
Abstract
Elements of Common Mental Disorders (CMD) like stress, depression and anxiety are significant contributors to the global burden of disease. Even though they affect people at all socioeconomic levels, most of those in the low-income and middle-income populations lack access to efficient psychological and pharmaceutical interventions. One potential solution to this issue is the application of indigenous low-intensity psychological interventions like Yagna Pathy. The current cross sectional pilot study includes a total of 426 heterogenous group of people suffering from Stress, Anxiety and Depression (both in normal and diseased range) received Yagna pathy for 30 days. The severity of the stress, anxiety and depression was evaluated using a validated depression, anxiety, and stress (DAS) score questionnaire. A significant association (chi square, p < 0.001) was found between the mental healing with gender and activity status of the participants. Strong inter-correlation (R2 > 0.7; p < 0.001) among features of stress, anxiety and depression also proved the manifoldness of the CMD. Improvements in DAS scores demonstrate the effectiveness of a well-directed Yagna practice maintained for a predetermined amount of time in managing stress, anxiety, and depression. The receiver operating characteristic (ROC) of the responses was also found to be “excellent”. Therefore, the study showcased that indigenous practices like Yagna Pathy could effectively minimize the severity of CMD. This approach is non-medicated, non-invasive, and cost-effective, making it a practicable therapy for global implementation.
Introduction
According to WHO, Common Mental Disorders (CMD) were ranked the second and sixth main causes of illness and are considered a global burden.1,2 Anxiety and depression are the two major symptoms that make up the majority of CMD. This neurotic and nonpsychotic affective disorder is designated as “common” because they are widely prevalent in the community and primary care. 3 Stress, which is characterized as any form of change that creates physical, mental, or psychological strain, intensifies this further. Still, Mental health is most neglected aspect of public health provision. 4 The pandemic has rendered mental health conditions much worse. 5 The COVID-19 pandemic, one of the global catastrophes of the present generations, has had profound and far-reaching effects on the physical and mental well-being of humankind. The pandemic disrupted people's mental peace for at least two years, and its effects continue to the present day.6-10 During the period billions of people have perished or lost their jobs. Communities and families have become strained and fractured. Young people have been denied the opportunity to learn and interact with others. Companies have filed for bankruptcy. Millions of individuals are living in poverty to date.11-13 Above all, as of 29th September 2022, 65.4 lakh people have lost their lives. 14 Therefore, the consequences retain a long-lasting effect on the mental wellness of people. The evidence of the same can also be perceived by both cross-sectional15-18 and longitudinal investigations,19-21 that have looked at the psychological effects for patients. Studies have shown that those who have been quarantined have a higher prevalence of psychological symptoms, emotional disturbance, melancholy, stress, mood swings and irritability, sleeplessness, post-traumatic stress symptoms, hostility, and emotional exhaustion. Notably, other psychological reactions to quarantine include fear, rage, anxiety, insomnia, perplexity, grief, and numbness.22-24 A delayed return to normalcy even months after the quarantine as well as long-term behavioral modifications like attentive handwashing and avoiding crowds were also documented. Anxiety and trepidation have a big impact on everyone in society. According to recent studies, those who are quarantined or kept in isolation exhibit higher than usual levels of tension, wrath, perplexity, and worry.6,12,25,26 In general, every study that has examined the psychological disorders during the COVID-19 pandemic has discovered that those affected show a variety of signs of mental trauma, such as emotional distress, depression, stress, mood swings, irritability, insomnia, attention deficit hyperactivity disorder, post-traumatic stress disorder, and anger.8,16,21 Additionally, research indicates that exposure to unfortunate news about Covid-19 in the media regularly had a significant impact on mental tranquility.27-29 The present lockdown in India appears to have a diverse impact on many individuals based on their sex, occupation, socioeconomic status, or place of residence, among other factors.30-33 According to the World Bank Report of 2021, nearly 1 billion people live with a mental disorder and more than 75% of people with the disorder do not receive treatment.5,14 Thus, it is considered a burden, especially for middle- and lower-income countries.
Various interventions were prescribed to reduce mental illness during this time. Integration of conventional medicines with indigenous therapies is being advised by experts to tackle the consequences of the Covid-19 pandemic.34-38 Performing Yagna Pathy or Hawan in the household is one such noble indigenous method. In India, Yagna is considered a spiritual practice for well-being of mostly in Hindu families from ages 39 however it has also been applied as a mental health improvement from Vedic period.40,41 Yagna as a therapy for psychological ailments provides pulmonary inhalation of medicinal smoke of multiple herbs (generated through oblation in fire along with chanting of Vedic hymns), which has the potential for therapeutic results.39,42 According to existing knowledge, the best drug delivery methods for brain-related illnesses are nasal drug administration systems.43-46 Thus, inhaling the smoke originating from Hawan must have a positive impact on neurological well-being. The specific shape and size of the Agni-Kunda (Energy Field), the arrangement of wood pieces in it, and the time-frequency and amount of ingredients used in Hawan account for controlled chemical processing in the fire and lead to sublimation, chemical conversion and/or transformation into vapor phase of the herbal/plant medicinal preparation leading to release the smokes of medicinally important phytochemicals.47-49 The reference to the effectiveness of Yagna has been documented in ancient literature in Indian medicine. Acharya Charak has indicated in Charak Samhita to perform Yagna for peace of mind and cleaning of the environment in pandemic conditions to calm mental disturbance due to fear, stress, and anxiety. 50 The effect of rhythmic Vedic hymns and inhalation of medicated fume create a feeling of peace and happiness in them, and the environment also get fresh and calm as stated in Veda and other Ayurvedic literature. 39 In support of the above, contemporary studies showed the binding property of the ingredients of herbal smoke with CB2 receptors, responsible for anxiety disorders. 51 Furthermore, the components of Yagna seem to have multiple actions in preventing anxiety through scavenging free radicals, increasing in level of antioxidants, and other underlying mechanisms.47,48 Similarly, generation of the electromagnetic waves during performing Yagna could alleviate psychological depression. 52 Apart from that the anti-microbial, antioxidant, immune protective and air cleaner role of herbal smoke released from Yagna is also evident in the literature.48,49,52,53 Although several studies could provide indirect indications regarding the psychoneurological effect of Yagna, a gap regarding the validation of the same still exists. Earlier studies have tried to justify the same, but the size of the sample is too less to be significant.54-56
With the perspectives in mind, the current study seeks to examine the levels of anxiety, stress, and depression among self-reporting patients during the COVID-19 outbreak and determine whether performing Yagna as a form of intervention will help to control the disorders. As the present study falls under observational study (Cross-sectional) we have followed STROBE guidelines 57 to conduct the same.
Material and Methods
Study Design & Participants Recruitment
This present study contains a cross-sectional design. Five hundred and twenty health-seekers suffering from different common mental conditions (Stress, Depression, and Anxiety) initially approached Patanjali YogGram, Haridwar, India (Latitude: 28.64739 Longitude: 77.19265) for the treatment purpose. Patanjali YogGram in Haridwar is a renowned research facility devoted to the scientific study and use of naturopathy, yoga, and Ayurveda. This institution, which combines modern scientific research approaches with ancient Indian healing practices, is situated in a serene area close to Haridwar, Uttarakhand. The center provides a favorable setting for in-depth investigation and study into the therapeutic, psychological, and physiological advantages of Ayurvedic and yoga medicine. Comprehensive facilities, including treatment rooms, lecture halls, and specialized laboratories, are beneficial to both researchers and practitioners, fostering multidisciplinary collaboration and the growth of evidence-based holistic health methods. Overall, Patanjali YogGram is an organization that aspires to contribute to the field of local and worldwide health research.
In regard of accessing the treatment effectivity, the patients were requested to fill out the DASS-42 form before and after the intervention (treatment) process. To check the level of anxiety, stress, and depression both pre- and post-intervention online questionnaires using the Depression Anxiety Stress Scales (DASS) scale58,59 distributed through Google Forms.
The Depression, Anxiety, and Stress Scale (DASS) was selected for this study due to its comprehensive assessment of depression, anxiety, and stress (DAS) symptoms, which aligns with the multidimensional nature of mental health issues encountered in community settings. The DASS is well-established for its robust psychometric properties across diverse populations and cultural contexts, offering a reliable and sensitive tool for evaluating psychological distress. Its brevity, ease of administration, and validated scoring protocols further enhance its suitability for large-scale community-based studies, ensuring efficient data collection and rigorous analysis of interventions aimed at managing CMD.60,61 DASS-42 consists of 42 items in three categories namely DAS. Question number 3, 5, 10, 13, 16, 17, 21, 24, 26, 31, 34, 37, and 42 are regarding depression, Question number 2, 4, 7, 9, 15, 19, 20, 23, 25, 28, 30, 36, 40, and 41 are for anxiety and question number 1, 6, 8, 11, 12, 14, 18, 22, 27, 29, 32, 33, 35, and 39 are for stress. A categorization of the different dimensions is obtained by summing up the scores on the answers to the items that correspond to each of the variables. The choices available to react to this scale were: 0: did not apply to me at all; 1: applied to me to some extent or some time; 2: applied to me to a significant degree or most of the time; and 3: applied to me a great deal or most of the time; The severity ratings used to interpret are shown in Table 1.58,59 All Questionnaires were conducted in British English.
DASS Scale.

Adopted from 58
Among the responses obtained, the inclusion criteria were applied, selecting only those participants who completed the full duration of the intervention. No external medications or interventions other than Yagna Pathy were used during this period. Consequently, 426 participants (86%) were included in the study. The study design is summarized in Figure 1. All of the participants in the study at Patanjali YogGram, Haridwar, identified as Hindu, which is consistent with the cultural setting where customs such as Yagna Pathy are traditionally followed. Although there were no constraints on religion, caste, or creed in the study, it is acknowledged that the participants’ acceptance of Yagna Pathy had its roots in Hindu beliefs. The research was conducted with strict adherence to ethical principles, having received approval from an institutional review board. Procedures for obtaining consent were created with clarity and consideration for participants’ religious beliefs in mind. The participants who are taken into consideration are those who voluntarily engage in the process. This method emphasizes a dedication to moral behavior and consideration for cultural diversity in the research setting.

Design of participants recruitment for the study.
Sample Size Validation
A sample that is larger than necessary will be a better representative of the population and will hence provide more accurate results. However, beyond a certain point, the increase in accuracy will be small and hence not worth the effort and expense involved in recruiting the extra patients. Therefore, the minimum number of samples required to get statistically significant results is of utmost importance before conducting a study. Here to find the minimum sample size, we set up the statistical constraints like a 5% margin of error, 50% population proportion, and a confidence interval was 95%. Initially, we received a total of 520 applicants for the study, the population size was set up as 520. Thus, according to the formula stated below.
Yagna Pathy: The Intervention
The group of experienced experts in perfuming Hawan or Yagna used to guide the participants to do it correctly. The materials used for performing Hawan were A simple Havan Kund, one bundle of mango or any other suitable wood / Dry cow dung (Keep aside three individual wood sticks as “Samidha”), Some Camphor, 250 g Pure Havan Samagree, 250 g Ghee (Melted), Some Sweet Rice, a container with fresh water and a teaspoon, Matches/Fire lighter, A lamp to be placed in front of the Havan kund and the Havan Samgri.
As described in the book “Sankshipt Gayatri Hawan Vidhi” by Pt. Shriram Sharma Acharya, Yagya was performed. 62 This study was conducted in a big room surrounded by four walls and two windows for ventilation. Also, the four walls were coated with cow dung along with the Yagya Kunda (fire pit). The four participants were made to sit on the four sides of the Kunda. Yagya was performed in the morning during the time of sunrise with special herbal powder available from Patanjali, Haridwar, India. Dried Cow dung patties of the indigenous breed were used as samadhi (firewood) and the fire pit used was made of clay and bricks. The mantras used were the Surya Gayatri mantra and the Chandra Gayatri mantra, with 12 oblations of both mantras. The procedure was conducted for 45 min daily for 30 days.
Ethical Approval
The ethical committee has approved the study as a part of project no.
Statistical Analysis
The continuous variables of the study are presented in mean ± standard deviation and categorical variables were presented in frequency (%). For sample representativeness, the participants were compared concerning substance use and sociodemographic characteristics using Chi-Square(X2) test. In all cases, the data were analyzed for normality using the Shapiro–Wilk Test and considering the skewness and kurtosis values before the application of the hypothesis testing.
For hypothesis testing, a two-sample two-tailed z-test is used to compare the means of Stress, Depression, and Overall DASS scores in Previous and the Post-intervention. So, if the mean score of the samples (both patients and normal) before the Yagna is
The association among the CMD (stress, anxiety, and depression) with each other was found by the linear regression of the DASS scores with an estimation of person correlation and goodness of fit values.
The discriminative accuracy of the DASS was evaluated by the receiver-operating characteristic (ROC) curve analysis. 64 A ROC curve plots the sensitivity and specificity at each consecutive threshold value. The area under the ROC curve (AUC) is a suitable parameter to summarize the overall discriminative value of a screening instrument. A value of 0.70 or more can be interpreted as reasonable, 0.80 up to 0.90 as good, and 0.90 or over as excellent.64-67 Regarding the performance of all the statistical methods and plotting graphs, we have used GraphPad Prism (Ver 8) and MS EXCEL.
Results
Socio-Demographic Profiling of the Participants
Before performing Yagna Pathy, the total DASS scores (DASS-D + DASS-A + DASS-S) of 87 participants among 426 patients were found on or below 30. This implies that the said participants were under the “Normal range” according to the specified DASS table (Table 1). Similarly, the rest of the 339 patients were found to be in the diseased range (mild/moderate/severe/ extremely severe) of CMD. The above pre-screening of patients aids the study in two ways. First, we can identify the diseased range, thus the effect of the intervention on the said range can be clarified. Secondly, the effect of Yagna Pathy on the mental situation of normal-range patients could also be explored.
The internal Consistency measurement (Cronbach alpha value), for DASS-S, DASS-D, and DASS-A scores were found to be 0.71, 0.70, and 0.79 respectively for the present study, and the overall DASS score was found to be 0.737. All the values were acceptable according to the previous studies. 68
In this study, the mean age of the participants was 42.15 (±12.81) years. The females and male participants were 258 (60.56%) and 168 (39.44%) respectively. There were 328 (77%) participants who are married, and 98 (23%) participants are unmarried. Only 12 (2.82%) participants have habits of smoking, and 414 (97.18%) participants were non-smokers. 407(95.54%) participants are non-alcoholic, and the rest were 19 (4.46%) participants were alcoholic. 166 (38.97%) participants reported having medication intake for different lifestyle diseases while 260 (61.03%) participants were not using any medication. The activity status of participants is light, moderate, sedentary, and vigorous with 40 (9.39%), 323 (75.82%), 13 (3.05%), and 50 (11.74%) respectively (Table 2).
Socio-Demographic Profiling of the Participants.

Significant association at *95% Confidence Interval; **99% Confidence Interval; #According to the DASS scoring table.
Association Between the Attributes of CMD
In the current study, we have encountered patients who have stress or anxiety or depression, or any of the two or all three mental illnesses. Thus, this is obvious to probe whether there is any relation between these three mental illnesses.
The regression analysis shows the linear relationship between stress and anxiety; anxiety and depression and between depression and stress (both previous and post-performing Yagna Pathy) Moderately strong association (R2> 0.7; p < 0.001) reflect in each case (Figure 2). This strongly suggests that if someone is suffering from stress then he would have a higher possibility to develop both depression and anxiety with vice versa.

Association among stress, anxiety, and depression.
Effect of Intervention: Yagna Pathy
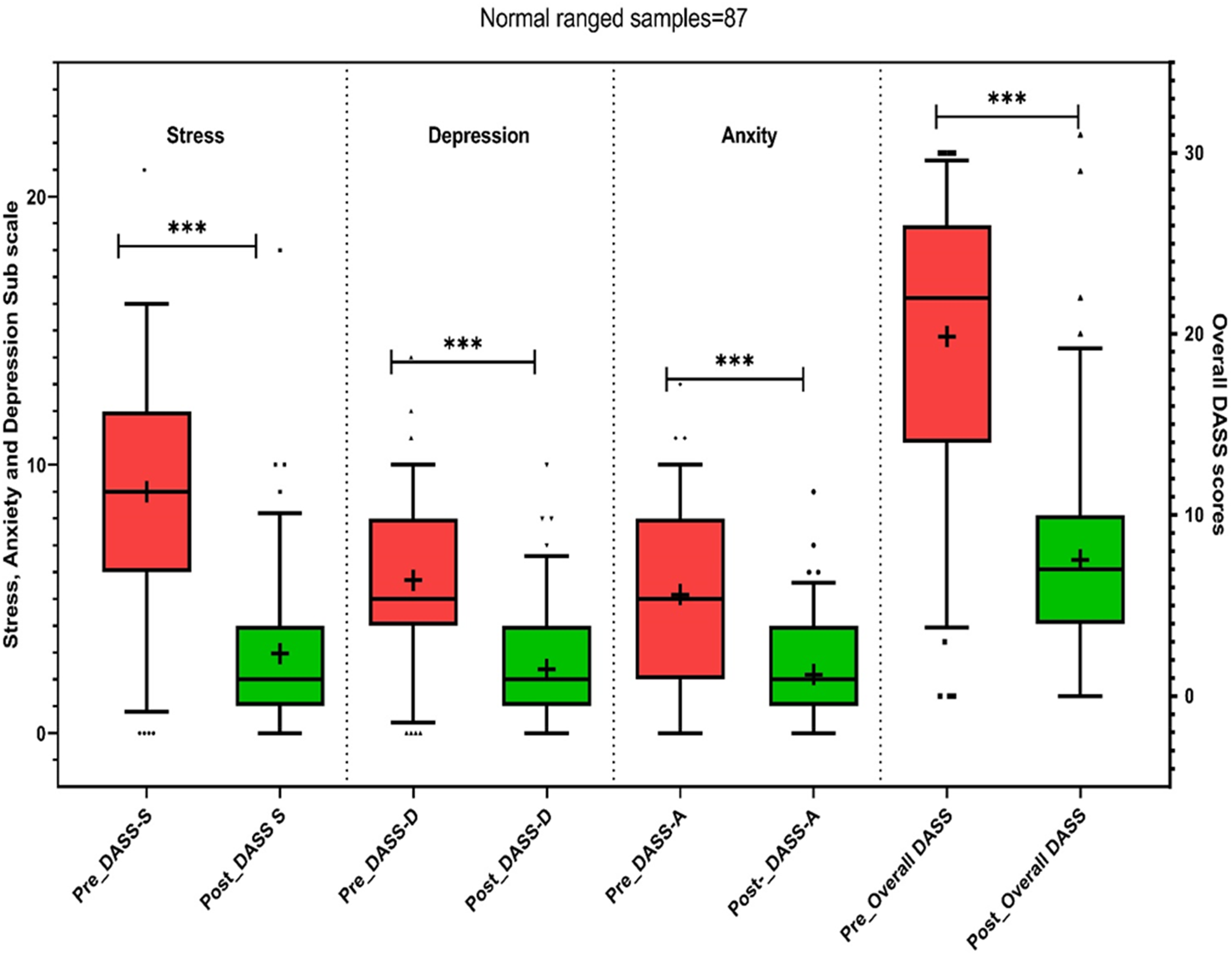
Effects of Yagna Pathy on Mean Scores of Depression (DASS-D), Anxiety (DASS-A), and Stress (DASS-S) Scales.

***p < 0.001 (Significant at 99% confidence interval); #Scores denotes the NORMAL condition of Mental Disorders; $Scores denotes SEVERE/MODERATE condition of Mental Disorders according to the DASS scoring table.
Effect of Yagna Pathy on Mental illness of patients under normal category.
This observation led us to investigate the effect of Yagna Pathy on the participants who are classified into the normal category. The Yagna Pathy also proved to retain a profound effect on the reduction of stress, anxiety, and depression in the previous manner (Figure 4) for diseased category. In this case, a 66.6% reduction was observed in DASS-S and 57.8% in DASS-D while 63.3% in the case of DASS-A. The overall DASS score of the participants under the Normal category has been reduced by 62.5% (Figure 4; Table 3). The difference between the pre- and post-mean scores was also found to be significant at a 95% confidence interval calculated by a two-tailed z- test.

Effect of Yagna Pathy on Mental conditions of patients under the diseased category.
Reliability Test
Receiver operating characteristics (ROC) is a crucial tool in reliability analysis that plays a significant role in measuring the accuracy and effectiveness of diagnostic tests. The ROC curve provides an opportunity to evaluate the trade-off between true positive rates (sensitivity) and false positive rates (1-specificity) over a range of test thresholds. To determine the cut-off values giving the best balance between sensitivity and specificity, ROC curves were computed (Figure 5A-5C).

Receiver operating characteristics (ROC) of the stress (A), anxiety (B) and depression (C).
This yielded statistically significant areas under the ROC-curves for DASS-S (AUC 0.93, 95% CI 0.92–0.95; p < 0.001) in predicting stress, DASS-A (AUC 0.89, 95% CI 0.86–0.91; p < 0.001) in predicting anxiety and DASS-D (AUC 0.88, 95% CI 0.86–0.91; p < 0.001) in predicting depression. The overall DASS score (AUC 0.92, 95% CI 0.91–0.94; p < 0.001). According to the AUCs, the overall discriminative value of the DASS-S, DASS-A, and DASS-D subscale as well as the overall DASS can be interpreted as “excellent”.
Discussion
The present study could open different avenues regarding mental wellness. First, common mental illnesses like stress, anxiety, and depression could be well expressed in people of all ages starting from adolescence to retirement age. Although we found no such significant association with age for stress and depression-affected individuals except for anxiety. Onset of anxiety disorders can also be influenced by psychological and social risk factors. Geriatric anxiety and depression share several risk factors, including female gender, cognitive impairment, chronic health issues, poor self-rated health, functional restrictions, and personality features like neuroticism and inadequate coping mechanisms.69,70 In the case of other social-demographic factors like alcohol intake, smoking habits, and medication intake, we also don’t find an association with common mental conditions. Some previous studies could prove that the effect of the above-mentioned elements has a profound effect on stress, anxiety, and depression. Perhaps in the present case, the participants are hiding or not willing to share their ill habits. Thus, the proportion of affirmative and negative cases varied significantly. One of the most promising and expected outcomes of the study was to showcase the importance of physical activity in mental well-being. We could observe a significant association between any type of physical activity that exists with stress, depression, and anxiety. In the world of modern medicine, the benefits of regular physical activity on health are without dispute. The mechanisms behind exercise's antidepressant benefits are still unknown, even though research consistently links exercise with depression. Thermogenic theory, 71 , endorphin hypothesis, 72 monoamine hypothesis, 73 distraction hypothesis, 74 self-efficacy enhancement, 75 and other plausible physiological and psychological causes have all been discussed. Most of these theories, however, have little research backing them up.
Another interesting finding of the present study is the significant strong correlation (R2 > 0.7; p < 0.05) among the subscales of DAS (DASS-A, DASS-S, and DASS-D). In both cases of pre and post-performance of Yagna therapy, the observation remains the same. This implies two conclusions, first, if someone develops any one attribute of CMD, the other two or one element of CMD that is stress or anxiety or depression, could also develop. Secondly, after the performance of Yagna Pathy, all three attributes are reduced correlatively. Thus, this can be inferred that Yagna Pathy could be fruitful for controlling CMD holistically. There was no such association with these mental disorders in previous literature till now. Thus, the present study could provide a noble avenue for further medical research.
The main goal of our study was to determine whether Yagna Pathy could have a controlling effect on CMD and if yes then to what extent? As cited in previous literature, Yagna is considered a powerful and comprehensive ancient therapy. Any type of sickness, whether somatic, mental, somatopsychic, or psychosomatic, can be improved by this therapy. Yagna is more of a religious practice but is also considered an herbal smoke therapy recommended for mental peace. Along the same lines, in this present study we could validate that the Yagna herbal smoke therapy has significantly reduced anxiety, depression, and stress (Table 2). There are three aspects of performance of Yagna which could affirmatively affect mental wellness. First, the ingredients used in the Yagna therapy led to the release of herbal smoke. Studies could prove that the ingredients are diversified and effective while they are released as herbal smoke during performing Yagna. While performing Yagna the ingredients are used to pour into the fire and mantras are chanted. The pouring is called Agni Hotra. “Agni” means ‘fire’ and “Hotra” means an ‘offering’; Agnihotra means the act of an oblation into the fire. 76 Agnihotra consists of a base fire generated in a specifically designed vessel fixed on the surface of the level ground. Burning fire of some specified characteristics forms the base fire. To this base fire specific substances like clarified butter (ghee) and herbal materials are added in the form of oblations. The detailed literature has been reviewed by Chaube and the coworkers. 48 The study also provided the information of active compounds released during the Yagna which eventually have significant effect on different parts of nervous system. Apart from that, the herbal smoke was proved to be air cleanser and could act as antifungal, anti-bacterial agent. The chanting of mantras is acted as noise therapy. 48 During the hawan, dev yagya & balivaishv dev yagya, and other mantras are chanted. The frequencies of mantras coupled with herbal smoke bring a resonance effect on the brain neurons and possibly that may bring peace of mind.77-79 Previous studies also support the same but the number of participants who participated in the studies was not significant to justify.54-56 The present study involves a significant sample size as per power analysis. Thus, it holds significant justification for the effectiveness of Yagna Pathy to control CMD.
It is crucial to maintain inclusivity and respect for different belief systems while discussing the ethical issues surrounding the use of Yagna Pathy as a therapeutic intervention, especially in a country with a diverse population in terms of culture and religion like India. Yagna Pathy is based on Hindu spiritual practices, hence those from non-Hindu backgrounds could find it difficult to participate if it goes against their own spiritual or religious views. Our study followed ethical guidelines that prioritize informed consent and cultural sensitivity in order to manage these challenges. Before participating, participants received thorough information about the spiritual and cultural aspects of Yagna Pathy, enabling them to make an informed choice based on their personal tastes and beliefs. Furthermore, Yagna Pathy's applicability must be expanded beyond Hindu communities in India and around the world, which calls for careful cultural adaptation and respect for various religious viewpoints. By adopting cultural competence concepts and customizing procedures to conform to local customs, comparable indigenous healing techniques have been successfully incorporated into mental health care systems around the world. 80 Subsequent investigations ought to go into methods for modifying Yagna Pathy to encompass a wide range of religious and spiritual traditions, thereby expanding its applicability and approval as a mild psychological remedy.
In conclusion, researchers can promote an atmosphere of respect and inclusivity by proactively addressing these ethical dimensions. This will guarantee that Yagna Pathy and other indigenous healing techniques positively impact mental health care without unintentionally marginalizing or excluding people based on their spiritual or religious affiliations.
Limitation of the Study
The study's reliance on quantitative data analysis may have limited the investigation of complex reactions and unique experiences because it did not use qualitative techniques, such as focus groups or in-depth interviews, to record participants’ subjective experiences and feedback.
The participant population was homogeneous, consisting exclusively of individuals who identified as Hindu, which may restrict the generalizability of findings to populations with diverse religious and cultural backgrounds.
Biochemical or brain imaging results that could provide a more precise correlation with the DASS questionnaire outcomes were not obtained, limiting the ability to establish exact physiological correlates of the observed mental health outcomes.
The study did not investigate the dose-dependent effects of Yagna Pathy on prevalent mental diseases, which could have provided insights into the therapeutic efficacy of these interventions across varying levels of treatment intensity.
Due to the cross-sectional design of the study, causal relationships between variables could not be inferred, highlighting a limitation in establishing temporal or cause-effect relationships among the observed variables.
Conclusion
In conclusion, Yagna Pathy, rooted in ancient literature, transcends religious, caste, and creed boundaries, making it accessible to all. The findings highlight the practical implications of Yagna Pathy, emphasizing its potential as a cost-effective, non-invasive and low-intensity psychological interventions for managing mental wellness. The study contributes to a deeper understanding of alternative mental health treatments and underscores the importance of integrating traditional practices into contemporary healthcare approaches. Moving forward, further research could explore broader applications and long-term benefits of Yagna Pathy.
Footnotes
Acknowledgments
The authors would like to thanks revered Swami Ramdev Ji Maharaj for his constant support and inspiration to execute the study. The authors are thankful to the Ministry of AYUSH under Grant-in-Aid for the Establishment of the Centre of Excellence of Renovation and Upgradation of Patanjali Ayurveda Hospital, Haridwar, India.
Authorship Contribution Statement
Acharya Balkrishna: Conceptualization, Funding acquisition, Sourav Ghosh: Writing – original draft and Reviewing, Data curation, Formal analysis, Anuradha Gupta: Methodology, Data curation, Vedpriya Arya: Writing - review & editing, Project management.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Ministry of AYUSH, Government of India under the AYURSWASTHYA Yojana (Z.15015/12/2018-COE).
Ethical Approval
The ethical committee has approved the study as a part of project no.