
Abstract
Background
Variety of conventional treatments are used to treat cancer. Cancer patients adopt other alternative therapies including medicinal plants. Their curative power results in the presence of secondary metabolites in its different parts. However, they can have toxic effects and interactions with conventional treatment and even chemosensitivity of the cancer cells.
Objectives
This study aims to determine the prevalence of the use of medecinal plants by cancer patients undergoing chemotherapy, list the medecinal plants used, identify the most consumed, present the reported adverse effects and determine the predictive factors of their use.
Materials and Methods
This was a cross-sectional study of 203 patients followed at the National Institute of Oncology in Rabat from 01 October 2018 to 30 November 2018. Regarding socio-demographic and clinical characteristics and data on the use of medicinal plants were collected from a questionnaire.
Findings
of 203 patients, 37% used medicinal plants. 30 plants also the honey were identified during this study. The “euphorbia honey"was consumed at (40%), The most used plants were garlic (13%), turmeric, fenugreek and thyme (11% each). 5% of patients presented side effects related to the consumption of medicinal plants. There is a significant association between the use of medicinal plants and socio-economic level (p = 0.004) and duration of illness (p = 0.048).
Conclusion
This study revealed a high prevalence of medicinal plants used by cancer patients receiving chemotherapy at National Institute of Oncology. The more clinical studies are desirable to demonstrate the efficacy of medicinal plants and their therapeutic effects to encourage their consumption or prohibit them.
Introduction
Cancer is a major public health problem in the world. Its incidence is increasing worldwide. 1 According to the International Agency for Research on Cancer, the number of new cancer cases in 2020 is 19.2 million and the number of cancer deaths was 9.9 million. 2 In Morocco, it is estimated that in 2020, 59.370 new cases of cancer are diagnosed and number of deaths was 35.265. 3 To treat the disease, doctors use a variety of conventional treatments including surgery, radiotherapy, chemotherapy, immunotherapy and targeted therapies. 4 However, as with any drug, these therapies have many side effects. To remedy these problems and cure their disease, cancer patients adopt other alternative therapies such as medicinal plants (MP). In the United States and developing countries, more than 35% and 50% of cancer patients use these remedies during chemotherapy. 5 In a study carried out in Morocco, 35% of cancer patients on chemotherapy use herbal medicines. 6 The reasons for the use of alternative and complementary medicine, including MP, are the relief of moral suffering related to the disease, stimulation of the immune system, relief of disease symptoms, prolongation of survival, reduction of side effects of prescribed treatments and cure of the disease. 7 Plants are more accessible than drugs because they are available in nature. 8 These natural products are the source of 60% of the anticancer agents used today. 9 More than 3.000 species worldwide have anti-cancer properties. 10 The curative power of MP results in the presence of secondary metabolites in its various parts including terpenoids, phenolics, alkaloids, flavonoids and compounds containing sulphur. 11 However, they may have toxic effects and interactions with conventional treatment and even chemosensitivity of cancer cells. 12 The interaction produced by herbs may be more important than that of the drug-drug. 13 Some natural supplements can affect the enzymes such as cytochrome P450 and anti-cancer drug carriers (ABCB1 and ABCG2). This can alter their plasma concentrations and cause severe toxicities or a decrease in treatment efficacy. 14 This study aims to determine the prevalence of the use of medecinal plants by cancer patients undergoing chemotherapy at National Institute of Oncology (NIO) in Rabat, list the medecinal plants used, identify the most consumed, present the reported adverse effects and determine the predictive factors of their use.
Materials and Methods
Study Design
This is a cross-sectional study that was carried out from 01 October 2018 to 30 November 2018 at the oncology and radiotherapy departments of NIO in Rabat.
Participants
The sample of the present study used a national average prevalence at 40% calculated from the results obtained in the national surveys of the use of MP in cancer patients. A confidence interval was 95% and a margin of error was 7%. The study sample was 188 patients. A majoration was made to eliminate the losses associated to the field investigations. The people who were included in this study are patients undergoing chemotherapy alone or concomitantly with radiotherapy, inpatients and outpatients and patients who are older than 16 years of age, of different sexes, present during the study period, expressing their willingness to participate in the study, and who are able to complete the questionnaire or to answer the interviewers.
The people excluded from this study are the patients who refused to participate in the study.
Ethical Approval and Consent to Participate
An ethical approval for this survey was obtained by the Ethics Committee for Biomedical Research under N° 27/18. After explaining the subject to the patients, clarifying the purpose of the study and having their agreement to participate in the study, the participants patients gave their agreement and signed a written consent. All participants (203) gave their consent to participate in this study
Questionnaire
In order to collect data, a questionnaire was used. The questionnaire was translated into dialectal Arabic and then tested with 10 people to assess the quality of the translation and its clarity. These 10 tested questionnaires are not counted in the study.
The first part of questionnaire was related to clinical and demographic characteristics (gender, age, middle of origin, education, socio-economic level, profession, marital status, disease case type, duration of illness and cancer type). The seconde part included 16 items related to the use of medicinal plants, their number, reason for use, person advising their use, difficulty of provisioning MP, time of use, protocol followed for use, part used, method of use, frequency, quantity consumed, duration, information on medicinal plants and their risk, reactions developed and finally the improvements felt. The 30 plants in this study were collected from the participants’ answers to the open question, what plants do you use? Also for the reasons, informations and improvements. These questions have been asked: why do you use medicinal plants?. Do you have any informations about the plants that do you use? If yes, what are this informations? Have you felt any improvement after taking MP? If yes, what are these improvements? The honey has been cited because is derived from the Euphorbia. The participants did not want to consume this plant for its toxicity, they prefer to consume the honey derived from this plant.
One plant was not identified by its user
Data Collection
After agreement to participate in the study was obtained, the objectives have been clarified to participants and an informed consent was signed by them. All patients willing to participate have filled out or responded to the interviewers and returned the questionnaire. For patients able to read and write, they responded to the questionnaire themselves, for the illiterates, they only answered the questions asked in a verbal form by interviewers. The data collection was carried out by the corresponding author and a low participation of two volunteer investigators.
Data Analysis
The statistical analysis of the data was done by IBM SPSS version 23. Qualitative variables were expressed in frequency and percentage and quantitative variables in average. A Pearon's chi-squared test was used to compare MP users and non-users. Univariate analysis was done to determine the association between sociodemographic, clinical parameters and MP use. 10 variables were used for this analysis especially (sex, age, middle of origin, education, socio-economic level, profession, marital status, disease case type, duration of illness and cancer type). Multivariate analysis was used to determine factors predictive of MP use. P value < 0.05 was used to determine that the association is statistically significant.
Result
Characteristics of Participants
The response rate was 100%. Of the 203 patients interviewed, 138 were female (68%), the average age was 50 years, the most affected age group was 40–60 years (51%), 73% were from rural areas, half of the participants were illiterate. 52% had an average socioeconomic level, 84% of the respondents were inactive (without a job), the average duration of the disease was 29 months, 75% had a cancer lasting more than 6 months. The most frequent type of cancer was gynecomammary cancer (49%). (Table 1)
Socio-demographic and clinical characteristics of MP user and non-user participants.

*digestif: digestive concerns cancers of the colon, stomach, esophagus and rectum.
Use of MP
75 (37%) of the participants reported using MP. As female participants had higher percentage of using MP remedies (69%), new cases (patients who are recently diagnosed) (65%), illiterate (43%), married (68%), with gynecomammary cancer (52%), aged 40–60 years (53%), inactive (81%), living in rural areas (73%), with average socioeconomic status (67%), and with a duration of illness greater than 6 months (65%) (Table 1).
The use of MP was encouraged mainly by the patients’ entourage (55%). 95% of users have consumed these remedies without a precise and identified protocol. 73% of the respondents found no difficulty in provision of MP. 61% of the patients consumed only one plant. The most common amount of MP consumed was one spoon (61%). The time of use was mostly before chemotherapy (65%) with the most reported frequency of use being once a day (59%). As consupmtion of MP for more than 2 years wasfounded in 64% of patients. MP were taken with water in 35%. The most used part of MP were seeds (27%). (Table 2).
Use of MP.

Types of Plants Used
30 plants were used by patients treated with chemotherapy. Different plants were reported (Garlic, turmeric, thyme, fenugreek, sage, dried fig, onion, linseed, black cumin seed lemon, rosemary, white marrube, nigella seed oil, saffron, salt, cider vinegar, caraway, sesame, green anise, apricot nuts, dried apricot, grapes, fine, Senna, lavender, aleo vera, cade and Pouliot mint) also the Bees products as “euphorbia honey” and propolis.
The “euphorbia honey” is very much evoked by the patients with 40%, garlic occupied the second position with 13%, turmeric, fenugreek and thyme were consumed at 11%. (Table 3).
Types of MP used and their frequency by location.

Reason for Using or not Using MP
The most reasons cited by respondents was cancer treatment (60%). For the non-users, the fear of the adverse effects of MP are the most registered (57%) (Table 4)
Reasons for using or not using MP and information on MP and its risks.

Information on MP and Their Risk
57% of the users had no information about the plants which they use. The most information recorded were cancer treatment (37%). 96% of users were ignorant about the risk associated to MP use. (Table 4).
Improvement and Reported side Effects
61% of users reported improvements as a result of MP consumption. 39% felt no improvement. Strengthening of immunity was the most evoked as improvement (37%). 95% of user had no adverse effects related to the use of MP however 5% reported these effects. (Figure 1)
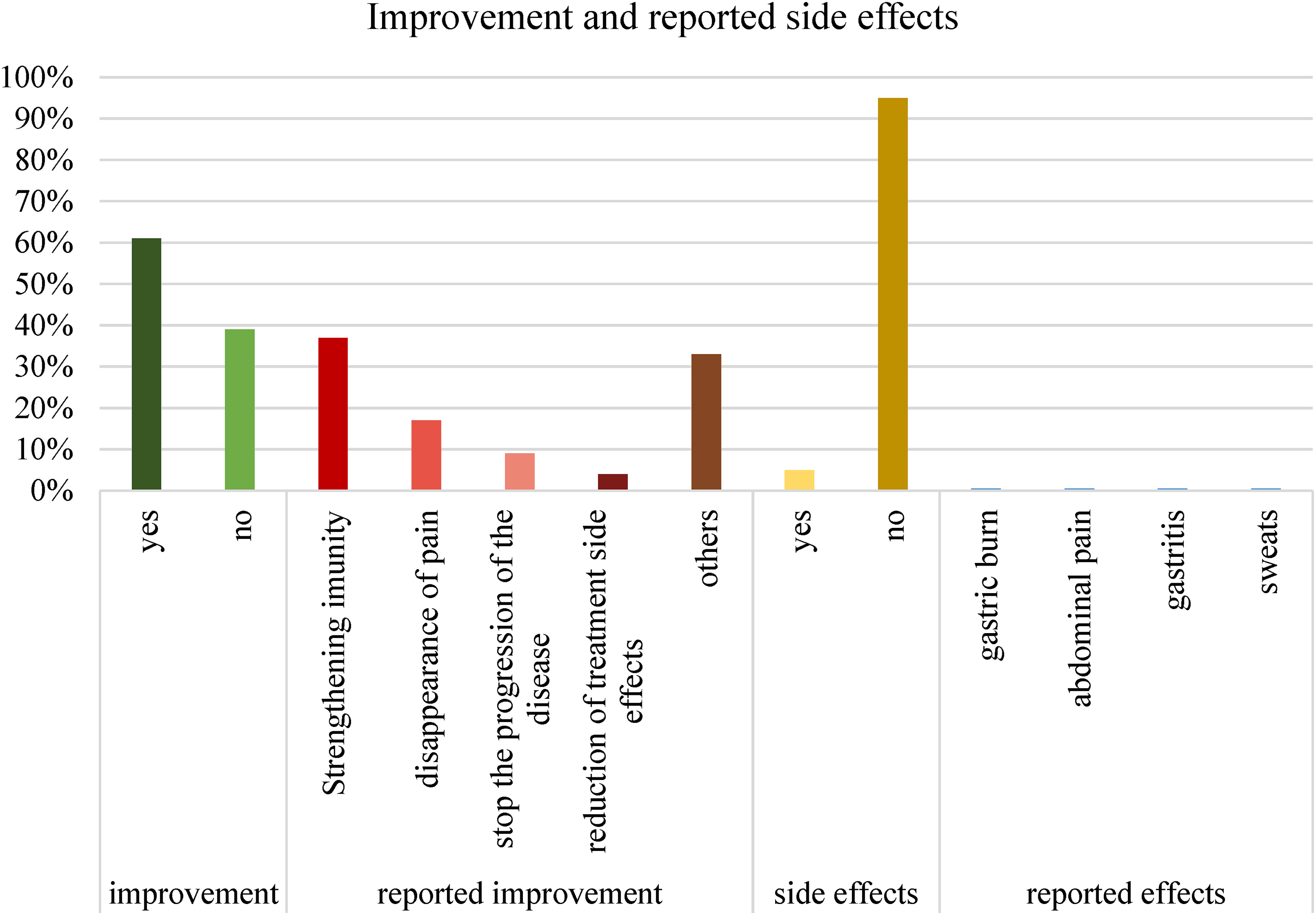
Improvement and reported side effects.
Predictors of MP use
A univariate analysis was used to calculate the OR to assess the association between socio-demographic (sex, age, middle of origin, education, socio-economic level, profession, marital status), clinical characteristics (disease case type, duration of illness and cancer type) and the use of medicinal plants. There was an association between socioeconomic level and the use of MP (OR: 0.38, 95% CI: [0.21-0.70], P = 0.002). Also for the duration of the disease (OR:2.18, 95% CI [1.14-4.17] P = 0.018). There was no association between the other variables and MP use. In multivariate analysis, the two significant predictors of the use of MP proven in the univariate analysis have remained significant as socioeconomic level (OR:0.41, 95% CI [0.22-0.76] P = 0.004) and duration of disease (OR:1.95, 95% CI [1.00-3.78] P = 0.048) (Table 5).
Predictors of MP use.

Discussion
This research complements and enriches previous Moroccan research on the use of MP by cancer patients in Morocco.The use of medicinal plants in cancer care in Morocco is between 24% and 68%.7–17 For ethnic chinese cancer patients in Asia this rateis is between 25% and 98% and for those living in North America the prevalence of use is between 25% to 47%. 18
According to this results, the prevalence of MP use is 37%, which is consistent with previous national research6,7,16,17 and some studies in other countries,19–21 but higher than those found in the UK 22 and lower than that found in Iran, 23 Palestine, 24 anapolis, 25 China, 26 America 27 and Brazil. 28 Although oncologists have educated and prohibited these remedies to patients undergoing chemotherapy, by delivering premedication prescriptions mentioning the proscription of MP consumption, patients continued to use these remedies perhaps for more efficiency and to have healing results in a short time. This can also be due to the influence of the entourage shown by our research (55%). As well as the media, which constantly draws attention to the use of medicinal plants in the treatment of diseases. On the other handand phytotherapy is part of Moroccan culture 29 and people easily got medicinal plants and didn't need a prescription, 16
Our study revealed that women used MP more than men, which is coherent to national studies4,16,17 and international studies.22,25,26 This use was justified by the oral transmission of traditional practices from mothers to daughters, 16 the rate of illiteracy and the attachment to traditional medicine, 17 the women are more concerned in the curing process and are also responsible for the dissemination of popular practices 25 and they have more knowledge of phototherapy. 4
Results of our survey revealed that patients with duration of illness more than 6 months are susceptible to use MP, this was also confirmed by damary et al. 22 This may be a reason to manage the effects therapy for cancer of long term. 22
Our research shows that the users of medicinal plants are illiterate. This is similar to the study conducted in the region of maknes-tafilalet. 4 It may be due to traditional knowledge of medicinal plants wich is verbally passed from generation to generation rather than the traditional organized education system. 4
We identified that patients with a average level used more MP while other previous studies confirmed that MP users had a low socioeconomic level16,17 and Damary et al found that the two wealthiest deprivation quartiles used more MP compared to the most deprived quartile. 22
30 medicinal plants were identified during this study. Previous studies have confirmed high numbers3,4,16,17,23,28,30–32 while other studies have shown low numbers.25,33–36
This results show that participants uses more “euphorbia honey” (40%), garlic (13%), turmeric, fenugreek and thyme (11% each). The frequent use of fenugreek and turmeric by cancer patients has also reported by some previous Moroccan studies.4–17 Other studies have also revealed the frequency of use of garlic22,23–25 as well as the use of turmeric22–37 and also for thyme. 37
These remedies have been studied in various studies for their anticancerous effects. Hamada Imtara and al demonstrated the presence of certain phenolic compounds in the “euphorbia honey” (Daghmouss) which is the most evoked during our study. It contains syrinic acid which has antioxidant activity capable of eliminating free radicals, it also has a high content of coumaric acid and caffeic acid which have antioxidant, anticancer and antidiabetic properties. This type of honey has antiproliferative activity on HCT-116 cells and cytostatic ayoctivity on MCF cell lines. 38
According to a systematic review conducted by Mansouri et al, curcumin, a polyphenol present in turmeric, has anticancerous properties proven by preclinical and clinical studies, it inhibits carcinogenesis, angiogenesis and tumor growth. It also increases the efficacy of chemotherapy and radiotherapy, which prolongs the survival time of cancer patients and increases the expression of anti-metastatic proteins. 39 According to Aggarwal et al, curcumin suppresses the proliferation of several tumor cells namely breast and colon carcinoma, renal cell carcinoma, hepatocellular carcinoma, T-cell leukemia, Bcell lymphoma, acute myeloid leukemia, basal cell carcinoma, melanoma and prostate carcinoma. 40
Su et al suggested that curcumin could be a cure for colon cancer. Their results showed that this pigment induced cytotoxicity and apoptosis of colorectal cancer colo 205 cells by the production of reactive oxygen species, Ca 2 + and activation of caspase-3. 41 Regarding thyme, a study on eleven species of Moroccan thyme showed that they contain carvacrol, thymol, borneol and p-cymene. According to this research, carvacrol and thymol have a cytotoxic effect against the P815 cell line, mainly carvacrol, which has this higher potency. 42
Another study showed that thyme extract causes necrotic cell death in the H460 human lung cancer cell line and reduces levels of IL-1 beta and IL-8. Due to its interference with the NF-kB p65 and NF-kB p52 pathways in cancer cells, data from this study proposed its use as an additional drug in decreasing the viability of cancer cells. 43 According to Al-Menhali et al, thyme induces proliferation and apoptosis of human colon carcinoma cells HCT116, inhibits their adhesion to fibronectin and inhibits their migration and invasion. 44
According to Lin et al, the Designer Food Program, NCI, 2005, considers garlic as a very powerful anticarcinogen that induces apoptosis and autophagy in cancer cells. These authors consider also garlic as a better alternative therapy for cancer. 45
A study conducted on garlic extract showed that this plant decreased the viability of two multiple myeloma cell lines RPMI-8226 and JJN3 and the prostate cancer cell line DU145, it also increased the efficacy of chemotherapy treatment such as docetaxel, gemcitabine, cisplatin and the combination of gemcitabine with cisplatin, as well as that of MAPK and PI3K inhibitors. In addition, it has weakened hundreds of proteins involved in cell signaling. 46
This results revealed that the most used part of the plants were seeds (27%) and leaves (24%). This has also been demonstrated by different previous studies,4,17,25,28,30,33-35,47,48 this frequency can be explained by the fact that leaves are important photosynthetic parts of plants that are rich in secondary metabolites with medicinal power 35 and because they are easy to harvest and more accessible than roots. 48
The adverse effects demonstrated by our study are low (5%), namely gastric burns, abdominal pain, gastritis and sweating. This rate is similar to that demonstrated by a study conducted in China 26 and low compared to other national studies.4–6
The results of our study show that medicinal plants are very important (37%) for patients undergoing chemotherapy. They seek above all in these remedies the cure of their disease (60%). Faced with this situation, many clinical studies are necessary to prove their effectiveness or not against cancer and their interaction with chemotherapy so that doctors can give alternatives based on concrete and scientific evidence and so that the patient himself can use safe and effective products concomitantly with its conventional treatment, and it also allows to develop a personalized consultation with the patients and their family to discuss the suitable complementary therapies and to give a plan of care based on convincing, personalized and safe evidence.
Limites
This study as a prevalence study, based on patients’ reporting of herbal use, may be subject to recall bias. Cancer patients may not disclose herbal use because they are afraid of their treating physicians which may result in an under-representation of the prevalence of MP. In addition, patients may not remember the type of herb, the amount used and the frequency, which will cause underuse, as well as for adverse events related to MP use.
Our study was conducted in a one hospital, this may influence the generalization of the results.
Conclusion
This study revealed a high prevalence of herbal use by cancer patients undergoing chemotherapy. Many of the plants used have anticancer activities proven by different studies. The more clinical studies are desirable to demonstrate the efficacy of medicinal plants and their therapeutic effects.
Different studies have been done in Morocco and have listed plants used in the oncological field. These plants must be studied scientifically and must present concrete proofs in order to have a solid basis to encourage or forbid the consumption or not of MP.
Footnotes
Acknowledgements
We would like to thank Ms. AZZOUZI Sanae and Aziza SELLAMI for their contribution to the data collection.
Contributions of the Authors
N.E. designed the study, participated in the collection, analysis and writing of the manuscript.
S.B, H.E and B.HR played a role in the revision of the manuscript and gave their final approval to the version that will be published.
Data Accessibility Statement
All data are included in the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval and Consent to Participate
An ethical approval for this survey was obtained by the Ethics Committee for Biomedical Research of the Faculty of Medicine and Pharmacy Mohamed V in Rabat under No. 27/18.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.