
Abstract
Background:
Changes in atmospheric pressure are suggested to trigger headaches. This pilot study was made to determine craniofacial sensations accompanying short phases of changing barometric pressure.
Methods:
In a crossover design, 15 adult healthy subjects were exposed in a climate chamber to 8 min phases of barometric pressure lowering by 0, 20 and 40 hPa. The subjects rated their sensations of ear pressure, head compression and the occurrence of headache every minute on a visual analogue scale (VAS, range 0–10). Pulse rate was recorded as a parameter for autonomic functions.
Results:
Nearly all subjects experienced ear pressure and half of them compression of their head at variable degrees. These sensations started in most subjects during the phase of lowering barometric pressure and increased to an average rating of about 3 VAS when returning to ambient atmospheric pressure. Heart rate slightly decreased during this phase. Three subjects reported mild to moderate headache for various durations within these phases.
Conclusions:
Changes in barometric pressure can be associated with sensations of ear pressure and head compression and may trigger headaches. The generation of these sensations is discussed with regard to convergent trigeminal innervation of the ear, the paranasal sinuses and the cranial meninges.
Introduction
Barometric pressure changes affecting humans in their environment can either be caused by weather changes with developing low or high atmospheric pressure systems or when people move to different heights above sea level and back like during mountain climbing or air travels. These situations can be associated with the occurrence of headaches but clinical data and the underlying mechanism are unclear, partly because all these conditions include more factors than only barometric pressure changes. Regarding weather changes, a considerable proportion of headache sufferers believe that they are sensitive to rain, wind and changes in atmospheric pressure 1 but systematic examinations are rare and inconsistent; in addition, the headaches were not properly classified. 2 In their current review, Maini and Schuster 2 summarized the available literature and reported that changes in barometric pressure can trigger primary headaches such as migraine and tension-type headache; however, more substantiated is a causative role for barometric pressure changes in the generation of some defined secondary headache disorders like high-altitude headache and headache attributed to airplane travel, listed in chapters 10.1.1 and 10.1.2, respectively, of the International Classification of Headache Disorders (ICHD-3). 3
Concerning primary headaches, some studies performed on groups of migraineurs revealed that changes in atmospheric pressure was only one of several factors that seemed to be associated with the prevalence of migraine. 4 –7 Bolay and Rapoport reviewed the data and concluded that low atmospheric pressure does not trigger migraine attacks unless it is accompanied by other factors. 8 Concerning non-classified headaches, a case crossover analysis of more than 7000 headache patients found an association of non-migraine headaches and low barometric pressure 2–3 days before the patients were seen in the emergency department. 9 Daily sales of loxoprofen, the preferred over-the-counter drug used against headaches in Japan, have been reported to increase when the average barometric pressure decreased. 10
In high-altitude headache, which is usually accompanied by additional symptoms of mountain sickness, 11 low atmospheric pressure is usually accompanied by hypoxia and cold. The essential impact of low oxygen levels on headache and migraine generation was recently examined by means of a hypoxic chamber. 12
Different to this simulation, the present pilot study focused on cranial sensations associated with small changes in barometric pressure (20 and 40 hPa) that can accompany weather changes. It was initiated following the experience of one of the authors in a previous investigation, in which we studied the activity of neurons in the rat spinal trigeminal nucleus with afferent input from the cranial dura mater. 13 In these previous experiments the same stimulus parameters as in the present study have been used, while the examiner stayed in the chamber and experienced ear pressure and mild to moderate headaches in temporal and frontal areas during changes of atmospheric pressure in each session. Therefore, the rationale of the present study was to evaluate these subjective experiences under controlled conditions in a small group of adults not suffering from migraine or any other form of primary headaches. We hypothesized that during changes in barometric pressure subjects may experience some form of pressure sensation at their head, possibly even headache. The experimental conditions were designed to simulate changes in atmospheric pressure during weather perturbations or changing altitudes of some hundred metres.
Methods
Participants
The study was conducted according to the World Medical Association Declaration of Helsinki and reviewed and approved by the Institutional Review Board of the Nagoya University (approval number 276, April 2006 and 276-2, February 2007). The participants, most of them students at the Nagoya University, were recruited for the study after they had given their written informed consent. None of the participants was suffering from diagnosed primary headaches or craniofacial pain, other acute or chronic medical problems or mental diseases. None of the participants reported acute or chronic problems with eyes, ears or nose or had any treatment of these organs in the past year. The participants were informed about the rationale of the study.
Experimental room
The experiments were conducted in a climatic chamber located at the Research Institute of Environmental Medicine, Nagoya University. The chamber allows to host up to six persons under artificial climate conditions simulating weather variables (light, temperature, humidity, barometric pressure, air movements), which can be separately and nearly selectively changed within natural limits. During the experiments temperature (25°C) and humidity (50%) were kept constant and air flow (unavoidably due to in- and outflow for air pressure changes) was kept at a minimum, while the air pressure was systematically varied starting from the particular environmental atmospheric pressure of the day. The actual air pressure in the chamber was continuously recorded throughout the experiments.
Sessions
The experiments spanned 8 months (February–November) and consisted of three different sessions performed on three different days, in which the test persons participated in random order (Figure 1). The interval between the different sessions of each participant was at least 2 days. In each session two or three persons were present in the chamber sitting in a comfortable position. Electrodes were attached to the extremities according to the Einthoven system to record the electrocardiogram (ECG). The heart rate was off-line extracted from the ECG using PowerLab with LabChart version 5.4.2 software (ADInstruments Japan, Nagoya, Japan). The sessions were identical except for the atmospheric pressure changes by 0, 20 and 40 hPa. The test persons were informed about the three possible modes of the sessions but not about the particular atmospheric pressure change in each session. During the experiments white noise of moderate intensity was applied to reduce recognition of specific sounds of the pumps associated with changes in barometric pressure. None of the test persons complained about an unpleasant sensation upon the white noise.

Timeline of experiments with barometric pressure lowering by 0 hPa (dotted line), 20 hPa (dashed line) and 40 hPa (continuous line). Heart rate was recorded 30 min prior to and throughout the experiment, ear pressure, sensation of head compression and headache were reported on a visual analogue scale (VAS) every minute during the phases ‘pre’-‘post’.
Experimental performance
Each session consisted of a baseline period of about 30 min, in which the heart rate of each test person was registered until it was stable, and five phases with a total duration of 40 min, which started after closing the chamber (Figures 1 and 2(a) to 4(a)): (a) 8 min constant air pressure equalling the natural atmospheric pressure (‘pre’), (b) continuous, nearly linear lowering of pressure within 8 min (‘down’), (c) constant pressure for 8 min at the low value (‘hold’), (d) continuous, nearly linear increase in pressure within 8 min (‘up’) and (e) constant normal environmental pressure for 8 min (‘post’); afterwards the door of the chamber was opened. When the pressure remained unchanged, simulated noise mimicked the sound of the pumps during pressure changes.
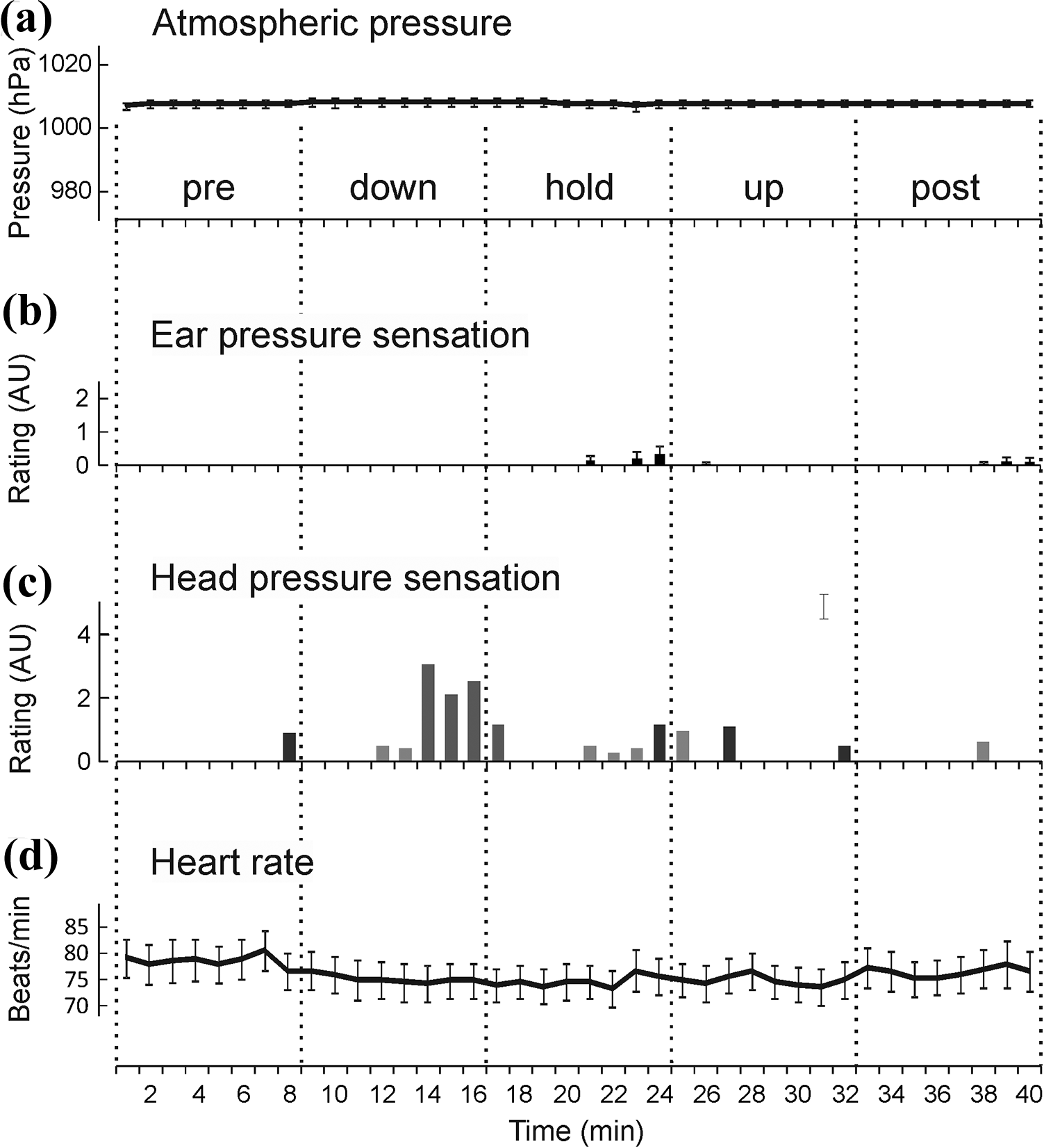
Craniofacial sensations and heart rate during the control session with no barometric pressure change (a, mean ± SEM). (b) Mean values of ear pressure sensation (±SEM). (c) Cumulative values of head compression sensations, subject values are expressed by bars of different grey values. (d) Heart rate (mean ± SEM).
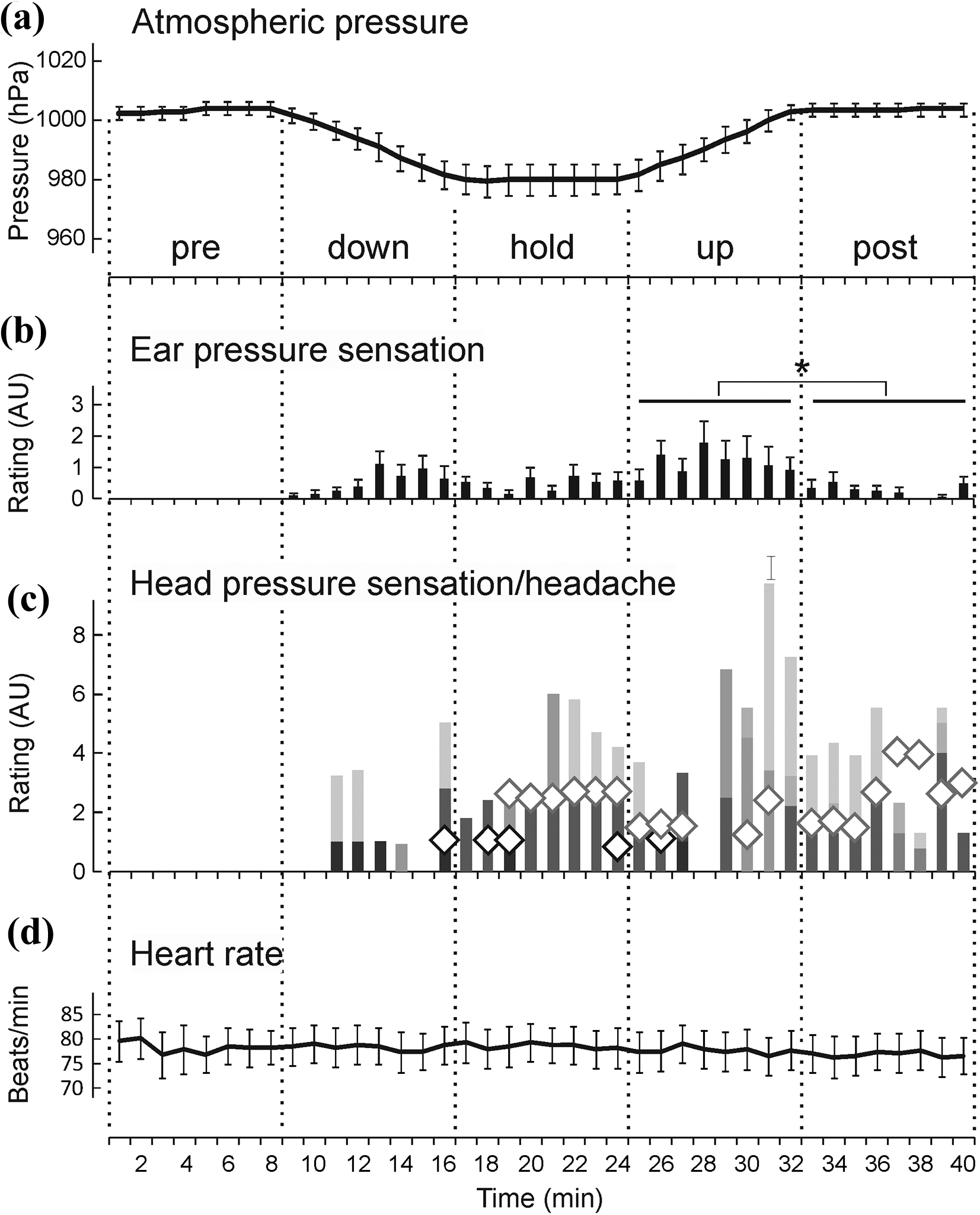
Craniofacial sensations and heart rate during transient lowering of barometric pressure by 20 hPa (a). (b) Mean values of ear pressure sensation (±SEM); *significant difference between ratings of ‘up’ and ‘post’. (c) Cumulative values of head compression sensations, subject values are expressed by bars of different grey values; headache is added as open squares. (d) Heart rate (mean ± SEM).

Craniofacial sensations and heart rate during transient lowering of barometric pressure by 40 hPa (a). (b) Mean values of ear pressure sensation (±SEM); *significant difference between ratings of ‘up’ and all other test phases. (c) Cumulative values of head compression sensations, subject values are expressed by bars of different grey values; headache is added as open square. (d) Heart rate (mean ± SEM); *significant difference to phase “pre”.
During the experiment the test persons filled a questionnaire containing non-graded visual analogue scales (VAS) reaching from 0 (no sensation) to 10 (maximal sensation). The sensations had to be registered every minute. The items asked were (1) pressure sensation on the ears, (2) sensation of head or eye compression, (3) dizziness and (4) headache. In addition, a scheme was presented showing four sides of a head, where the test persons could draw the location of head compression and headache. The test persons were asked to make a note if they yawned or gulped or pressed on their ears to equalize the perceived air pressure.
Biometry, data analysis and statistics
The intended sample size (n = 15) was calculated expecting an effect size of f = 0.3 in the VAS ratings caused by changes in atmospheric pressure between the five phases of the experiment analysed by repeated measures analysis of variance (ANOVA) setting an α error of 0.05 and a β error of 0.2 (G*Power 3.1 software, Universities of Kiel, Mannheim, Düsseldorf, Germany). This effect size was expected based on the differences in spinal trigeminal activity and heart rate measured in previous electrophysiological recordings in animal experiments with a similar design regarding atmospheric pressure changes. 13 In the present study the 1 min VAS ratings and heart rate values of each test person were averaged within each of the five test phases (‘pre’ to ‘post’). These mean values were statistically evaluated across the whole study group using repeated measures ANOVA extended by the Tukey post-hoc significance (HSD) test (Statistica 7.0 software package; StatSoft, Tulsa, OK, USA); p values < 0.05 were regarded as significant. Values are reported as means ± standard error of the mean (SEM).
Results
Subjects
Sixteen healthy volunteers, 11 females and 5 males aged 18–58 years (mean 26.6, median 19 years) were included in the study. One female came down with a cold after her first (40 hPa) session and therefore did not continue the experiments, another female dropped out after her first (20 hPa) session. Therefore, data of either these sessions derived from 15 subjects. Eleven persons participated in the 0 hPa session. The test persons were interviewed prior to the experiments about their experiences with headaches. Three of them reported that they never had any kind of headache. Six persons, who had experienced unclassified headaches, reported two to three episodes during the last 6 months, another six persons more than five headache episodes. None of the test persons was diagnosed to suffer from any specific type of primary headache according to ICHD-3 including migraine but non-classified tension-type headache could not be ruled out. Four persons noted that their headaches may be related to weather variables, either heavy rain, strong wind, immediately before and after typhoons, high atmospheric pressure or strong sunshine. None of the participants was suffering from a significant paranasal sinus disease. None of the participants complained about headache at the beginning of each session.
Sensation of ear pressure
Eight of 11 subjects in the 20 hPa session and 9 in the 40 hPa session (among them 3 males) but only 3 persons (1 male) in the control experiment (0 hPa) reported sensations of pressure on their ears during the low-pressure experiments (Figures 2(b) to 4(b)); 3 participants did not rate ear pressure. The sensations were symmetrical, were striking both ears and occurred mainly during the phases of the experiments, in which the atmospheric pressure was changed (‘down’ and ‘up’). The sensation was particularly strong in the phase of increasing pressure, in which the average peak intensity reached 2 (20 hPa) or exceeded 3 (40 hPa) on the VAS, respectively; in three persons (two males) the intensity of ear pressure exceeded 5 on the VAS. The mean value was 1.11 ± 0.54 (20 hPa) and 2.11 ± 0.69 (40 hPa). However, there was considerable variance between the participants with two of them rating 0 during the whole experiment. The VAS values of the persons reporting head pressure between the test phases were evaluated with repeated measures ANOVA, which revealed significant variance during the 40 hPa experiment (F(4,40) = 9.28; p < 0.001). The Tukey post-hoc test showed that the values within the phase ‘up’ were significantly different to all values of all other phases (p < 0.001–0.01). In the 20 hPa experiment only the phases ‘down’ to ‘post’ could be compared with ANOVA, because ‘pre’ showed no variance due to the only rating 0. There was a significant effect (F(3,30) = 4.19; p = 0.014) and a difference between the ratings of ‘up’ and ‘post’ according to the Tukey test (p = 0.012). In most participants the ear pressure sensation tailed off within the 8 min of the last phase (normalized ambient pressure). In only one person during the 40 hPa and in four persons during the 20 hPa experiment the pressure sensation outlasted this phase. The few ratings (deviant from 0) in the 0 hPa experiment showed no significant effect.
Sensation of head or eye compression
Seven of 14 subjects (2 males) in the 20 hPa session and 8 subjects (1 male) in the 40 hPa session noted sensations of compression or localized pressure onto their head, preferentially during the constant low-pressure phase (‘hold’), the increase to environmental pressure values (‘up’) and during the phase of normalized pressure (‘post’); 1 person did not rate. Persons who noted these sensations reported also ear pressure. The time and the strength of the head compression sensation were again considerably variable between the subjects with more than 4 VAS within the ‘up’ phase in one (female) participant in the 20 hPa session, while others rated 0 during the whole experiment. Figures 2(c) to 4(c) show the cumulated individual sensation strengths as drawn on the VAS. Three persons experienced this sensation surprisingly as more severe during the 20 hPa decrease than during the 40 hPa decrease (see discussion). The head compression sensation outlasted the phase of normalized ambient pressure in the 40 hPa session in one participant and in the 20 hPa session in two participants. ANOVA with repeated measures (including only persons who reported head pressure) revealed no significant difference in any of the experiments (20 hPa: F(3,39) = 0.86; p = 0.47; 40 hPa: F(3,30) = 0.93; p = 0.44). Three subjects complained about compression sensations even when the barometric pressure was not changed (0 hPa session). Preferential areas, at which the subjects felt pressure, were the temple and the whole temporal area. One female subject noted eye compression during the ‘up-phase’ of the 20 hPa session.
Headache
Three subjects, all females, reported headaches during changing barometric pressure, two in the 20 hPa session but not in the 40 hPa session, and one in the 40 hPa session (Figures 3(c) and 4(c)). There was no association of the headache sensation with the order of low-pressure exposures making an influence of expectance or experience unlikely. However, all three subjects were among those who reported that their incidental headaches were related to weather changes. These subjects experienced headache in the phases ‘hold’, ‘up’ and ‘post’ and the headache was associated with head and ear pressure sensations in two persons and with only ear pressure in one person. In one person the headache reached nearly grade 4 on VAS during the 20 hPa session and, together with head pressure sensation, outlasted the phase of normalized ambient pressure. No subject experienced headache during the 0 hPa session.
Dizziness
None of the subjects noted dizziness in any of the sessions.
Heart rate
The mean heart rate of 14 subjects (in 1 person measurements failed) ranged from 50 to 95 beats/min. The average heart rate of the whole cohort was stable during the 0 hPa and the 20 hPa experiment but slightly decreased during the 40 hPa experiment (Figures 2(d) to 4(d)), i.e. it was significantly lower in phases ‘up’ and ‘post’ compared to phase ‘pre’ (ANOVA with repeated measurements, F(4,52) = 4.55; p = 0.003 and Tukey post-hoc test, p = 0.019 and 0.004). One of the persons who experienced headache was deviant; she had a heart rate of about 100 beats/min with an increasing tendency during the experiment.
Discussion
Sensations of ear pressure, head compression and headache
The present experiments demonstrate that transient lowering of barometric pressure by 20 and 40 hPa can be associated with craniofacial sensations such as ear pressure, head compression and occasionally mild headache in healthy subjects. It seems obvious that the sensation of ear pressure upon changing atmospheric pressure is due to a pressure inbalance between the external and the middle ear causing deformation and tension of the tympanon. This assumption is supported by the ratings, which are on average higher during the pressure changes in the 40 hPa experiment compared to the 20 hPa experiment (see Figures 3(b) and 4(b)). This was different regarding the sensation of head compression, since there was no clear difference in the frequency and severity of the head compression sensations between the 20 hPa and the 40 hPa experiment (see Figures 3(c) and 4(c)). Some participants experienced the head compression even as more severe in the 20 hPa experiment than in the 40 hPa experiment. Some test persons noted that they executed less ear pressure adjusting maneuvers such as yawning and swallowing in the 20 hPa experiment, which may be an explanation for this higher rating.
Under natural conditions like weather changes, barometric pressure changes are smaller and slower (0.1∼1 hPa/hr) and possibly not balanced by these maneuvers but it should be taken into account that even such small changes may induce long-lasting pressure imbalances in the ear that may lead to uncomfortable sensations. There may be a transition between the sensation of head compression and headache, and the interpretation of both sensations may be highly individual. Thus in a more extended study it may be useful to ask the participants to compare the rated headache sensations with their experiences of spontaneous headaches.
Generation of head pressure sensation and headache
In a previous animal experimental examination using the same stimulus paradigm as in the present study we recorded from neurons in the rat spinal trigeminal nucleus with afferent input from the cranial dura mater. 13 In humans those neurons are supposedly signalling headaches. Not all of these neurons but a distinct sample with convergent input from the cornea and the orbita increased their activity during lowering of barometric pressure (phases ‘down’ and first minutes of ‘hold’). This study suggested that a pressure sensor may be located around the eye and let us speculate that additional extracranial inputs to spinal trigeminal neurons may be important factors for triggering headaches. We did not investigate a possible convergent input from the ear at this time but the involvement of the inner ear in sensing barometric pressure changes has been suggested by another series of examinations of our group. Paw lifting to tactile stimuli in rats indicating mechanical hyperalgesia following chronic nerve constriction injury 14 was aggravated during and after lowered barometric pressure by 27 hPa for 80 min, 15 and this behaviour was abolished after inner ear lesion. 16 In a recent study in mice, as a marker for neural activation the number of c-Fos-positive cells in the superior vestibular nucleus was found to be increased following exposure to lowered barometric pressure by 40 hPa for 50 min. 17
Although a pressure sensor has not yet been described, we speculate that central neurons signalling head pressure or headache receive convergent input from intracranial afferents and mechanically sensitive nociceptors innervating middle ear structures like the tympanon. Meningeal afferents which, according to our understanding, are involved in headache generation, could even form collaterals that innervate the middle ear, as it was found in meningeal afferents innervating pericranial structures. 18,19 Other structures that come into account for sensing changes in barometric pressure are the paranasal sinuses, which can be more or less open to the ambient air. An association of sinonasal anatomy and headaches presumably triggered by Chinook winds has been described. 20 The authors concluded that anatomical variations blocking the sinus ostia may prevent equilibration of changes in atmospheric pressure, thus forming a risk factor for these headaches.
Autonomic changes
In our previous animal experimental study 13 the arterial blood pressure decreased during the low-pressure exposure, followed by an increase in heart rate during the re-establishment of normal pressure. In the present human study, the heart rate slightly decreased during the 40 hPa experiment. This may indicate that the changes in atmospheric pressure have an impact on the autonomic nervous system. It is unclear if this phenomenon is functionally related to the sensations described. Autonomic dysregulation has frequently been reported in headache patients. 21
Atmospheric pressure changes and headache
Atmospheric pressure changes of the size as executed in our experiments, though with slower changes in time, are frequent events that accompany the approach of low-pressure systems like typhoons. Within a similar time course they also occur during travels with a cable car or during ascending and descending flights, where a change in atmospheric pressure by 40 hPa corresponds to a height difference of about 320 m relative to sea level. Headache associated with airplane travelling has attracted particular attention about one decade ago 22 –25 ; later this acute headache was specified 26,27 and classified as ‘headache attributed to airplane travel’ (ICHD-3A). 3 In a survey on more than 250 passengers, Bui and colleagues found an incidence of 8.3% for the ‘airplane headache’ and an even higher incidence in persons with a history of high-altitude headache. 28 This headache, which occurs most often during landing, i.e. increase in atmospheric pressure, appears mostly unilaterally, preferentially in the fronto-orbital region, and lasts usually not longer than 30 min; Mainardi et al. 26 and Bui and Gazerani 27 suggested an involvement of affected paranasal sinuses. We may assume that the persons who are prone to ‘airplane headache’ have generally a higher susceptibility to barometric pressure changes. Similar headache phenomena have also been reported during diving and during rapid descent from high mountains; an imbalance between intrasinusal and external air pressure as a common pathological basis may also be involved. 26 In a recent study, 29 patients regularly suffering from ‘airplane headache’ and healthy controls were subjected to barometric pressure changes as occurring during airplane travels, simulated in a pressure chamber similar to the devise of our examination. All seven patients suffering from ‘airplane headache’ but none of the group of seven control persons experienced headache during this simulation. 29 However, the changes in atmospheric pressure applied in this simulation were much higher than in our study. We changed the barometric pressure within 8 min by maximally 40 hPa, whereas in the airplane simulation the change was about 250 hPa simulating a height of 2438 m that was reached within 5–6 min.
We conclude that even small changes in barometric pressure, as they can occur during weather changes, can cause cranial sensations and can be a potential trigger for headaches. Some persons seem to be particularly sensitive to this stimulus. This does not argue for changes in atmospheric pressure as a specific trigger for migraine or tension-type headache but some patients suffering from primary headaches may additionally be sensitive to changes in barometric pressure. Apart from the mentioned meteorological data 4,5 and the simulation of airplane headache, 29 experimental studies in patients examining the association of experimental or travel-induced barometric pressure changes and the initiation of headache attacks are lacking.
Limitations of the study
The a priori assumed effect size caused by the air pressure changes in our experiments was too optimistic in the light of the high variance of ratings between test persons and test phases, particularly since some participants rated 0 throughout the experiment. Therefore, it was not possible to draw reliable conclusions about the temporal association or the follow-up of different complaints, which could provide hypotheses about functional associations between the craniofacial sensations. A more extended examination with biometrical calculations based on a smaller effect size may be useful to ascertain the not statistically evaluable trends in the present study, particularly head pressure sensation and headache. Also, a true placebo group would be useful to test if repeated sessions under same conditions might have an impact on the craniofacial sensations. Additional psychophysical measurements like sensitivity testing to mechanical and thermal stimuli may be included in such a future study.
Conclusions
Taken together, our experiments have shown that changes in ambient barometric pressure by values, which are quite common during travels with changing positions above sea level, but also changes in atmospheric pressure associated with weather changes can induce unpleasant craniofacial sensations such as ear pressure, head compression and even headache. The underlying mechanisms are unclear but may be related to an impact of barometric pressure changes on the middle ear and the paranasal sinuses. Future research should look at a possible collateral or convergent afferent innervation of these structures and the meninges as the main site of headache generation. Furthermore, a broader study including more subjects and with repeated exposure to same barometric pressure changes may confirm an association between these unpleasant sensations and headache.
Key findings
Small transient lowering of barometric pressure can cause craniofacial sensations such as ear pressure, head compression and mild headaches in healthy subjects.
These symptoms are highly variable among persons.
The experiments may model in part environmental changes in atmospheric pressure as trigger factors for unpleasant craniofacial sensations and headache.
Footnotes
Acknowledgements
The authors acknowledge the generous permission to use the climate chamber of the Institute of Environmental Medicine of the Nagoya University.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethic approval and patient consent
The study was conducted according to the World Medical Association Declaration of Helsinki and approved by the Institutional Review Board of the Nagoya University responsible for ethical issues (approval number 276, April 2006 and 276-2, February 2007). All participants were informed about the experimental procedures and gave their written consent to participate in the study.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a Guest Professorship of the Nagoya University awarded to KM.