bilateral, while only 7 out of the 52 cases with unilateral headache were in the 5–10 age range. The attack duration was between 2 and 4 h in 13 patients (8.8%), between 4 and 24 h in 104 patients (70.3%), and longer than 24 h in 31 patients (20.9%). Among the 13 patients with an attack duration of 2–4 h, 7 (53.8%) were in the 5–10 age range. Attack frequencies were categorized into five groups: monthly (33.1%), multi-weekly (29.7%), weekly (19.6%), and multi-monthly (9.5%), and sporadic (8.1%).
Throbbing headache was the predominant type of pain in both genders. Photophobia was detected in 108 (73%) patients, with a female-to-male ratio of 1.35. Phonophobia was reported in 101(68.2%) patients, with a female-to-male ratio of 1.3. Nausea was observed in 116 patients (78.4%), and vomiting was observed in 105 patients (70.9%). Nausea (female/male:1.1) and vomiting (female/male:1.02) were found to be present at similar rates in both genders. A rarer symptom, osmophobia, was reported in 22 of all patients (14.9%), of which 16 were female.
Out of 148 patients, 20 (13.5%) had migraine attacks with aura. Among all the patients of migraine with aura, 11 (55%) were girls. Visual symptoms were the most commonly reported during attacks with aura (70%) and included both positive phenomena (such as bright spots, flashes of light, or scintillating scotoma) and negative phenomena (such as vision loss). Somatosensory (15%), aphasic (10%), and motor (5%) auras were less frequently observed in our patients.
Additionally, a history of comorbid conditions was recorded in 24 patients (16.2%), including anxiety disorder in 8 patients, febrile seizures in 6, asthma in 2, obesity in 4, attention deficit hyperactivity disorder in 1, depression in 1, and precocious puberty in 1.
Awake-sleep EEG examination results were normal in 121 patients. Abnormal EEG findings were observed in 27 patients (18.2%), including generalized slowing in 13 patients, focal slowing in 8, generalized epileptiform anomalies in 5, and focal epileptiform anomalies in 1. EEG findings of patients with migraine are summarized in Table 1.
Summary of EEG findings in patients with migraine.

Abbreviations: EEG = Electroencephalogram, F = Female, M = Male, MA: Migraine with aura, MO: Migraine without aura.
No statistically significant differences were found between patient groups with normal and abnormal EEGs regarding gender, pain characteristics, pain localization, attack duration, and attack frequency (p > 0.05).
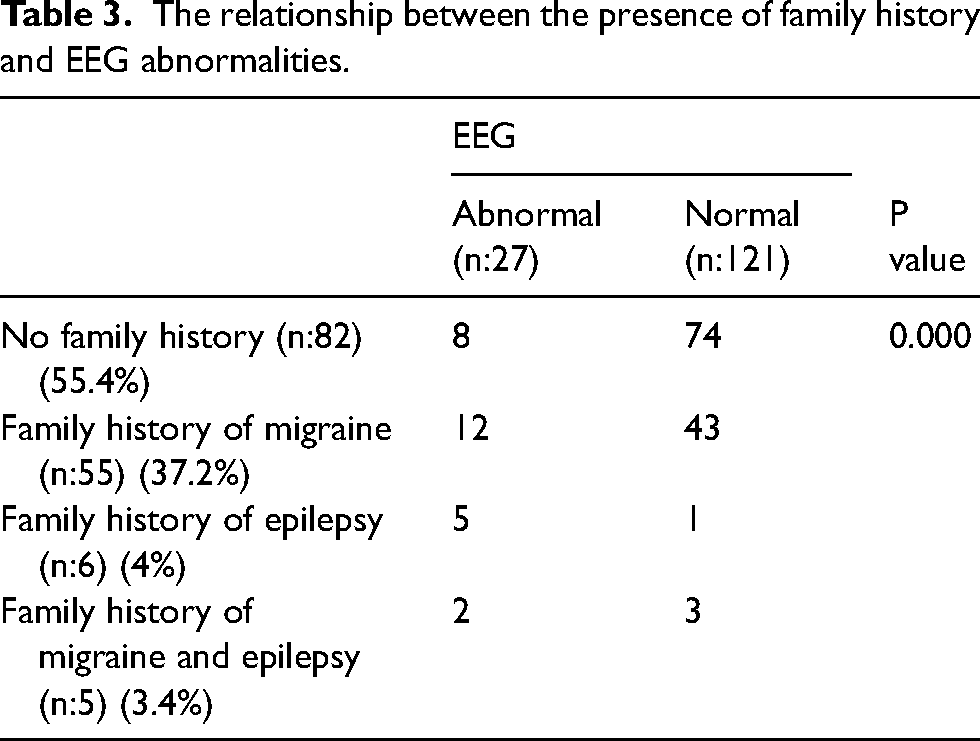
Photoparoxysmal responses were detected in the EEG examination of 7 patients (4.7%). EEG recordings of 19 patients were conducted during a headache-attack. It was determined that 11 of 27 patients with abnormal findings on EEG were taken during the headache-attack. The rate of abnormal findings in EEG examinations was significantly higher during headache attacks compared to headache-free periods, and a statistically significant relationship was found between family history and EEG abnormalities (Pearson Chi-square value = 22.978, p = 0.000; Pearson Chi-square value = 23.062, p = 0.000, respectively) (Table 2) (Table 3).
Summary of EEG findings in patients with migraine based on the presence of a headache during recording.

The relationship between the presence of family history and EEG abnormalities.
Moreover, of the 20 patients diagnosed with migraine with aura, 19 (95%) had a family history of migraine/epilepsy, whereas 47 (36.7%) of the migraine without aura patients had a family history of migraine/epilepsy. Abnormalities were detected in the EEG of 15 (75%) of patients diagnosed with migraine with aura. The presence of family history and EEG abnormalities was significant in patients diagnosed with migraine with aura than in those with migraine without aura (Pearson Chi-square value = 26.325, p < 0.001; Pearson Chi-square value = 44.922, p < 0.001, respectively).
Besides lifestyle measures, migraine preventive pharmacological treatment was administered to 27 patients. Of these, 11 patients were treated with flunarizine, 6 with valproate, 5 with propranolol, 3 with topiramate, and 2 with fluoxetine (Table 4). Preventive treatment was not started in 6 patients with EEG abnormalities due to the low frequency and severity of attacks, and EEG follow-up was continued. The rate of starting migraine preventive treatment was higher in the group with abnormal EEGs (21/27) than normal EEGs.
EEG findings of migraine patients receiving preventive treatment

Abbreviations: EEG = Electroencephalogram, MA: Migraine with aura, MO: Migraine without aura.
Discussion
Migraine is the most prevalent and disabling primary headache disorder affecting children and adolescents.1,22 Migraine can occur at any age and may even start in infancy. 22 Before puberty, migraines affect both females and males equally; however, during puberty, migraines begin to affect females more than males. 23 In our series, 57 patients (38.5%) were between the ages of 5–10 with a male predominance, while 91 patients (61.5%) were between the ages of 11–18 with a female predominance, which is in line with existing literature.
The prevalence of migraine with aura is reported to vary widely, ranging from 1.6% to 26.2%, and our rate is 13.5% with 20 patients.24,25 In our study, adolescents were 4 times more likely to experience aura compared to prepubertal children, and the average age of children reporting aura was 11.35 years. Similar findings were reported by Eidlitz-Markus and Genizi et al., who found that migraine with aura occurs more frequently in children over the age of 8.25,26 Visual aura is the most common type, occurring in 70% of patients, followed by somatosensory aura (15%), aphasic aura (10%), and motor aura (5%), which aligns with existing literature.22,27
Migraine is thought to have a polygenetic and multifactorial etiology.28,29 In our series, 66 (44.6%) of the cases had a family history of migraine and/or epilepsy, which supports the familial transmission of migraine, consistent with the literature.28,29 Just a small number of studies have examined the relationship between migraine with or without aura in children and family history.25,30 In our study, we found a significantly higher presence of a family history of migraine and/or epilepsy in patients diagnosed with migraine with aura compared to those diagnosed with migraine without aura (p < 0.001).
In a large study conducted by Tal Eidlitz-Markus et al. in a tertiary care pediatric headache clinic, it was found that female children and adolescents with treated migraine had a higher incidence of migraine with aura and a lower frequency of vomiting compared to males. The authors suggested that these findings might be attributed to the better verbal communication skills of females, which could enable them to describe migraine symptoms more effectively. 31
We found that photophobia (F/M ratio: 1.35) and phonophobia (F/M ratio:1.3) were more common in females, while nausea and vomiting were observed at similar rates in both genders. Osmophobia, a less common symptom, is not included in the diagnostic criteria and has been investigated in only a limited number of studies. In a large series, osmophobia is reported in 34.6% of pediatric patients with migraine. 32 We observed osmophobia in 22 of all patients (14.9%), with 16 of them being female.
The ICHD-3 diagnostic criteria note that certain features of migraine in children may differ from typical features in adults. While migraines in adults typically last 4 to 72 h, the duration of attacks in pediatric patients can be as brief as 2 h.4–6 Short headache attack duration is a prominent feature of pediatric headaches, which may be linked to specific pathophysiological mechanisms in children. Additionally, the literature agrees that determining the exact end time of an attack in children can be challenging, and therefore accurately assessing the duration of the attack can be difficult.33,34
In our study, 13 patients (8.8%) had attack durations between 2 and 4 h, and of these, 7 (53.8%) were aged 5–10 years. Some studies suggest that reducing the attack duration criterion to less than 2 h can improve diagnostic sensitivity, particularly in children under 6 years old. 34 However, since our study did not include patients under 6, we could not evaluate this aspect.
The ICHD-3 categorizes a group of disorders that have been traditionally recognized as occurring in childhood and may be associated with a higher risk of developing migraine. Taking a detailed history of these episodic syndromes may be valuable in supporting the diagnosis of migraine. 4 Pediatric migraine variants, previously referred to as childhood periodic syndromes, primarily include benign paroxysmal vertigo in children, benign paroxysmal torticollis, cyclic vomiting syndrome, and abdominal migraine.4,22 We noted that five of our patients had a medical history of benign paroxysmal vertigo.
Migraine is diagnosed based on a detailed clinical history and neurological examination. There is no definitive diagnostic test available. The diagnosis may be more difficult in young children who have a limited ability to describe their symptoms or in patients with atypical symptoms.4,10 Epilepsy and migraines are often seen as comorbid conditions, with the presence of one increasing the likelihood of the other.18,35 The comorbidity of migraine and epilepsy is an area of active research, as both conditions are common chronic neurological disorders in children. They share similar pathophysiological and genetic mechanisms associated with paroxysmal disorders, including overlapping precipitating factors, clinical symptoms, and treatment strategies.35,36
The relationship or co-occurrence between epilepsy and headaches, whether causal or coincidental, has been under discussion for over a hundred years. At its core, the presence of both headaches and epileptic seizures is thought to reflect an underlying alteration in neuronal network excitability. More recently, headache has been increasingly recognized as a manifestation of a transient brain state of altered excitability—particularly within the framework of the “dysexcitability” concept—occurring at different times in the same individual.37,38
An EEG is a non-invasive test that can be valuable in studying the pathophysiology of migraine and is commonly used as a tool for patients with headaches in the differential diagnosis of epilepsy. However, according to the European Federation of Neurological Societies guidelines for diagnosing non-acute headaches, an interictal EEG is not routinely recommended for headache diagnosis. 39 Abnormal EEG findings were observed in several studies of headache patients, particularly in those with migraines.17,18,40 Studies investigating EEG findings in children with migraine have reported that the prevalence of EEG abnormalities ranges widely from 5.5–35.2%.17,18,40,41 We believe that the wide range of results found in retrospective studies in the literature may be influenced by the heterogeneity of the patient groups and the timing of EEG recordings, which may coincide with either headache or headache-free periods.
In our study, abnormal EEG findings were noted in 27 migraine patients (18.2%). Furthermore, among the 20 patients diagnosed with migraine with aura, 15 (75%) showed EEG abnormalities. Additionally, the rate of EEG abnormalities was found to be statistically significantly higher in patients with migraine with aura compared to those with migraine without aura (p < 0.001). In light of our findings and the literature, we believe that it would be appropriate to perform EEG earlier, especially in pediatric patients with migraine with aura.18,42
Generally, an EEG may be performed in headache patients, especially for atypical auras (visual and brainstem auras) or episodic loss of consciousness for the differential diagnosis of epilepsy. 42 EEGs were performed on all patients diagnosed with migraine during follow-up in our study. The predisposition for its occurrence is likely influenced by genetic factors that cause the cerebral cortex to shift between states of hyperexcitability and hypoexcitability at different points in time within the same individual, due to an imbalance in excitatory and inhibitory mechanisms. 37 In 66 of our patients (46.6%), there was a family history of epilepsy and/or migraine. In this group, we observed a significantly higher rate of EEG abnormalities compared to those without a family history. This finding suggests that genetic factors contributing to altered cortical excitability may play a role in the development of both epilepsy and migraine. 37 Especially in patients who are unable to express themselves or in younger age groups, in those with a family history of migraine and/or epilepsy, we suggest that EEG may play a role in the differential diagnosis of migraine and in guiding its management.
In the prospective study by Özkan et al., they examined EEG findings in patients with migraine and tension-type headache, observing a significantly higher rate of EEG abnormalities during migraine attacks (36%) compared to the headache-free period (9%). 19
Although our study is retrospective, since the presence of a headache was documented during EEG recordings, we were able to compare the recordings taken during headache attacks with those taken during headache-free periods. It was found that 11 out of 27 patients with abnormal EEG findings had recordings taken during a headache attack. Similar to the findings of Özkan et al., the frequency of abnormal findings in EEG examinations was significantly higher in recordings made during a headache attack compared to those made during headache-free periods (p = 0.000). 19
Migraine and epilepsy, being paroxysmal in nature, are considered episodic disorders and share several common clinical features. Migraine headaches and epileptic seizures can be easily confused with one another and may even occur together. Specifically, seizures originating in the occipital lobe may be mistakenly identified as migraine auras. 36 As observed by Parisi et al. and Verrotti et al., headache can serve as the sole manifestation of epilepsy, a rare event where a seizure occurs during the aura phase of a migraine.43,44
In migraine, neocortical hyperexcitability is thought to evolve into cortical spreading depression (CSD), rather than the hypersynchronous activity typically seen in epilepsy. 45 CSD is increasingly recognized as the underlying mechanism for migraine aura and the initiation of headache pain. Several researchers have identified CSD as a key link between migraine and epilepsy.36,45 The hypothesis of increased cortical excitability shared by both conditions is further supported by the effectiveness of certain antiepileptic drugs, such as topiramate, valproic acid, and gabapentin, which have demonstrated benefits in preventing migraines.22,36
Piccinelli found that 87% of pediatric migraineurs had normal EEG findings in the absence of headache or within 24 h of a headache. 17 Especially during or shortly after a migraine attack, the EEG may appear normal or show transient changes such as focal (typically temporal) or generalized slow-frequency activity and asymmetry in the background activity.16,19,36
In migraineurs without aura, the EEG may show an asymmetry or slowing of the background activity located contralateral to the headache. During a classic visual aura, the EEG may either be normal or show posterior delta waves or a reduced amplitude of the normal alpha rhythm.15,16,46 Martens et al. conducted a study involving 209 patients, in which they found that 82.8% of the EEGs were normal, and that the most common abnormality was diffuse or focal slowing (%5.3), while epileptic waves were observed in a lesser proportion (%3.3). 47 In our series, among the 27 patients (18.2%) with abnormal EEG findings, we observed generalized slowing in 48.1% (13/27) and focal slowing in 29.6% (8/27) of the patients. Our results, where the most commonly observed abnormality was slow wave abnormality, show similarity to previous studies.15,19,41 The EEG abnormalities identified in our study were also nonspecific, similar to those reported in previous studies, and their clinical significance remains uncertain.12,15,17,19,40,47 While generalized epileptiform abnormalities were detected in 5 of our patients and focal epileptiform abnormalities in 1 patient, none of the patients were diagnosed with epilepsy during the follow-up period. Additionally, in 23 patients with EEG abnormalities, we observed that the EEG normalized during follow-up, with some patients on migraine preventive treatment and others spontaneously.
The objective of migraine preventive treatment is to reduce the frequency of migraine attacks.1,22 Furthermore
Anxiety and mood disorders are commonly reported as comorbidities in children with migraine, and addressing these is crucial due to their potential effects on both the headache and overall quality of life. 48 Eight of our patients had been diagnosed with anxiety disorder, and one had been diagnosed with depression. Besides counseling in a clinical setting that emphasizes routine and consistency, structured behavioral approaches such as cognitive behavioral therapy and biofeedback have proven to be helpful for preventing migraines. 22 One patient diagnosed with depression and four patients diagnosed with anxiety disorder were referred for cognitive behavioral therapy support.
We are aware of the limitations of this study mainly being its retrospective character and lack of healthy control group. The rate of initiating migraine preventive treatment was higher in patients with abnormal EEGs (21/27). However, due to the small number of patients with abnormal EEGs who did not receive preventive treatment, a statistical comparison between the treated and untreated groups was not possible. The relatively small number of patients diagnosed with migraine with aura limits the ability to make comprehensive comparisons.
Our study had several strengths, despite some limitations. In our study, since EEG was performed on all migraine-diagnosed patients during follow-up, even though we did not have a control group and the study had a retrospective design, we were able to compare the clinical and EEG features of all migraine patients. We demonstrated a strong correlation between the presence of a family history of epilepsy/migraine and EEG abnormalities. Additionally, we obtained results supporting the literature, showing a higher rate of EEG abnormalities detected during headache attack, and that in migraine with aura, both family history and EEG abnormalities were more prevalent compared to migraine without aura. EEGs were recorded both during migraine attacks and headache-free periods, but since the study only notes whether the patient had a headache during the EEG, naturally, we cannot definitively associate the data with a migraine attack.
Although the findings of this study offer valuable information regarding the clinical and EEG features of pediatric migraine patients, caution is needed when applying these results to the broader pediatric migraine population. To strengthen the generalizability, future research could replicate these findings in different clinical settings with larger and more diverse populations.
Conclusion
The results of this study suggest that pediatric patients with migraine with aura may require EEGs, as there could be shared pathophysiological mechanisms between migraine and epilepsy. In patients with a family history of migraine/epilepsy and those with migraine with aura, especially EEG recording performed during a headache attack may play a role in the differential diagnosis of migraine and in guiding its management. Patients with abnormal EEGs required more migraine preventive treatment in follow-up.
We are aware that nonspecific abnormal EEG findings are present in children with migraine, and we believe that EEG, especially in pediatric migraine patients, can help clarify the borderland between migraine and epilepsy, considering the challenges of expression at a young age, and that EEGs may be used more frequently in follow-up. However, large prospective controlled studies are needed to determine the clinical significance of EEG findings.
Article highlights
The presence of a family history of epilepsy/migraine is associated with EEG abnormalities in pediatric migraine patients.
Migraineurs with aura had more EEG abnormalities and a higher positive family history compared to those without aura.
EEG abnormalities were more common during headache attacks.
EEG may be used more frequently in follow-up for pediatric migraineurs, given the challenges of expression at a young age.
Footnotes
Acknowledgments
Special thanks to Prof. Dr Rabia Gönül Sezer Yamanel for her insightful feedback and guidance throughout this research.
Author contributions
Conceptualization: E.U., N.E.H.; methodology: E.U; software: E.U.; validation: E.U., N.E.H.; formal analysis: E.U., R.G.S.Y.; investigation: E.U; resources: E.U., N.E.H.; data curation: E.U., N.E.H; writing—original draft preparation: E.U; writing—review and editing: E.U, N.E.H.; supervision: R.G.S.Y. All authors have read and agreed to the published version of the manuscript.
Data availability statement
The datasets generated and/or analyzed during this study can be obtained from the corresponding author upon reasonable request.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed consent statement
All parents or legal guardians consented to their children's participation in the study.
Institutional review board statement
This study was approved by the decision of the Health Sciences University Zeynep Kamil Gynecology and Children's Diseases Training and Research Hospital Ethics Committee dated 20/01/2021 and numbered 14. With the additional decision of the ethics committee, the date range for patient recruitment was extended until December 2023.