
Abstract
The prospective clinical, non-inferiority study aimed to investigate the effectiveness of Thai traditional massage on lower urinary tract symptoms (LUTS) compared with Tamsulosin in Thai men. It was conducted on men aged 50 to 75 years old with LUTS (N = 45). Participants were blocked four randomly assigned into 2 groups. The control group (n = 25) was received 0.4 mg Tamsulosin daily and the study group (n = 20) was given Thai traditional massage for 4 weeks. The efficacy evaluation was performed by the International Prostate Symptoms Score (IPSS), a Thai version of the World Health Organization Quality of Life Questionnaire (WHO-QoL Brief), Uroflowmetry, and Post-void residual urine (PVR) at baseline and end of study. The background characteristics of participants were not significantly different between groups. Both interventions relieved LUTS in the total IPSS and the quality of life score associated with urination were decreased, described as symptoms and quality of life due to urination improvement after 4 weeks of intervention. Interestingly, the Thai traditional massage has significant improvement in total IPSS and voiding score (p < .05). Additionally, the time to peak flow rate, peak flow rate (Qmax), average flow rate (Qave) and voided volume of both interventions were improved with no statistical significance. PVR was decreased in both interventions. The WHO-QoL brief score was improved the total score. There was no significant difference in terms of uroflowmetry, PVR, and WHO-QoL brief scores compared between groups. The result suggests that Thai traditional massage has the potential to be an alternative treatment for LUTS.
Introduction
Benign prostatic hyperplasia (BPH) is one of the most common urological diseases in men worldwide.1,2 It is distinguished by a benign overgrowth of prostatic tissue around the urethra, which eventually constricts the urethral opening, resulting in lower urinary tract symptoms (LUTS). In addition, the highest prevalence (80%) is present in men of age 71 to 80.3–5 BPH has also been linked to various medical complications, such as a lower quality of life and higher annual healthcare costs.6,7
According to the report of the outpatient department of surgery (urology) from 2015 to 2017, there were over 5000 male patients diagnosed with BPH, which was the most common urology condition. As a clinical practice guidelines of LUTS including BPH, the pharmacological treatment includes
Nevertheless, the study of massage therapy for BPH-associated LUTS is still limited. Hence, this study aims to investigate the efficacy of Thai traditional massage technique (Sen Sib massage) from the Wat Pho marble inscription compared to standard treatment using Tamsulosin in Thai men with BPH associated LUTS. 12
Methodology
Study Design
A prospective non-inferiority randomized clinical trial study has been approved by the Human Research Ethical Committee and registered the Thai Clinical Trials Registry. The study was carried out from December 2018 to December 2020.
Participants
The sample size was calculated by the G*Power program with
Inclusion criteria
Male patients suffering from LUTS for at least 6 months Age 50 to 75 years old Reveal the moderate level of symptoms (IPSS score between 8-19) Urinary peak flow rate (Qmax) is between 5 to 15 ml/s evaluated by uroflowmetry with Post-voided volume of ≥150 ml determined by bladder scan Prostate-Specific Antigen (PSA) level is ≤ 4 ng/ml Blood urine nitrogen (BUN) level is 10 to 20 mg/dL Creatinine level is 0.7 to 1.3 mg/dL Glomerular filtration rate is > 60 ml/min. Urethral stricture and/or bladder neck disease active or recent < 3 months Recurrent urinary tract infection Urinary retention Indication of BPH surgery or prostate surgery Bladder/urethra stone Acute or chronic prostatitis Prostate or bladder cancer, Interstitial cystitis, Active upper tract stone disease-causing symptoms Indication of bladder neck and pelvic region surgery Local or systemic inflammation disorder Orthostatic hypotension (standing SBP reduced > 20 mm Hg or DBP reduced > 10 mm Hg compared to supine position) History of neurologic or psychiatric disorder/disease interfering with the detrusor or sphincter muscle Insulin-dependent diabetes mellitus and non-controlled non-insulin-dependent diabetes mellitus History of chronic renal insufficiency History of severe hepatic failure or other severe underlying diseases
Exclusion criteria
Every new case of the Urology department with LUTS would be screened by urologist following the above criteria. If they meet the criteria, they will be invited to participate in the study.
Study Intervention
After the informed consent signing was obtained, 58 eligible participants were randomly allocated to two groups using block four randomization technique: 1) Control groups (n = 29); and 2) Study group (n = 29). The control group was prescribed 0.4 mg Tamsulosin orally before bedtime every day while the study group received 30 min of Thai traditional massage twice a week for four weeks. (Figure 4)
Due to the nature of the intervention, participants and the research team delivering the intervention will not be blinded to the treatment received. Outcome measures are primarily self-reported and submitted anonymously. Those involved in the data analyses and statistics will be blinded to the group allocation.
The control group: tamsulosin treatment
The participants took 0.4 mg Tamsulosin orally before bedtime for 4 weeks.
The study group: Thai traditional massage treatment
During the study, the massage was done by a licensed Applied Thai traditional practitioner (ATTM) in a private place. Each study participant was placed in a supine position, then was coached to relax for 5 min in this position before the treatment. An abdominal massage was performed on each participant for 30 min. The massage method is followed as:
Step 1: Abdominal massage started from using the base of both palms pressing on the line begun at Anterior superior iliac spines (ASIS) to costal margin at 10th rib level of each side, right and left respectively (Figure 1) for 5 min.

the location of Thai traditional massage, the line of edge of abdomen
Step 2: The points pressed on the abdomen consisted of 3 pairs of points. The first pair of points are below the umbilicus (close to the lower edge of the navel) at medial edge of rectus abdominis muscle (Figure 2). Technique: With practitioner's thumbs, placed on both points, thumb tips pointed close together, vertically pressed both points for 45 s and rested for 15 s in a cycle, then released pressure on points and repeated the pressing and releasing cycle for total of 5 min.

three pairs points of massage
The second pair of points, are below the first pair, 2 fingerbreadths below the navel, and 2 fingerbreadths lateral to the linea alba (Figure 2). Technique: Same as for first pair of points.
The third pair of points are below the second pair of points on the edge of the abdominal oblique muscle, near the inguinal groove at the edge of the abdominal oblique muscle (Figure 2). Technique: Same as for the first and second pair of points, using both upside thumbs on each point, right and left respectively.
Step 3: Technique: Pressed vertically along the linea alba line below the umbilicus, using both tips of thumbs using same 45 s pressing then releasing cycle as in Step 2 for total of 5 min (Figure 3).

the middle line of abdominal massage
Analytical Tools
The international prostate symptoms score (IPSS)
The IPSS questionnaire is used to evaluate the symptoms’ severity. IPSS is an 8-item questionnaire that appears to be a subjective measurement that includes 7 symptoms questions and a quality of life due to urination question (UQoL). It can be divided into three subgroups as storage symptoms (item 2, 4 and 7), voiding symptoms (item 1, 3, 5 and 6) and UQoL (item 8). The questionnaire was scored from 0 to 5, and the summation score was calculated to be between 0 and 35. A score of less than 7 indicates mild symptoms, a score of 8 to 19 indicates moderate symptoms, and a score of more than 20 indicates severe symptoms. The UQoL is defined as the lower score resulting in high quality of life due to urination (0 = well and 5 = very bad). 14 The score of each participant was summarized from symptoms daily recording that was given on recruitment day.
Thai version of world health organization quality of life questionnaire (WHO-QoL)
The WHOQOL brief Thai version includes 26 items of question assessing 1 to 5 ranges of scoring. The physical results were described as good, fair, and poor, with good = 27 to 35, fair = 17 to 26, and poor = 7 to 16. The psychological domain is described as good = 23 to 30, fair = 15 to 22 and poor = 6 to 14, while the social relationship domain is described as good = 12 to 15, fair = 8 to 11 and poor = 3 to 7. The environmental domain is described as good = 30 to 40, fair = 17 to 29 and poor = 8 to 18 as well as the total score is described as good = 96 to 130, fair = 61 to 95 and poor = 20 to 60. 15
Uroflowmetry
Uroflowmetry is used to measure the flow rate and pattern of the flow of urination. The uroflowmetry parameters are classified into 3 parts of analysis as time of urination, rate of urination and volume of urination. The time of urination is included as voiding time, flow time and time to peak flow rate, after treatment should be decreased. The rate of urination consists of peak flow rate (Qmax) and average flow rate (Qave), after treatment should be increased as well as the voided volume is also increased after treatment. Normally, the peak flow rate, or Qmax, is set to 15 ml/s. Furthermore, when the voided volume exceeds 150 mL and the PVR exceeds 100 mL, uroflowmetry parameters should be evaluated..8,16
Post-void residual urine (PVR)
The post-voided residual urine was measured by suprapubic ultrasound or bladder scanner. The total urine remaining after urination should be less than 100 mL. 8
Statistical Analysis
The results were analyzed by SPSS 16.0 for Windows. The findings were reported via descriptive, frequency, percentage, mean and standard deviation. The statistical analysis was performed by using a Chi-square test to compare the background characteristics, duration of LUTS, subgroup of symptoms (storage and voiding), and comorbidity. ANOVA was applied to compare age, total IPSS score (storage and voiding), quality of life related to urinary symptoms (UQoL), uroflowmetry parameters, post-voided residual urine, PSA, BUN, Cr and GFR, baseline and end of study of the interventions. P-value < .05 significant level was used for all testing. Participants and the research team delivering the intervention cannot be blinded to the treatment received due to the nature of the intervention. Outcome measures are primarily self-reported and submitted anonymously. Those who were involved in the data analysis and statistics will be blinded to the group allocation.
Results
There were 58 study participants at the beginning of the trial. 45 participants completed the interventions. They were randomly assigned into 2 groups by block randomization in Figure 4. Table 1 shows that baseline characteristics of participants, such as age and laboratory investigations (PSA, BUN, Cr, and GFR), were similar.

Study flowchart
Baseline Characteristics of Participants.

Data was analyzed by ANOVA test.
Values are expressed in mean ± standard deviation.
Abbreviations: N = Number of patients in each group.
PSA = Prostate Specific Antigen.
BUN = Blood Urea Nitrogen.
Cr = Creatinine.
GFR = Glomerular Filtration Rate.
* = P-value <.05 is considered a statistically significant difference.
Participants had LUTS from 6 to 36 months, mostly in 6 months. In both interventions, subgroups LUTS analysis revealed that nocturia was the most common storage symptom. The voiding symptom was shown the most frequent in slow stream of urination in both interventions, while the control group was also most frequent in incomplete emptying and intermittency in the study group. The majority of the control group was reported to have no comorbid conditions. Hypertension, on the other hand, was found to be a comorbidity in half of the study participants. Subgroup lower urinary tract (LUT) symptoms and comorbidity of all participants at baseline evaluation are shown in Table 2. When focusing on the baseline evaluation on age, laboratory investigation, duration of LUTS, frequency of subgroup LUTS and comorbidity were similar in both interventions.
Duration of LUTS, Frequency of Subgroup LUT Symptoms and Comorbidity of Baseline Evaluation.

Data was analyzed by Chi2 test, LUT = Lower Urinary Tract Symptoms.
* = P-value <0.05 is considered a statistically significant difference.
The efficacy indicators were included as IPSS, Uroflowmetry parameters, PVR, and WHO-QoL assessed at baseline and the end of study evaluations.
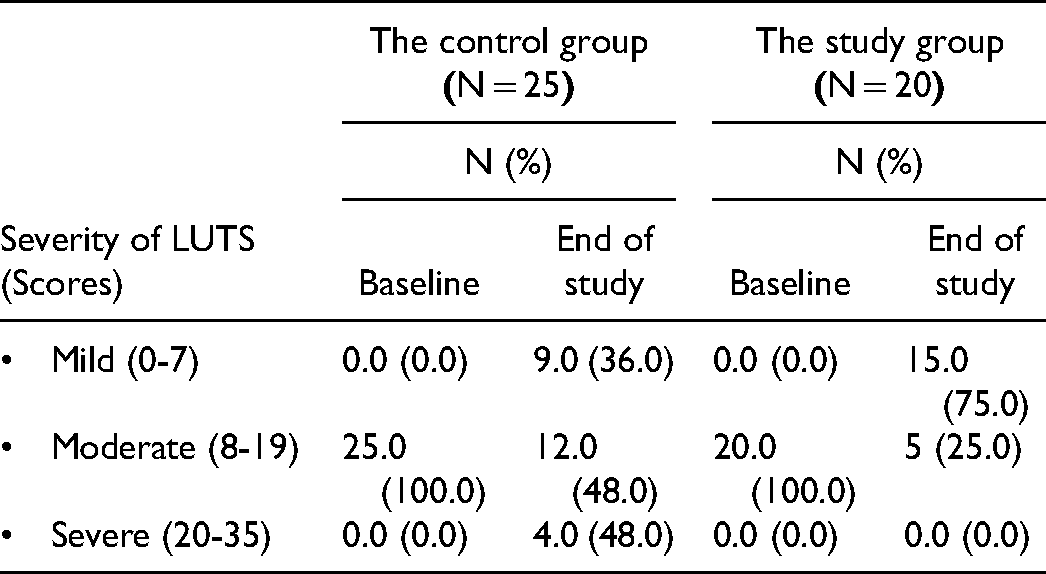
The IPSS evaluation suggests that both interventions can reduce the severity of LUTS. The IPSS questionnaire consists of 4 parts, namely total IPSS score (IPSS-T), storage score (IPSS-S), voiding score (IPSS-V), and quality of life due to urination (UQoL). There was decreased in all parts of the IPSS score for all subjects. Due to the IPSS questionnaire is a subjective measurement, when compared between the 2 groups, the mean IPSS-T and IPSS-V score after the massage was lower than the control group with a statistically meaningful difference (P < .05). According to the IPSS-T, the severity of LUTS of participants who received a massage appears to reduce from moderate to mild level (table 3). The IPSS of each group was demonstrated in table 4.
the Severity of LUTS from Baseline to end of Treatments.
Changes from Baseline to end of Treatments in IPSS, Uroflowmetry Parameters, PVR, and WHO-QoL.

Data was analyzed by ANOVA test.
Values are expressed in mean ± standard deviation.
Abbreviations: N = Number of patients in each group.
IPSS = International Prostate Symptom Score.
PVR = Post-voided residual urine volume.
WHO-QoL = World Health Organization Quality of Life.
* = P-value <.05 is considered a statistically significant difference.
The mean of uroflowmetry parameters, there was no significant difference between the two treatments. In the study group, voiding time was a statistical reduction after treatment (P < .05). Flowtime and time to peak flow rate were slightly reduced after the massage session. Additionally, the peak flow rate (Qmax), average flow rate (Qave) and voided volume were negligible reductions after the massage session. In addition, Qave of the study had a significantly high positive correlation (cor > 0.767). Flow time, time to peak flow rate, and voided volume of the study had a statistically significant low positive correlation at the start and end of the study. However, all the changes did not reach statistical significance when compared between the 2 groups. (Table 4)
PVR (Table 4) exhibited a reduction of urine retention in both groups. When compared PVR between the 2 groups, there was no significant difference.
When focusing on the quality of life of the participants, the mean WHO-QoL total score was increased in both groups with an increase from baseline in the control and the study groups, respectively. The total score, which represents overall quality of life, showed that both interventions remained at a fair level when compared to the baseline and end of the study. The physical score (D1) decreased in the control group and increased in the study group. For psychological score (D2), there was an improvement in both groups. The score of social relationship (D3) was increased in the study group, but decreased in the study group. It meant that the social relationship improved only in the control group. For environment (D4), the mean score was increased in the control group and decreased in the study group. Nonetheless, no statistically significant difference between the two groups was found in all domains. Physical, psychological, social relationship and environmental domains of the control group remained at a good level. On the contrary, the study group had a fair level of acceptance in the psychological domain. The changes in WHO-QoL score from baseline to the end of the study were shown in Table 4.
Discussion
The results suggested the improvement of LUTS severity after massage session shown the LUTS severity detected by IPSS, peak flow rate (Qmax) and PVR improvement. It may have the same effect as the 0.4 mg Tamsulosin oral daily, a super selective
Conclusion
Finally, Thai traditional massage appears to be as effective as Tamsulosin in treating LUTS. Thai traditional massage reduces symptom severity from moderate to mild. As a result, Thai traditional massage could be considered as a therapeutic option for LUTS.
Footnotes
Author Contributions
Study conception and design: Sinsomboon, Noppakulsatit, Tassanarong, Tungsukruthai and Sriyakul
Acquisition of data: Sinsomboon, Noppakulsatit and Sriyakul
Analysis and interpretation of data: Sinsomboon, Noppakulsatit, Tassanarong, Tungsukruthai and Sriyakul
Drafting of manuscript: Sinsomboon, and Sriyakul
Critical revision: Sinsomboon, and Sriyakul
Acknowledgments
The method of Thai traditional massage is passed on knowledge from Sirimongkol Tobngam, Thai traditional medicine expertise. The out-patient department of surgery, Thammasat University Hospital supported to recruitment of participants to the study. Chulabhorn International College of Medicine, Thammasat University provided the equipment and room for the massage sessions.
Ethical Approval
This study had been approved by the Human Research Ethical Committee No.1 of faculty of medicine, Thammasat University before data collection (MTU-EC-OO-4-068/61) and registered the Thai Clinical Trials Registry (No. TCTR20190204001.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Thai traditional medical knowledge fund, Department of Thai traditional and alternative medicine, Ministry of public health, Thailand. (grant number TKF.6/2019).