
Abstract
Objective:
The main objective of this study was to obtain efficacy data for external trigeminal nerve stimulation (e-TNS) in the acute treatment of migraine in patients using the device at home.
Methods:
This was a single-center, open-label trial conducted at the Rochester Clinical Research Center (Rochester, NY, USA). Patients who met International Classification of Headache Disorders, Third Edition, criteria for migraine with and without aura for ≥1 year and having between 2 and 8 moderate or severe attacks per month were recruited. Patients were advised to treat one migraine attack of moderate to severe intensity that started less than 4 h earlier and was not treated with an acute migraine medication, with a 2-h e-TNS session. Primary outcome measures were pain freedom at 2 h and most bothersome migraine-associated symptom (MBS) freedom at 2 h. Secondary outcome measures were pain relief at 2 h, the absence of migraine-associated symptoms at 2 h, the use of rescue medication between 2 and 24 h, and sustained pain freedom at 24 h.
Results:
Fifty-nine subjects were included in the study, and among them, 48 subjects were eligible for the modified intention-to-treat analysis. After 2 h of e-TNS, 35.4% of the subjects were pain-free, 60.4% were MBS-free, 70.8% had pain relief, and 45.8% were free from all migraine-associated symptoms. Half of the subjects took rescue medication between 2 h and 24 h, and sustained pain freedom at 24 h was achieved for 25.0% of the subjects. Regarding safety, 15 patients reported adverse events, all minor and fully reversible, mainly forehead paresthesia.
Conclusions:
This study shows that e-TNS with the Cefaly® Acute Device is effective, well-tolerated, and safe for the acute treatment of migraine in patients using the device at home. A large, multicenter, randomized, sham-controlled trial is needed to confirm this finding.
Introduction
Several pilot studies 1 –3 and a postmarketing survey in Europe 4 have shown the effectiveness of external trigeminal nerve stimulation (e-TNS) for the acute treatment of migraine. A multicenter, randomized, sham-controlled trial 5 confirmed its efficacy and safety and led to US Food and Drug Administration (FDA) clearance of e-TNS for the acute treatment of migraine with or without aura. The trial took place in the hospital setting under the supervision of research staff. So far, no data are available for patients using e-TNS by themselves at home, in the early stages of a migraine attack. 6,7 The objective of this open-label pilot trial is to provide some preliminary efficacy data for e-TNS in the acute treatment of migraine in patients using the device at home, in preparation for a phase 3, multicenter, randomized, controlled trial.
Methods
Standard protocol approvals and patient consents
The study protocol and the informed consent form were reviewed and approved by the IntegReview Institutional Review Board (protocol number 50803). Written informed consent was obtained from all participants.
Study design
This trial was a single-center, prospective, open-label clinical trial conducted at the Rochester Clinical Research Center (Rochester, NY, USA).
Patients were recruited from a research site database and were screened during a visit to the research site. Patients had to meet all inclusion criteria and none of the exclusion criteria listed in Table 1. For exclusion criteria number 14, they were given training in how to use the e-TNS device, and they tested the device on themselves for a 20-min session to learn the appropriate use of the device and the electrode.
Inclusion and exclusion criteria.
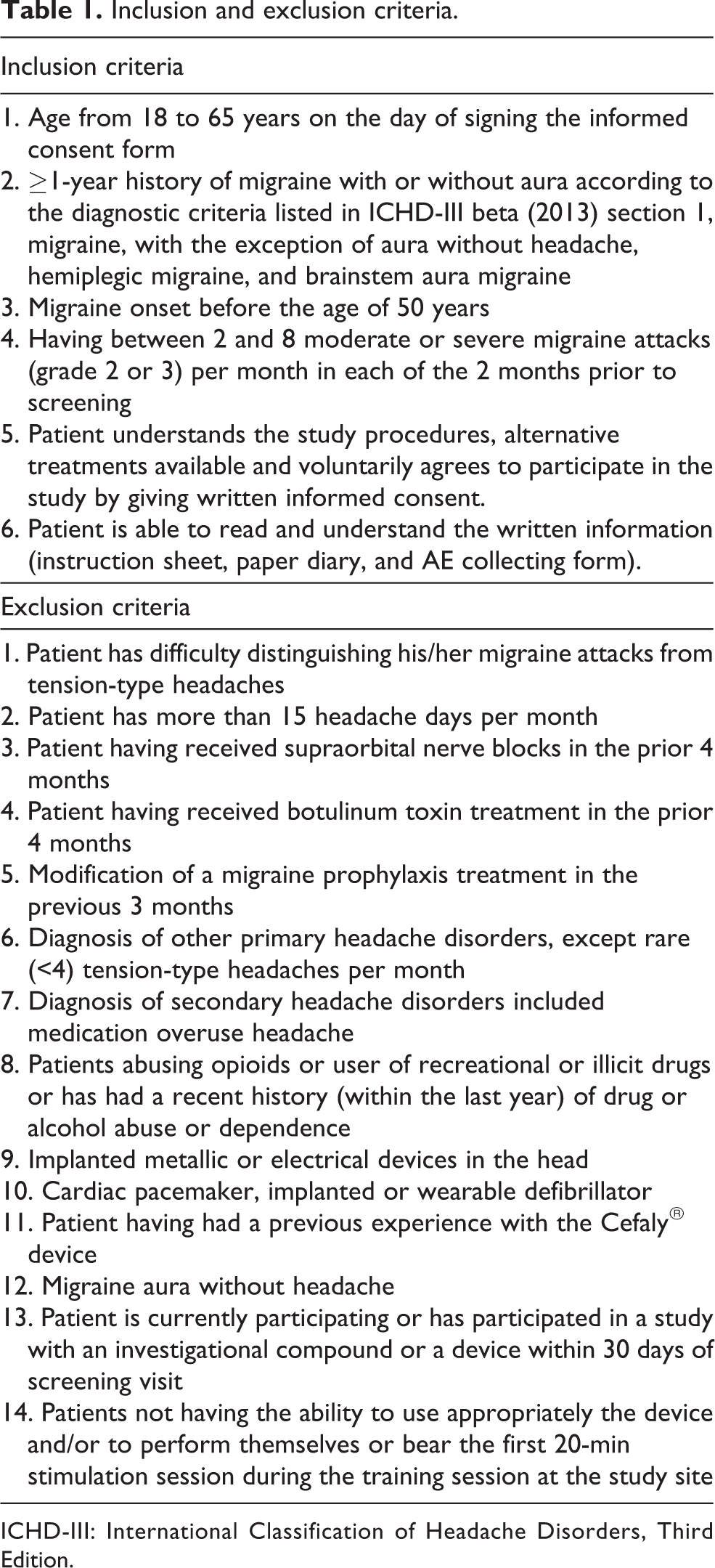
ICHD-III: International Classification of Headache Disorders, Third Edition.
Included patients were given a device and a headache diary to keep with them for 2 months to be used on a single qualifying migraine attack.
To qualify, the migraine attack had to meet the following criteria: a migraine with moderate or severe headache pain severity (grade 2 or 3) and with at least one migraine-associated symptom, being photophobia, phonophobia, nausea, and/or vomiting. The headache had to have started less than 4 h before the use of device, or the patient woke up with a migraine. Patients could also not have had another headache in the previous 48 h. Patients were also advised not to start using the device on a migraine resolving spontaneously or if acute anti-migraine medication had been taken since the beginning of the attack.
During the acute treatment phase, patients reported the following data in their headache diary: (1) headache pain severity on a 4-grade scale (0 = no pain; 1 = mild pain; 2 = moderate pain; 3 = severe pain); (2) migraine-associated symptoms (photophobia, phonophobia, nausea, and/or vomiting); (3) which migraine-associated symptom was their most bothersome symptom (MBS). These data were recorded at baseline, that is, just before the start of the e-TNS session, and also at 2 and 24 h after the start of the treatment session.
The overall study design flow is illustrated in Figure 1.

Study design flow. MBS: most bothersome migraine-associated symptom; e-TNS: external trigeminal nerve stimulation.
Patients were instructed not to take any acute anti-migraine medication within the 2-h acute treatment phase and to document the intake of any rescue medication during the 24 h following the start of the e-TNS treatment.
The e-TNS session duration and intensity were recorded for each patient by the device. Patients recorded all adverse events (AEs) date, nature, treatment (if any), and progress in an AE collecting form. Patients were instructed to notify the investigator immediately for any serious or severe AE with the stimulation.
Neurostimulation
Neurostimulation was applied with an e-TNS device (CEFALY Technology, Seraing, Belgium) for a 2-h session, as the outcome analysis reported in the article on the acute migraine therapy with external trigeminal neurostimulation trial, 5 the ACME trial, suggested that a 2-h e-TNS treatment session seems more appropriate than a 1-h session. The device is a constant current generator for a maximum skin impedance of 2.2 kΩ that delivers rectangular biphasic symmetrical pulses with a zero electrical mean. The pulse frequency is 100 Hz and pulse width 250 µs; the total dose of current delivered during a 2-h session is 2.728 coulomb. 8 The intensity increases linearly to reach a maximum of 16 mA after 14 min and then remains constant for 106 min. The electrical pulses are transmitted transcutaneously via a supraorbital bipolar self-adhesive electrode (30 × 94 mm2) placed on the forehead and designed to cover and excite (trigger action potentials) the supratrochlear and supraorbital nerves bilaterally.
Outcome measures
There were two primary outcomes in this study. The first primary outcome was pain freedom at 2 h, defined as the percentage of patients who were pain-free at the 2-h timepoint. The second primary outcome was MBS freedom at 2 h, defined as the percentage of patients with absence at 2h of the MBS they identified at baseline.
The secondary outcomes were as follows: (1) pain relief at 2 h: defined as the percentage of patients having a reduction of a moderate (grade 2) or a severe (grade 3) migraine headache at baseline to mild (grade 1) or no headache (grade 0) at 2 h; (2) percentage of patients with the absence of photophobia, phonophobia, nausea, and vomiting at 2 h; (3) percentage of patients who took rescue medication between 2 and 24 h; and (4) sustained pain freedom at 24 h: the percentage of patients having no headache at 2 h, with no use of rescue medication and no relapse of headache pain within 24 h.
Statistical analysis
The analysis was carried out on a modified intention-to-treat (mITT) basis. Patient data were included in the mITT analysis if all the three following conditions were met: (1) the patient had a qualifying migraine, (2) the patient applied the treatment, and (3) at least one posttreatment measurement was reported at 2 h.
The safety analysis was performed on all patients who underwent at least the e-TNS training session.
Continuous data were summarized by the number of patients (N), the arithmetic mean, and the standard deviation when appropriate. Categorical data were summarized by absolute (N) and relative (%) frequency tables. For each patient, the outcome was calculated according to all data available, and if necessary, imputation of missing data was conducted according to the last value carried-forward method.
The sample size was computed based on the primary outcome, that is, pain freedom at 2 h. Although this study was an open-label trial, one of the objectives was dimensioning a future phase 3, sham-controlled trial. A theoretical placebo response was therefore used in the computation of the sample size. The rate of pain-free patients is expected to be similar to triptans, so a target of 32.2% (from SAMURAI study on lasmiditan) 9 was used in the computation. A placebo effect of 7.7% has been reported for e-TNS in a previous trial. 5 The resulting power analysis showed that a sample of 42 patients allows detecting a statistically significant difference between 32.2% and 7.7% with a power of at least 80% and a level of significance of 5%. Considering a rate of 30% of patient loss during the study, at least 60 patients should be assessed for eligibility.
Results
Between August 11, 2017, and January 26, 2018, 60 patients were assessed for eligibility, of whom 59 met eligibility criteria. One patient met exclusion criteria (number 14) (it is the number of the exclusion criteria, see Table 1) (the electrode had not been correctly stuck) and was not enrolled. Of these 59 patients, 48 were eligible for the mITT analysis and 11 were not for the following reasons: one patient was lost to follow-up, two patients did not have a qualifying migraine, six patients did not report measurements at 2 h, and two patients took rescue medication within the 2 first hours (Figure 2). No data were missing for the patients in the mITT analysis.

Study participant flow. mITT: modified intention-to-treat.
Patient demographic data are detailed in Table 2. The pain intensity at baseline was moderate (grade 2) for 68.8% of patients and severe (grade 3) for 31.2%.
Demographic data.

mITT: modified intention-to-treat; MBS: most bothersome migraine-associated symptom; SD: standard deviation.
Data are expressed as n, n (%), or mean ± SD where appropriate.
The most reported MBS at baseline was photophobia (56.2%). Nausea and phonophobia were the second and third most reported MBSs at baseline (22.9% and 18.8%, respectively). Only one patient (2.1%) reported vomiting as the MBS at baseline.
Of the 59 patients included in the trial, 15 patients reported at least one AE. All AEs were minor and fully reversible. Of the reported AEs, the majority were uncomfortable paresthesia (various forehead sensations including burning, itching, tingling, stinging, and numbness) that prevented four subjects to use the device during the acute treatment phase.
Performance results are summarized in Table 3. At 2 h, 17 patients (35.4%) were pain-free, 29 (60.4%) were MBS-free, 34 (70.8%) achieved pain relief, and 22 (45.8%) were free from all migraine-associated symptoms. Sustained pain freedom at 24 h was achieved for 12 patients (25.0%), and 24 patients (50.0%) took rescue medication between 2 and 24 h.
Performance results.

mITT: modified intention-to-treat; MBS: most bothersome migraine-associated symptom.
Data are expressed as n (%).
Concerning the compliance to the treatment, 42 of the 59 included patients (71.2%) applied the e-TNS during a 2-h session for a qualifying migraine. In the 17 others, four patients did not bear the sensations and were unable to complete the session, one patient stopped early because of ineffective treatment, one patient was lost to follow-up (without data available on device use), two patients did not treat an attack, and nine patients faced a practical problem during the session (two patients reported they could not switch on the device, two reported the device and/or the electrode felt down, the five others did not report why the device stopped before the end of the session).
Discussion
This study is a single-center, open-label trial, and therefore, no control group was incorporated to assess the treatment effect. The main objective of this study was to have a pilot feasibility assessment of safety and efficacy of a 2-h e-TNS session for the acute treatment of a qualifying migraine at home in accordance with FDA guidance for trials on the acute treatment of migraine. 7 Compliance, safety, and efficacy data were needed to determine the interest and sample size for a large, randomized, sham-controlled, phase 3 trial.
The compliance to the treatment was satisfactory as 71.2% of the included patients completed the 2-h session to treat a qualifying migraine at home.
As in previous clinical trials with e-TNS for acute migraine treatment, 1 –3 reported AEs were minor and fully reversible. The main reported AE was uncomfortable forehead skin paresthesia that prevented four of the 59 enrolled patients (6.8%) to apply the full treatment during a qualifying migraine attack. Considering that 48 patients were eligible for the mITT analysis, 8.3% did not tolerate the paresthesia feeling during the migraine attack likely because of increasing cutaneous allodynia and low nociceptive threshold during a headache. 10 This reason is likely as these same patients tolerated the initial e-TNS training session when they were headache free. No patients were excluded from the study during the screening phase due to intolerance to paresthesia.
The results showed that 35.4% of patients achieved pain freedom at 2 h, and 25.0% achieved sustained pain freedom at 24 h. Regarding migraine-associated symptoms, 60.4% of patients were MBS-free at 2 h (especially those with photophobia and phonophobia), and 45.8% of patients had no symptoms at 2 h. A total of 34 patients (70.8%) achieved pain relief at 2 h. Regarding rescue medication, half of the patients took rescue medication after the treatment session.
Placebo-controlled trials related to usual acute anti-migraine medications having used the same study protocol design (qualifying migraine, mITT) and outcomes have reported similar figures for pain freedom and MBS freedom at 2 h, pain relief at 2 h, and sustained pain freedom at 24 h. 11 –15 However, the difference in the type of trial (open-label vs. placebo-controlled trials) limits comparison between the results of this trial and the results of the randomized controlled trials with acute anti-migraine medications. Nevertheless, the outcomes of this study indicate a probable efficacy of e-TNS for the acute treatment at home of qualifying migraine attacks and confirm the need for further randomized controlled clinical trials.
Conclusion
The compliance, safety, and efficacy data of this pilot trial about e-TNS for the acute treatment of migraine attack at home are encouraging and justify the need for further research.
Clinical implications
This is the first trial of e-TNS for the acute treatment of a qualifying migraine attack at home and using protocol design and outcome according to FDA and International Headache Society (IHS) guidance. The use of e-TNS at home by the patient during a qualifying migraine attack is safe and does not meet compliance issue. The efficacy of e-TNS at home by the patient during a qualifying migraine attack seems similar or higher than with usual acute anti-migraine medication and has to be confirmed by further randomized controlled trials.
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Deena Kuruvilla has received consulting fees from Amgen, Lilly, Allergan, and GLG Consulting Group. Dr Joseph I Mann has no conflicting interests. Dr Jean Schoenen has received honoraria from CEFALY Technology as an external consultant; outside of the submitted work, he has received research grants from Electrocore and Medtronic, as well as personal fees from Allergan and Novartis. Sophie Penning is an employee of CEFALY Technology. None of the authors are on the sponsor’s medical board.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study received funding from CEFALY Technology.