
Abstract
Background.
A growing trend in surgical care is the investigation and incorporation of multimodal interventions into standardized programs. Additionally, manual therapies such as osteopathic manipulative treatment (OMT) are being used with patients in surgical care. Yet the scientific dialogue and the use of OMT in surgical care are currently insubstantial.
Objective.
The aim of this study was to present an overview of published research articles within the subject field of OMT in surgical care.
Method.
Summative review of peer-reviewed research articles published in osteopathic journals during the period 1990 to 2017. In total, 10 articles were identified.
Result.
Previous research has been conducted within the areas of abdominal, thoracic, gynecological, and/or orthopedic surgery with measured outcomes such as pain, analgesia consumption, length of hospital stay, and range of motion. Heterogeneity was identified in usage of osteopathic techniques, treatment duration, and occurrence, as well as in the treating osteopath’s experience.
Conclusion.
Despite the small number of research articles within this field, both positive measured effects as well as the absence of such effects were identified. Overall, there was a heterogeneity concerning surgical contexts, diagnoses, signs and symptoms, as well as surgical phases in current interprofessional osteopathic publications. In this era of multimodal surgical care, we argue that there is an urgent need to evaluate OMT in this context of care and with a proper research approach.
Current estimates suggest that approximately 234 million surgical operations are performed worldwide each year. 1 A growing trend in surgical care is the use of multimodal, evidence-based interventions as structured programs. These programs aim for optimal recovery and minimal impact from signs and symptoms resulting from the surgical intervention. Programs such as enhanced recovery after surgery (ERAS) 2 and fast-track surgery 3 have successfully been initiated since the 1990s 4,5 and may include interventions that have previously been sporadically used or considered unconventional, such as acupuncture and music therapy. 6 It is known that patients themselves use complementary therapies to improve health prior to or during surgical care. 7 Besides herbal and natural products, manual therapies are among the most common patient-initiated therapies in surgical care. 7
As part of integrative or complementary medicine, manual or manipulative therapies are grouped under mind and body practices, which are methods that encompass a broad range of therapeutic interventions. 8 Regulated professionals such as osteopaths, chiropractors, and physical therapists commonly employ manual therapy methods in order to assess and treat neuromusculoskeletal dysfunction and pain syndromes. However, unregulated practitioners may also provide some manual therapies, for example, massage and Bowen therapy. Manual therapies may be defined and subdivided into various categories, with a general aim of affecting either biomechanical or neurophysiological change. 9 –15 Additionally, different manual therapy professionals may utilize similar methods but with a distinct professional-specific intent, as in chiropractic and osteopathic care.
Osteopathy is a patient-centered, whole-person health care discipline that first appeared in the late 19th century and has since evolved differently in different parts of the world. 16,17 Two major branches may be defined: the European tradition and the American form of osteopathy. American osteopathic physicians are licensed medical physicians, with additional training in osteopathic manipulative treatment (OMT) and osteopathic philosophy. European osteopaths are trained in the tradition of osteopathy as autonomous, nonphysician, primary health care practitioners with a specific expertise in the diagnosis and treatment of pain syndromes and somatic dysfunction rather than disease.
With regard to the distinctive philosophical perspective on health and application of manual techniques that are proposed within the realm of osteopathic practice, it is important to investigate the intraprofessional scientific publication dialogue with focus on surgery during this period of major changes in surgical care. This is important because, despite the growing body of research on OMT, and the increasing interest in expanding surgical care interventions into historically unconventional areas, no summary of published research on OMT in surgical care has previously been presented. Hence, the aim of this study was to present an overview of research publications in osteopathic journals within the subject area of OMT in surgical care.
Method
This summative review encompassed research articles within the realm of OMT research communication during the past 28 years and was not restricted to methodology, form of OMT or the context, and phase or form of surgical care.
Sample
The inclusion criteria for journals were that they should be scientific, peer-reviewed osteopathic medical journals, published in English, and active during the years 1990 to 2017. Exclusion criteria were journals with a broader aim of covering manual therapies not included within OMT, osteopathic journals covering the aims and scope of the osteopathic physicians’ practice, and osteopathic journals that limit their scope to allopathic medical perspectives.
Inclusion criteria for articles within the included journals were that they should cover studies published between January 1, 1990, and November 31, 2017, presented in English, and containing a research aim and results that investigated any form of OMT in any kind of surgical care. Surgical care was defined as care given by all health care professionals, during the total period of care, to patients seeking help for a surgically treatable disease or injury, or who had signs and symptoms of such. 7 Exclusion criteria were articles on primary care that included lesser surgical incisions (such as naevus removal or shallow wound suturing) and articles awaiting publication or in press.
Data Collection
Initially, international osteopathic research journals were identified through medical university library resources, osteopathic medicine library archives, professional osteopathic associations, and organized osteopathic research collaborations. A total of 32 journals were identified. After applying the inclusion and exclusion criteria, a total of 9 journals were included in the article search.
All issues of the included journals covering the appropriate time period were investigated in the search for articles matching the study’s inclusion criteria. First, all article titles were read, resulting in the extraction of 22 articles. Next, abstracts from the extracted articles were read, resulting in 10 articles that were read in full. This resulted in 10 articles that were included in the analysis. The article collection process is presented in Table 1.
Article Collection Process.

Analysis
The identified articles were analyzed using a fixed framework including the following aspects: article demographics (country of investigation, type of surgery, number of participants), research methods, measurement parameters, treatment properties, and OMT techniques applied.
Data were compiled in Microsoft Excel 2013 and presented in absolute and relative frequencies, mean and range (min–max), and in tables.
Ethics
Ethical considerations in the included articles were also investigated. The reviewed studies had all received either institutional review board approval 18–26 or regional ethics review board approval. 27 Out of the 10 studies, 7 stated that informed consent had been obtained from the participating subjects. 21–27 The 3 remaining studies were all retrospective ones based on patient charts. 18–20
Results
In total, 10 research articles were identified from the total of 1447 that were reviewed (0.7%); see Table 1. Summative demographics of the included studies are presented in Table 2. Concerning geography, 7 of the studies were performed in the United States, 2 in Europe, and 1 in Asia. The included articles were conducted within 4 different surgical areas, including both soft tissue as well as orthopedic specialties. Concerning methodology, 5 studies were randomized controlled trials, 3 were retrospective chart reviews, 1 had a single-subject design, and 1 was a prospective clinical pilot study. Measurements presented and calculated in the studies, as well as a descriptive presentation of the OMT included, have been thematically structured and are presented in Tables 2 and 4.
Article Demographics (n = 10).

Measured Parameters
Postoperative measurements of pain and analgesia consumption were used to evaluate OMT in 5 studies. 21–23,25,27 Two studies measured postoperative pain using the Visual Analogue Scale (VAS), 22 a Pain-o-Meter, and the Brief Pain Inventory–Short Form. 27 Probst et al 25 used a numerical rating scale (NRS) to record pain intensity levels in a randomized controlled pilot trial and reported a decrease in pain following abdominal surgery in the OMT group (n = 10) compared to the control group (n = 10) during the first 5 postoperative days (a decrease of 2 units of the NRS [P < .01] for the OMT group). Kim et al 22 conducted a prospective, randomized controlled pilot study where OMT treatment was compared with an exercise intervention program in the rehabilitation phase after lumbar disc surgery. Change in VAS prior to and after the intervention was nonsignificant for leg pain (P = .81) and lower back pain (P = .29) when comparing the OMT group (n = 16) and the exercise group (n = 17). It is worth noticing that the OMT group had lower levels of pain prior to the intervention compared to the exercise group. In a single-subject study (n = 8), Bjerså et al 27 investigated OMT treatment for chronic postoperative pain, thoracic stiffness, and impaired breathing following thoraco-abdominal esophagus resection. The results indicated that chronic postoperative pain might be decreased by OMT.
In 3 studies, pharmacological analgesic consumption was evaluated. 21–23 Goldstein et al 21 conducted a study with 4 groups (1, Preoperative saline and Postoperative sham-OMT [n = 9]; 2, Preoperative saline and Postoperative OMT [n = 10]; 3, Preoperative morphine and Postoperative sham-OMT [n = 10]; 4, Preoperative morphine and Postoperative OMT [n = 10]) among patients scheduled for abdominal hysterectomy, and the authors found that group 4 consumed significantly (P = .011) less postoperative morphine compared to group 3, but this level was nonsignificant compared to groups 1 and 2. Kim et al 22 reported a decrease in weekly analgesia consumption in both the OMT group and the exercise group, with a larger decrease in the OMT group, though it was statistically nonsignificant (P = .28). Licciardone et al 23 reported no significant difference in analgesia consumption (mg/day) in the form of acetaminophen (P = .68) and hydrocodone (P = .71) between patients receiving OMT (n = 30) compared to sham-OMT (n = 30) in the context of rehabilitation after knee or hip arthroplasty. 23 Additionally, Bjerså et al 27 only registered analgesics before and after the OMT phase and showed a decrease in paracetamol usage in 1 participant.
Functionality was included as a distinct measure in the results of a minority of the included studies. 22,23,26 However, all the 10 articles analyzed included some form of results indicating functional independence, such as length of hospital stay (LOS) and/or joint mobility, improved peripheral circulation, and increased mixed venous oxygen saturation.
Postoperative LOS was measured in a majority of the included studies. 18–20,23,25,26 The results from 2 articles suggest shorter LOS due to complementary surgical care with OMT. 18,19 Baltazar et al 18 found that general surgical patients given OMT (n = 17) had a significantly (P = .006) shorter LOS compared to general surgical patients not receiving OMT (n = 38), of approximately 5 days in mean. In a retrospective chart review, Crow and Gorodinsky 19 also found significantly (P = .029) shorter LOS among general surgical patients given OMT (n = 172) compared to patients who had not received OMT (n = 139), by approximately 2.5 days in mean. In contrast, 3 articles reported nonsignificant findings concerning LOS. 20,25,26 Following thoracotomy, Fleming et al 20 found no statistical differences (P > .09) in LOS between patients receiving OMT (n = 23) and patients not receiving OMT (n = 15). After abdominal surgery, Probst et al 25 found no significant (P = .29) difference in LOS between the OMT group (n = 10) and the control group (n = 10). Nor did Wieting et al 26 in patients after cardiac artery bypass graft (P = .72), among patients receiving OMT (n = 17), placebo (n = 18), and a control group (n = 18). Additionally, Licciardone et al 23 found that patients given OMT (n = 19) compared to sham-OMT (n = 11) when rehabilitating after knee arthroplasty had a significantly (P = .004) longer LOS of just above 7 days in mean.
Range of motion as a mobility measurement was reported in 2 articles. 22,27 In rehabilitation after lumbar disc surgery, Kim et al 22 found no significant change prior to and after intervention between the OMT group (n = 16) and the exercise group (n = 17) in flexion (P = .51), extension (P = .24), and right (P = .76) and left (P = .25) side bending. After thoracotomy, Bjerså et al 27 found, in a single-subject study, significant (using the ±2SD maneuver) improvement in left (n = 3) and right (n = 6) lateral flexion during and after the OMT treatment phase compared to the prior treatment phase.
Postoperative bowel function as a measure of OMT effects was presented in 4 studies. 18,20,25,26 Among general surgical patients, Baltazar et al 18 found a significantly (P = .035) shorter time to first postoperative flatus in the OMT provided group (n = 17) compared to the non-OMT provided group (n = 38) by approximately 1.5 days in mean, and no statistical differences between the groups in time for first postoperative bowel movement (P = .43) or start of postoperative clear liquid diet (P = .59). Post-thoracotomy, Fleming et al 20 found no difference in postoperative ileus incidence between the OMT group (n = 23) and the non-OMT group (n = 15). Also, Probst et al 25 found no statistical differences in the first postoperative bowel movement (P = .42), first postoperative flatus (P = .26), or postoperative solid food intake (P = .54) after major abdominal surgery between the OMT group (n = 10) and control group (n = 10). Also in cardiac surgery, Wieting et al 26 found no significant difference in time for postoperative bowel movement (P = .19) among the OMT group (n = 17), placebo group (n = 18), and the control group (n = 18). However, both Probst et al 25 and Wieting et al 26 indicated beneficial nonstatistical trends of bowel function in their OMT groups, and none of the included articles reported adverse or negative findings regarding bowel moment after OMT treatment.
Hemodynamic and cardiac measurements were included in the results of one article. 24 O-Yurvati et al 24 found statistical improvements in the OMT provided group (n = 10) compared to the control group (n = 19) in change of venous saturation (SvO2; %) after coronary artery bypass grafting surgery. Furthermore, analysis within the OMT group (n = 10) prior to and after given OMT treatment also revealed statistical benefits in thoracic impedance (P = .02), SvO2 (P = .005), as well as in the cardiac index (P = .01).
In addition to these themes, global measures such as care satisfaction and satisfaction with OMT were presented in 2 studies. 22,27 The patients in these studies generally gave high ratings for satisfaction and were positive about the OMT following orthopedic and thoracic surgery.
Treatment Properties and Applied Osteopathic Techniques
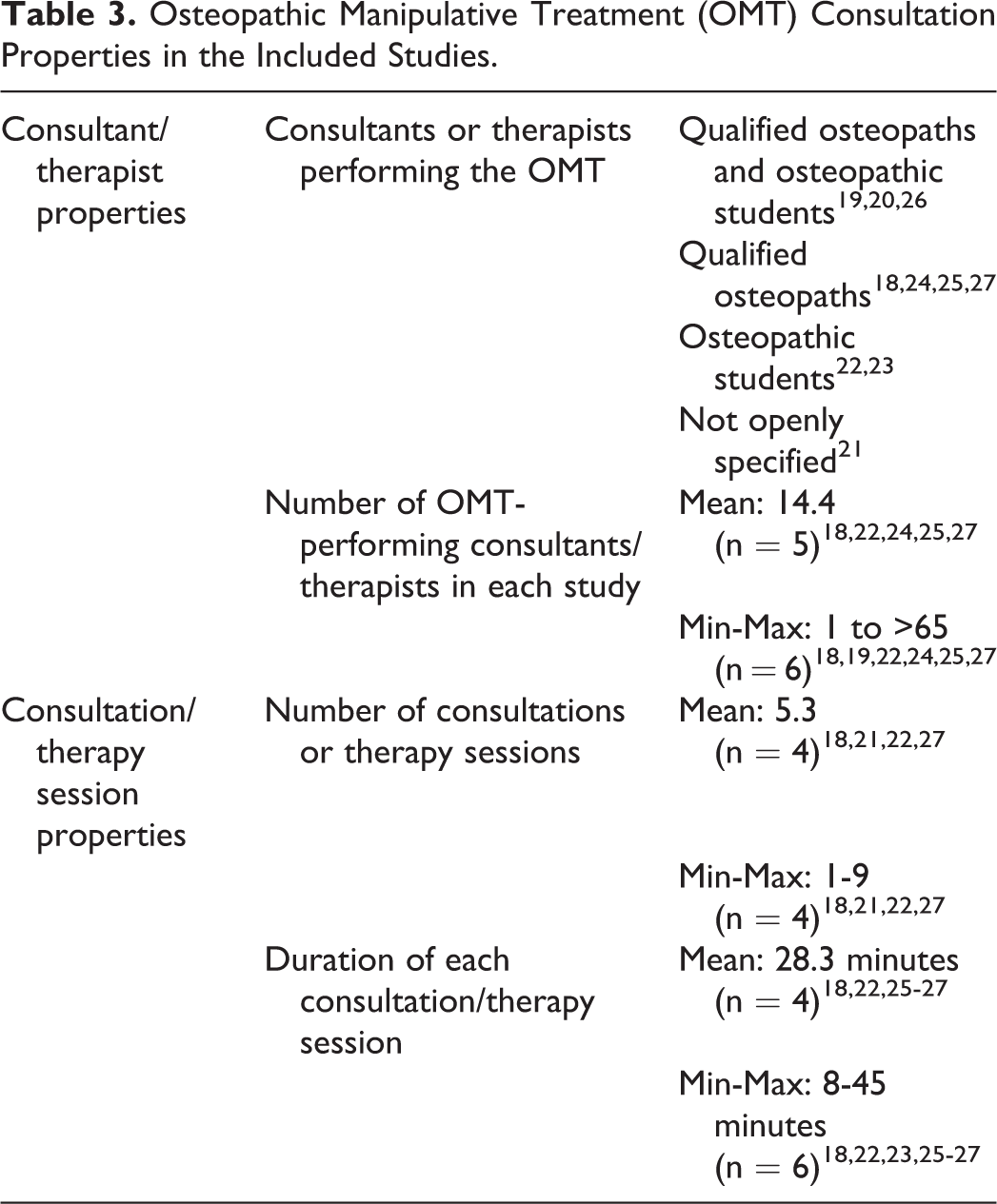
Information concerning the therapeutic nature of the OMT sessions in each of the studies included was disparate in detail. Data on OMT providers’ qualifications, number of treatments, and treatment time varied considerably, and in some studies was inconclusive; see Table 3. Furthermore, the rationale for the therapeutic methods included was generally vague 21–25 or absent. 18–20,27 As an exception, Wieting et al 26 chose the techniques they employed in all treated areas on the basis of the techniques’ supposed neurophysiological, circulatory, and biomechanical effects.
Osteopathic Manipulative Treatment (OMT) Consultation Properties in the Included Studies.
Descriptions of the forms of OMT applied within each study varied in specificity and structure. A summary of treatment and OMT techniques included is presented in Table 4. Please note that the terminology used to categorize OMT techniques may vary slightly from the nomenclature stated in each article. However, the content and meaning remain the same. Various forms of soft tissue techniques and so-called indirect techniques were used frequently throughout the reviewed studies, although a general feature concerning the treatment protocols was the combination of different forms of OMT. Notably, high-velocity, low-amplitude manipulation was only specifically included in 2 studies, 20,23 one of which concerned only one patient. 20
Osteopathic Manipulative Treatment (OMT) Techniques Used in the Included Studies (n = 10).

Discussion
In order to achieve the aims of this study, 10 studies published during the past 28 years were identified within osteopathic journals. This sparse number raises questions regarding why this area has not been explored in more depth, and whether there are any particular reasons that the intraprofessional dialogue that is normally required in this area of research is hindered. Irrespective of reasons, the current development and use of multimodal programs such as ERAS 2 and fast-track surgery 3 should present an interesting opportunity to prioritize future research on OMT in surgical care for the osteopathic research community.
Some of the most common postoperative symptoms in surgical care include pain, 28 –30 decreased bowel function and postoperative ileus, 31 –33 nausea and vomiting, 34 –36 malnutrition, 37 –39 fatigue, 40,41 anxiety and depression, 42 –46 confusion and delirium, 47 –50 and sleep disturbance. 51 –53 A feasible approach toward evaluating OMT in surgical care could be to structurally prioritize research parameters based on current knowledge of the prevalence of specific symptoms, complications, LOS, related socioeconomic factors, and person-centeredness, as documented in the literature. Such structural assumptions were not found in the articles included in this summative review. As suggested above, and based on the fundamental principle of osteopathy as a whole-person health care discipline, measuring the patient’s perception of OMT should be a standard research protocol in all osteopathic studies. However, this was not the case in the included studies, as none of them included validated instruments for measuring person-centered care.
All of the studies included focused on the postoperative phase. However, preparing patients for surgery in a manner that optimizes both the perioperative as well as the postoperative phases has become a goal in surgical care. 2,4 Preoperative care encompasses physical, psychological, and nutritional aspects, for example, exercise, 54 –56 smoking cessation, 57,58 oral nutrition, 59 –62 and/or education. 63 –65 A legitimate suggestion would be to explore OMT as part of such a prehabilitation protocol, yet none of the included studies investigated the effects of preoperative OMT.
OMT applied in the included studies showed considerable variation and limited motivation for use, both in isolation and in combination, as presented in the respective treatment protocols. Furthermore, the results showed vast discrepancies between the various studies regarding the consultants’ clinical experience, number of treatment sessions provided, treatment time, and therapeutic interventions. While the importance of these factors has not yet been sufficiently researched within the domain of OMT, they may still have an impact on the therapeutic outcome. Consequently, even though there were indications of both positive effects as well as absence of effects of OMT, no general conclusions could be drawn regarding the efficacy of OMT in surgical care.
Finally, based on these results and the issues discussed above, the authors argue that future research within this field should be based on hypotheses that stem from both biomechanical and neurophysiological knowledge, with valid motivations for treatment and measurement properties in order to minimize the risk of excessively widespread research.
Limitations
The possibility of analyzing any relevant data in the study was restricted by the limited amount of scientific material published on the subject of OMT in surgical care in osteopathic medicine journals, as well as by the lack of research foci across the reviewed articles. This lack of research made impossible any attempt to systematically review as part of unique intraprofessional osteopathic research. Therefore, the authors suggest that, as the next step to investigate manual therapies in surgical care, a future systematic review should include a broader spectrum of manual therapies based on a data-based methodology. However, this intraprofessional summary is still needed as a first step in order to clarify the unique focus of the osteopathic profession. There is also a need to perform this type of summative review on other manual therapy professions in order to reveal intraprofessional applications and trends that could affect research within this area.
Conclusion
Although the number of osteopathic research articles published in the area of surgical care since 1990 is small, they contain indications of both positive effects and absence of effects of OMT in areas such as postoperative pain, analgesia consumption, LOS, and postoperative bowel function. Although several areas within the surgical spectrum have been investigated, specification and argumentation for the use of certain osteopathic techniques varies, as does the knowledge and experience of the performers of these techniques. Overall, there is a heterogeneity concerning surgical contexts, diagnoses, signs and symptoms, as well as the surgical phases of current intraprofessional osteopathic publications. In this era of multimodal surgical care, such as ERAS and fast-track protocols, we argue that there is an urgent need to evaluate OMT in this context of care and with a proper research approach.
Footnotes
Author Contributions
NS and KB conceived the idea for the study. Both authors contributed to the design and concept. NS managed the data collection. Both authors analyzed and interpreted the data, constructed and revised the manuscript for logical content, and approved the final version.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.