
Abstract
The purpose of the present study was to conduct a systematic review of the literature, adhering to PRISMA guidelines, regarding evidence of neuroplasticity in children and adolescents in response to cognitive or sensory-motor interventions. Twenty-eight studies employing seven different types of neuroimaging techniques were included in the review. Findings revealed that significant variability existed across the 28 studies with regard to the clinical populations examined, type of interventions employed, neuroimaging methods, and the type of neuroimaging data included in the studies. Overall, results supported that experience-dependent interventions were associated with neuroplastic changes among children and adolescents in both neurotypical and clinical populations. However, it remains unclear whether these molecular neuroplastic changes, including the degree and direction of those differences, were the direct result of the intervention. Although the findings are encouraging, methodological limitations of the studies limit clinical utility of the results. Future studies are warranted that rigorously define the construct of neuroplasticity, establish consistent protocols across measurement techniques, and have adequate statistical power. Lastly, studies are needed to identify the functional and structural neuroplastic mechanisms that correspond with changes in cognition and behavior in child and adolescent samples.
Introduction
Broadly speaking, neuroplasticity refers to the ability of the brain to undergo morphological and neurochemical changes as a result of experience. A variety of definitions on neuroplasticity exist, each emphasizing different elements. For example, Cramer et al. defined neuroplasticity as “the ability of the nervous system to respond to intrinsic or extrinsic stimuli by reorganizing its structure, function and connections” (p. 1591), while Sarrasin and colleagues’ more recent definition focuses on “the capacity of the brain to modify its neural connections through learning” (p. 23). 1,2 An abundance of human and other animal research supports the ability of the brain to change in response to environmental stimuli and this change can be adaptive (improvement in function) or maladaptive (loss of function). 3 –8 These underlying cellular, morphological, structural, and functional changes are believed to be the result of a complex interplay between genetic, biological, psychological, and environmental factors. 9,10
Developmentally, human brain growth is mediated by genetic and environmental factors from the moment of conception; however, historically it was believed that the brain underwent little change beyond childhood. Indeed, it was not until the late 1970s that research substantiated that the prefrontal cortex undergoes structural changes during adolescence. 11 Technological advances in brain imaging have enabled researchers to demonstrate aspects of brain development that continue throughout childhood and adolescence; however, the ways in which these changes unfold as well as their effects on behavior and cognition are less clear. 12 –18 Since the establishment of the Decade of the Brain in the 1990s, there has been a fivefold increase in neuroplasticity-related research, and similarly, an increased interest in the topic by the media and popular press. 19,20
Understanding the mechanisms underlying neuroplasticity is important from a basic and an applied perspective. For example, ongoing research in the field of neuroplasticity indicates that negative environmental triggers (e.g. inadequate care, poverty, neglect, and stress) can result in increased vulnerability to psychological disorders or an impaired stress response later in life, presumably in part due to morphological and functional brain changes. 21,22 On the other hand, the brain’s ability to adapt both structurally and functionally makes childhood the preferred period for many surgical interventions (such as hemispherectomies or cochlear implants) that are less effective if delayed until adulthood. 23 Understanding neuroplasticity during childhood and adolescence and investigating methods to foster this process across the life span could help to counteract negative outcomes associated with environmental factors and possibly neurodegeneration later in life.
In response to the body of research that supports that the brain undergoes substantial growth and development during childhood and adolescence, and the increased interest in neuroplasticity in the scientific literature and popular press, the purpose of the present study was to conduct a systematic review of the literature addressing neuroplasticity among children and adolescents using neuroimaging techniques. A second purpose of the article was to critically evaluate the methodological strengths and weaknesses of these studies in order to provide direction to future research. Specifically, the present systematic review sought to address whether neuroplasticity occurs among children and adolescents with and without clinical disorders in response to experience-dependent intervention based on neuroimaging findings. The research questions were as follows: (1) What are the key measures and analytical techniques used within this neuroplasticity literature?; (2) What are the associated methodological strengths and limitations from this area of research?; (3) Does current neuroimaging research support the presence of neuroplasticity among children and adolescents in the context of experience-dependent interventions and, if so, what are those changes and how do they relate to functional outcomes?; and (4) What are the implications for future research?
Methods
Search strategies
A systematic review of the literature was conducted in January through March 2018, adhering to PRISMA guidelines. 24 The review process included a comprehensive search of the following databases: Scopus, PubMed, and PsychINFO. To identify articles, we used two main search queries: Plasticity + Neuroimag* + Child* (P + N + Child*) and Plasticity + Neuroimag* + Adolesc* (P + N + Adolesc*).
Eligibility criteria
Studies were included in the present review based on the following criteria: (1) original research; (2) included a treatment intervention that aimed to facilitate neuroplasticity and a neuroimaging technique (i.e. functional magnetic resonance imaging (fMRI), diffusion tensor imaging (DTI), and magnetic resonance imaging (MRI)) both with pre- and post-measures; (3) was published in English; (4) included human participants only (i.e. animal studies were excluded); (5) included children and/or adolescents (i.e. 18 or younger); and (6) articles were published between January 2008 and March 2018. Articles were excluded if they met one or more of the following exclusion criteria: review article, case study, open study, method or proof-of-concept paper, no treatment intervention utilized, and not written in English.
Data collection and extraction
The eligibility of the studies was examined by two investigators using a standardized data extraction form, and full consensus was reached on the studies included in the review. Information including publication year, sample size, and population characteristics was collected along with two other key components—intervention and imaging data. A description of the type of intervention including frequency and duration and pre and post-intervention measures along with type of neuroimaging performed, regions of interest (ROIs), and pre and post-measures was extracted from each individual study.
Results
Search results
The search yielded 1122 articles (Scopus = 387, PubMed = 520, and PsychINFO = 215). Duplicates within each database search were removed (Scopus = 94, PubMed = 12, and PsychINFO = 20) and an additional 7 duplicates between the databases were removed. After removing journal articles that did not meet inclusion criteria, 82 article titles and abstracts remained. Of the 82 articles, 32 met the inclusion criteria of the study and were eligible for full article review. Upon further review, three additional articles were excluded as they did not include a treatment intervention with pre- and post-measures, and an additional article was excluded because it was a case study. This process resulted in a final total of 28 articles meeting all inclusion criteria (see Figure 1).
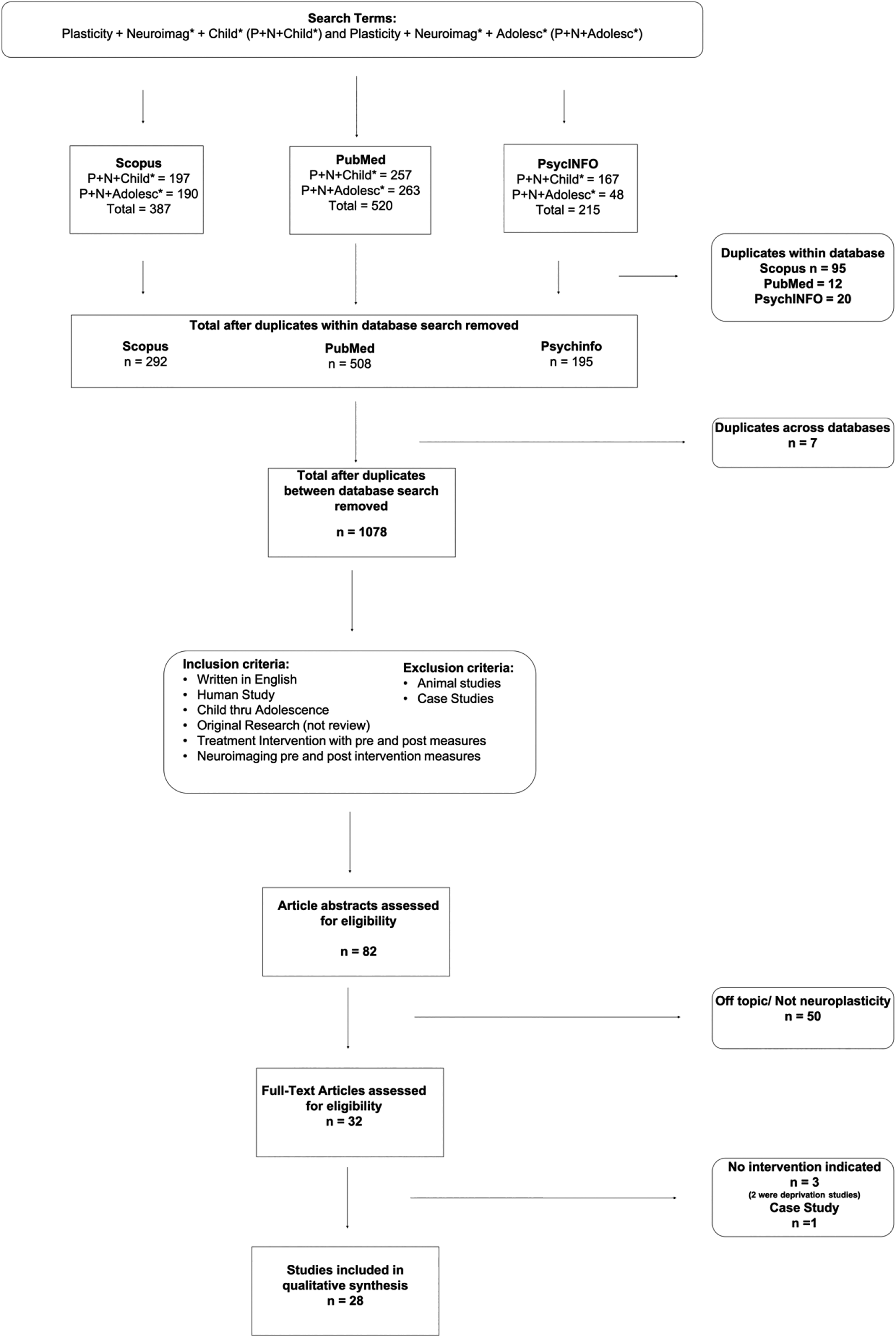
Flow diagram of the selection process of studies on neuroplasticity in children and adolescents (PRISMA, Moher et al. 24 ).
Baseline characteristics of studies
Significant variability existed across the 28 studies with regard to the type of clinical population studied, the type of experience-dependent intervention employed, intervention frequency and delivery method, timing of assessments, neuroimaging method, and type of data extracted from that imaging. Table 1 provides a summary of the study characteristics for the 28 included studies. The majority of the studies (57%) were conducted in the United States (n = 16), three in Canada, one in the United Kingdom, two in the Netherlands, one in Germany, one in Switzerland, one in Spain, one in Iran, one in Israel, and one in Japan. Most of the studies conducted in the United States were conducted in California and Massachusetts (four studies in each state), two in Alabama, and one study each in New Jersey, New York, Ohio, Pennsylvania, Texas, and Wisconsin. Studies were published between 2008 and 2018; the median publication year was 2015. Eighty-two percent of the studies (n = 23) were published with in the last 5 years.
Review of studies assessing neuroplasticity in children and adolescents: Summary of study characteristics.
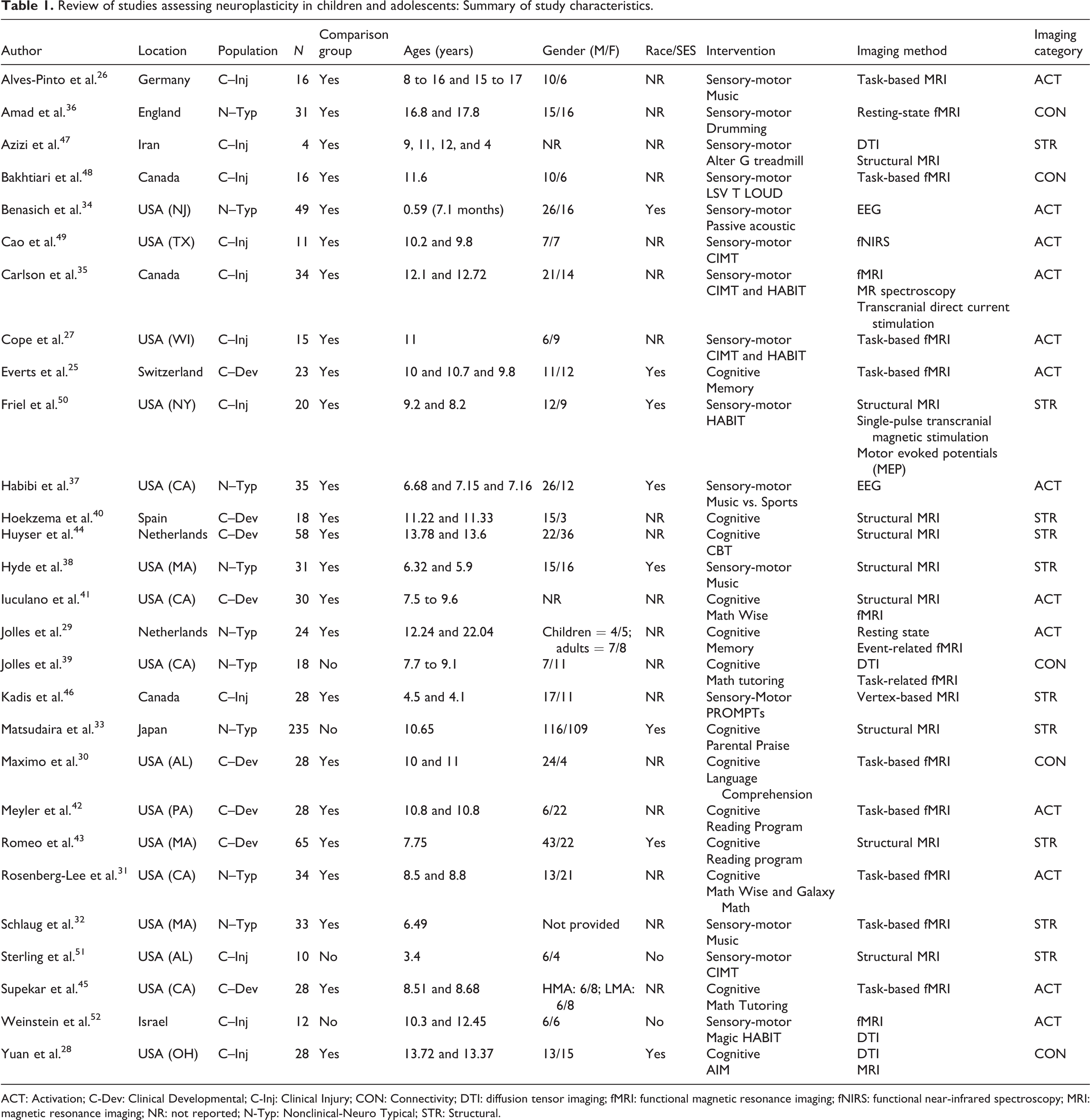
ACT: Activation; C-Dev: Clinical Developmental; C-Inj: Clinical Injury; CON: Connectivity; DTI: diffusion tensor imaging; fMRI: functional magnetic resonance imaging; fNIRS: functional near-infrared spectroscopy; MRI: magnetic resonance imaging; NR: not reported; N-Typ: Nonclinical-Neuro Typical; STR: Structural.
Plasticity terminology and measurement
Among the 28 reviewed studies, broad and more specific terms for neuroplasticity were used. Most of the studies used the term plasticity (n = 13) or neuroplasticity (n = 8). Alternative terms included neural change, neuronal change, neural plasticity, functional connectivity, brain connectivity, experience-dependent structural change, experience-dependent plasticity, and developmental plasticity. 25–34 Furthermore, even broader terms for plasticity were used in some studies, such as neuromodulation. 35 The terminology of plasticity in studies correspondingly influenced the selection of imaging modality.
Description of samples
Sample sizes ranged from 4 to 235 (M = 34.36, SD = 41.63) resulting in a total of 962 participants. There was one outlier study with 235 participants. Excluding that study is more reflective of the remaining 27 studies with a sample size ranging from 4 to 65 (M = 26.92, SD = 13.94) resulting in a total of 727 participants. Gender (binary only) was reported in 25 of the studies for a total male/female ratio of 463/408. Age was reported in all 28 studies; mean age ranged from 0.59 to 17.3 years. Across all studies, the mean of mean ages was 9.43 years.
Description of study populations
The high degree of heterogeneity of sample participants across all 28 studies led the authors to categorize each study into one of three groups based on the clinical or nonclinical diagnoses (see Figure 2).

Distribution of studies by clinical population category. Key: Non-italicized = sensory-motor intervention; italicized = cognitive-based intervention.
All studies assessing nonclinical, that is, neurotypical populations (n = 9) were assigned into the Nonclinical Typical grouping (N-Typ). 29,31–34,36–39 Studies that included individuals with a diagnosed developmental disability (n = 8) were assigned into the Clinical Neurodevelopmental (C-Dev) group. These studies included individuals that were born preterm or were diagnosed with attention deficit hyperactivity disorder (ADHD), learning disabilities, obsessive compulsive disorder (OCD), math anxiety, or autism spectrum disorder. 25,30,40–45 Finally, studies that assessed individuals with a neurological injury diagnosis were assigned into the Clinical Neurological Injury (C-Inj) group. This included diagnoses of apraxia, traumatic brain injury, and cerebral palsy including spastic hemiplegia. 26–28,35,46–52
Description of interventions
All 28 studies examined the effects of an experience-dependent intervention employing a variety of behavioral outcome measures. These interventions were either cognitive (n = 13) or sensory-motor focused (n = 15) (see Table 1). Four studies in the N-Typ category, 29,31,33,39 eight studies in the C-Dev category, 25,30,40–45 and one study in the C-Inj category 28 used cognitive training interventions. Five studies in the N-Typ category 32,34,36–38 implemented sensory-motor interventions using either music or auditory-related interventions. There were no studies in the C-Dev category that examined experience-dependent plasticity among children and adolescents using a sensory-motor intervention. Ten studies in the C-Inj category examined experience-dependent plasticity among children and adolescents using a sensory-motor intervention. 26,27,35,46–52
The type of intervention appeared to be closely correlated with the clinical population that was being studied (see Figure 2). For example, children and adolescent participants that had a motor impairment such as speech apraxia were treated with a sensory-motor intervention which focused on improved motor function, while individuals with a learning disability were treated with a cognitive-based intervention focused on those skills (i.e. reading or math). Nonclinical populations assessed both types of interventions approximately equally.
Description of intervention delivery, frequency, and duration
The studies in this review demonstrated inconsistent reporting regarding the intensity, volume, and frequency of the interventions employed. Six studies did not report any of this information while the remaining studies reported significant variability ranging from 20 min one time a week to 6 h a day for 5 days a week. Duration and mode of delivery of interventions was reported in all 28 studies. The median duration was 8 weeks; however, the majority of interventions (79%) were 16 weeks or less (see Table 2). Five of the 28 studies, or 18% of the articles, investigated the effects of long-duration interventions that lasted longer than 16 weeks on neuroplasticity of children or adolescents. 26,32,33,37,38 The majority of the studies (75%) employed interventions that were delivered 1:1 while 11% were delivered as a group and 14% compared 1:1 to group.
Review of studies assessing neuroplasticity in children and adolescents: Summary of behavioral interventions and imaging.

C-Dev: Clinical Developmental; C-Inj: Clinical Injury; DTI: diffusion tensor imaging; fMRI: functional magnetic resonance imaging; fNIRS: functional near-infrared spectroscopy; MRI: magnetic resonance imaging; NR: not reported; N-Typ: Nonclinical-Neuro Typical; BOLD: blood-oxygen-level-dependent; ROI: region of interest.
Description of neuroimaging
There was substantial heterogeneity in imaging modality employed, processing pipelines, and analytical approaches across studies (see Table 2). The neuroimaging modality or combination of modalities differed among the studies, demonstrating the flexibility of neuroimaging to identify and localize changes in plasticity in response to an intervention. MRI (n = 8), fMRI (n = 10), DTI (n = 1), functional near-infrared spectroscopy (fNIRS) (n = 1), and electroencephalography (EEG) (n = 2) were used by the studies reviewed here. Furthermore, several studies used multimodal imaging to investigate neural changes or brain structure, combining fMRI and structural MRI; DTI and task-based fMRI; fMRI, magnetic resonance spectroscopy, and transcranial direct magnetic stimulation (TMS); structural MRI and TMS; MRI and DTI; and fMRI and DTI. 28,35,39,41,50,52 Based on imaging modality and measurement of plasticity, studies were grouped into three categories. These groups reflect how the study’s authors interpreted and measured neuroplasticity as (a) changes in brain structure (STR) (n = 10), 32,33,38,40,43,44,46,47,50,51 (b) activation of regions of interest (ACT) (n = 13), 25–27,29,31,34,35,37,41,42,45,49,52 or (c) functional connectivity (CON) (n = 5) 28,30,36,39,40 (see Table 1; Figure 3).
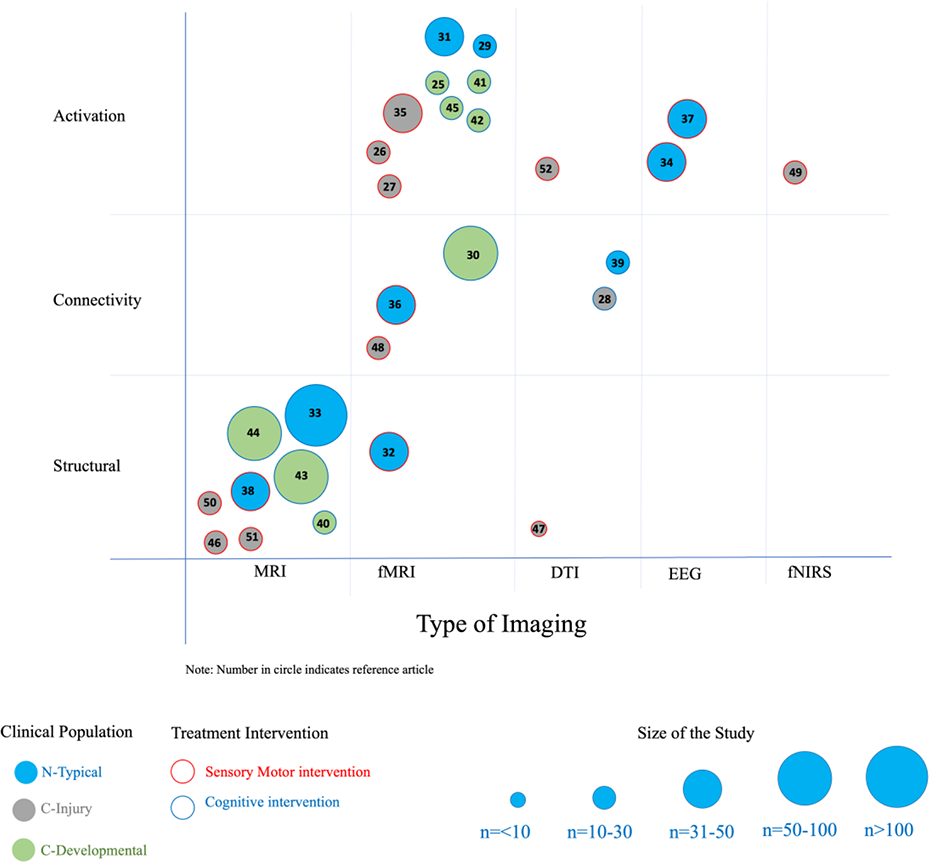
Overall distribution of neuroplasticity studies by type of imaging including population category, type of imaging, and sample size. Note: Number in circle indicates reference article.
The studies identified in this systematic review measured neuroplasticity using single or multimodal imaging strategies based on the authors’ working definition of plasticity and the specific research questions. Neuroimaging modalities differ in their spatial resolution, temporal resolution, and signal of interest that approximates or directly measures neural activity. fMRI relies on the detection of blood-oxygen-level-dependent (BOLD) signal to indirectly measure neuronal activity. 53 Task-based fMRI provides information about regions of activation in response to a cognitive, motor, or sensory task. By contrast, resting-state fMRI detects spontaneous changes in the BOLD signal without task presentation and resting-state fMRI is commonly used to approximate the functional connectivity of brain regions. 53 Acquiring fMRI images from children is particularly challenging given the environment of the scanner and the duration of acquisition. 54
Similar to fMRI, the neuroimaging method fNIRS approximates neuronal activity as a function of metabolic demand and cardiac perfusion, which is referred to as neurovascular coupling. 55 fNIRS measures changes in near-infrared light absorption to indirectly measure changes in the concentration of oxyhemoglobin and deoxyhemoglobin. 56 In comparison to fMRI, fNIRS has a shorter acquisition period and is both portable and robust. 49 Unlike fNIRS and fMRI, which indirectly measure brain activity, structural MRI measures changes in structure, such as alterations in volume or thickness of gray matter. DTI was also used in some of the studies. The principle of DTI image contrast relies on the anisotropic diffusion of water molecules along axonal tracts in white matter when a gradient is applied that increases magnetic field strength in one direction. 57 After fiber tract reconstruction by tractography or fMRI-guided fiber tracking, valuable information can be obtained about white matter microstructure and axonal tract orientation. 58,59
Methodological heterogeneity and limitations of selected studies
Neuroimaging results are dependent on instrument parameters of the imaging modality employed and on strategies used to define and detect low-quality data, remove noise and artifacts, and prepare the data for statistical analyses. 60 –63 The order of preprocessing steps is subject to researcher discretion based on the imaging protocol and research questions. To date, there is a lack of agreement in the neuroimaging field about the order of preprocessing steps. 64,65 The multiple steps of preprocessing and processing steps are referred to as “pipelines” for preprocessing and processing. Below, we briefly discuss the processing pipelines of the reviewed studies.
Preprocessing and data quality control
Before analyzing and interpreting neuroimaging data, it is important to check the quality of the acquired images. Researchers can assess data quality using a variety of approaches such as visual inspection of data, removal of scans with excessive noise, band-pass filtering, shim correction, and algorithms. 64 Data quality control may also be assessed by calculating signal-to-noise ratios and contrast-to-noise ratios. 66 Of the 28 articles reviewed, four studies did not report data quality control measures in their preprocessing methods. 28,32,33,40 Several studies reported visual inspection of data quality or signal prior to data processing. Four studies, or 14.3% of the articles reviewed, inspected data quality for quality before analysis. 34,37,43,44 Two studies reported quality control strategies for EEG recordings. 34,37
Capturing accurate, physiologically relevant signals and quality data is important for downstream analysis. A common strategy for stabilizing the signal of fMRI time series is to remove data from the first several runs or volumes for each scan to improve quality and signal detection. Five studies reported using this strategy. 25,41,45,48,52 Signal can be additionally be improved by applying a linear shim correction to each slice during reconstruction. 67 Four studies reported using this technique during MRI acquisition to optimize magnetic field homogeneity, reduce blurring, and improve signal. 31,41,43,45 It is important to note that a specific issue for fMRI data is the acquisition time required to sample multiple slices and stack them into a three-dimensional image, which can result in temporal errors in fMRI time series data, or “offset delays, which can be corrected for using slice timing correction methods before or after motion correction.” 64 Only 4 of the total 14 fMRI studies reviewed here carried out slice-time correction on acquired functional images prior to processing the data. 31,36,41,45 Additionally, applying a frequency filter to neuroimaging data is a widely used method for removing nonneuronal physiological artifacts and improving signal detection. 68 Five studies used band-pass filtering to limit data collection to relevant signals. 30,34,36,37,49
Motion detection and correction methods
Motion artifacts in neuroimaging data can cause systematic disruptions in image resolution, such as blurring and ghosting artifacts, which occur more frequently in pediatric populations. 69–71 Motion during imaging is time-locked to the acquired images, so it is necessary to effectively correct for motion before analyzing and interpreting data. 72 –74 Furthermore, motion during diffusion-weighted imaging can affect mean diffusivity and fractional anisotropy metrics whereas movement during task-based fMRI can result in spurious activations, especially for movement tasks. 75 Given that motion during image acquisition affects the quality of neuroimaging data, we discuss several important methods used by the reviewed studies to address this concern. Improving image quality by increasing the signal-to-noise ratio affects the accuracy of later processing steps, such as segmentation. 66 Therefore, it is crucial that motion artifacts in neuroimaging data are corrected for before data analysis and interpretation. 76,77 Five of the 28 articles, or 17.8% of the studies reviewed, did not correct for motion in their neuroimaging data or report motion correction procedures in the methods section. Four of the reviewed studies, or 14.3% of the studies, reported using default software settings to remove motion artifacts from the imaging data as a preprocessing step. 29,36,42,47 Reporting motion thresholds in the methods section of an article provides transparency about how the authors quantified motion artifacts during pre- or post-processing. 66 Of the 28 articles reviewed, 6 studies listed the motion threshold for images acquired using MRI and DTI. 25,26,41,45,48,52 Three out of the 28 articles used de-spiking procedures to correct for deviant volumes that arose from spikes in movement. 31,41,45
Several studies monitored movement during image acquisition to detect head motion or eye movements. 34,35,37 EEG recordings are susceptible to ocular artifacts, such as eye movement and blink artifacts. 78 Two out of the 28 articles included in this review used EEG to measure neuroplasticity. 34,37 Benasich et al. and Habibi et al. monitored eye movements from EEG recordings using electrodes located above and lateral to the eyes. 34,37 Moreover, Benasich et al. played movies or conducted silent puppet shows to hold infants’ attention during EEG acquisition. 34,37,78 Two studies removed motion artifacts from neuroimaging data after image acquisition by modeling motion artifacts as nuisance regressions in a general linear statistical model of the physiological signal of interest. 27,30
Several studies described familiarizing and acclimating participants with the scanning environment prior to neuroimaging to reduce motion during actual data acquisition. Weinstein et al. noted that participants in their study practiced lying in a mock scanner before the MRI scan and a movie was played during the scanning session while the child’s guardian was present in the room to reduce movement and anxiety. 52 Additionally, during the fMRI motor task, videos were recorded to monitor mirror movements that were rated retrospectively by the authors using the Woods and Teuber scale. 79 Jolles et al. also familiarized participants with the MRI scanner environment before scanning sessions and provided detailed instructions to participants prior to acquiring fMRI images. 29 Friel et al. provided participants with a tour of the MRI center and offered a simulation of the MRI setup by allowing the participants to lie in a tunnel while wearing a baseball catcher’s mask to simulate a head coil while listening to MRI sounds. 50 During the actual scanning session, participants watched a movie of their choice and the child’s guardian was present in the room. 50 Head restraints and head molds are additional methods that can be used to deter motion during imaging. 50,80 Of the 28 reviewed articles, two studies reported using foam pads or pillows to reduce movement or muscle tension during imaging. 44,50 Additionally, sedation during pediatric neuroimaging helps to control for motion during data acquisition as previously described in the literature. 81,82 Of the 28 articles reviewed here, one study reported using propofol to sedate participants before acquiring structural MRI images. 51
Statistical analyses
In the studies reviewed, missing data were a prevalent issue in studies with multiple neuroimaging time points. To correct for missing data, some studies removed scans from the participant that missed a session. Removing participants’ scans due to a missed imaging session is an example of a deletion method for handling missing data. Deletion methods may introduce bias and reduce statistical power, especially if there is a small sample size to begin with. 83,84 Existing methods for correcting for missing data include likelihood-based methods, multiple imputation, and weighting. 84 Two studies used strategies to address missing data in their analyses. Friel et al. interpolated missing data based on the group average from 6-month time point and Hyde et al. replaced missing data with the series’ mean. 38,50
Second, although many studies reported p values for statistical tests, few reported effect size estimates. Providing estimates of effect size, such as beta-values from regression models, eta squared values, and Cohen’s d values, provide meaningful information and increase interpretability of results. 85 Five of the 28 reviewed studies reported estimates of effect size to describe the magnitude of an observed outcome. 28,31,32,35,51 Yuan et al. standardized continuous variables and calculated parameter estimates using a mixed model for dependent variables; the coefficients were subsequently treated as mean differences. 28 Furthermore, Rosenberg-Lee et al. and Sterling et al. reported Cohen’s d values as estimates of effect size whereas Schlaug et al. included eta squared values in the results. 31,32,51
Lastly, when multiple hypothesis tests are conducted, there is an increased risk of incorrectly rejecting a null hypothesis, which can result in type I error, or false positives. 86 This is particularly relevant to neuroimaging analytical methods. 86–88 Of the 28 papers reviewed, 7 studies did not report corrections for multiple comparisons. 25,27,29,35,36,46,47 Two articles reported that multiple comparison tests were not carried out due to the small sample size of the study. 27,46 Similarly, Carlson et al. did not correct for multiple comparisons because of the low number of comparisons made during analysis. 35 The 20 articles that reported multiple correction methods used various statistical approaches, including family-wise error rate (FWER) correction, false discovery rate (FDR), Monte Carlo simulations, Tukey tests, and Bonferroni tests. 26,28,30–34,37,38,40–45,51,52 One study conducted post hoc Tukey tests and reduced the degrees of freedom using Greenhous-Geisser epsilon to reduce the risk of type I error. 37
Discussion
Key measures and analytical techniques
A main aim of the review was to identify key measures and analytical techniques used within the neuroplasticity literature pertaining to children and adolescents. Results revealed substantial variability among studies with respect to types of cognitive and sensory motor interventions as well as delivery protocol, frequency, and duration of interventions. For example, duration of interventions varied from 20 min once per day to 6 h per day for 5 days per week. Delivery protocol also varied; however, 75% of studies used one-to-one delivery while the others used group methods. Given the heterogeneity across studies, results remain equivocal; however, findings do suggest that intervention studies of longer duration likely have a more robust influence on neuroplastic changes than those of shorter duration. With regard to specific type of intervention, the present review was unable to determine whether sensory-motor interventions or cognitive interventions were more impactful as several neuroimaging findings supported alterations in functional connectivity, volumetric changes, changes in neural activation, or other parameters of neuroplasticity; however, two cognitive interventions and two sensory-motor interventions had inconclusive imaging findings (Table 2). 29,35,39,46 Similarly, findings across studies were inconsistent with respect to whether cognitive or sensory motor interventions had a larger impact on neuroplastic changes across age and type of disability. Replication of designs using larger samples, varying ages, and different types of disability along with effect size information is vital for understanding these potential relationships.
In terms of analytical techniques, there was substantial heterogeneity in imaging modality employed, processing pipelines, and approaches across studies. The majority of studies employed MRI or fMRI. In terms of analyses, most studies used multivariate or cluster-level analytical techniques and/or multiple analyses using the general linear model. Of the 28 articles reviewed, 5 studies, or 17.9% of the articles, described using nonparametric statistical tests such as the Wilcoxon signed rank test and Spearman rank correlations when data violated normality assumptions of the general linear model. 25,27,28,35,49 Although there was heterogeneity in statistical methods across the studies, 46%, or 13 of the 28 reviewed articles, reported using analysis of variance models. 25,32,34–37,39,42,44,45,48–50 As discussed in the next section, these different approaches affect the methodological strengths and limitations of the studies, as well as the interpretation of the findings.
Methodological strengths and limitations
In response to the second aim of the review, findings revealed important methodological limitations among the studies. Specifically, differences existed in terms of variations of imaging modality, sample sizes, order and number of steps of preprocessing and data processing pipelines, leading to a multiplicity of analytical methods. It is understandable that different imaging protocols and experimental designs may require specialized pipelines for preprocessing and processing of neuroimaging data; however, it is important that researchers are transparent in reporting the preprocessing and processing steps and statistical analyses used to increase the validity and reproducibility of experiments. MRI and fMRI data obtained from pediatric populations typically has more motion artifacts and lower quality imaging data compared to adult populations. 69,70 Similarly, segmentation and quantification of brain regions taken from high-resolution MR images can have a significant impact on imaging findings. 89 Eleven of the 28 studies (39%) included in the present review were volumetric neuroimaging studies. Brain size and shape differs substantially among children and it is therefore especially important to correct for intracranial volume (ICV). 90 In the current review, however, only 7% of the studies reported ICV correction methods. Consequently, the impact on the findings from the remaining studies that did not employ correction procedures is suspect but unknown. 33,43 Additionally, only two studies reported that blind observers checked neuroimaging data for motion artifacts, accurate segmentation, or correct identification of structures of interest. 32,43 Sterling et al. reported that a second investigator inspected the accuracy of lesion masks. 51 Including post-processing inspections and combining manual data inspection with automated software processing improve validity. Likewise, reporting and sharing methods for neuroimaging studies that provide specific guidelines for future studies will be critical in improving quality and validity. 64,91 –93
Motion detection is a major methodological concern of this review as MRI data obtained from pediatric populations has increased motion artifacts compared to older populations. The studies included in the present review that addressed artifacts (not all did) used a variety of methods to detect, limit, and remove movement from neuroimaging data. It is possible, however, to prospectively correct for artifacts in neuroimaging data caused by head motion during scanning acquisition to reduce motion artifacts and improve data quality. 94 Examples of prospective motion correction techniques include BLADE/PROPELLER MRI and PROMO. 95,96 PROMO utilizes interleaved spiral navigator scans and image-based tracking to ensure that the relationship between the imaged object, subject to motion, is constant with the imaged volume by adjusting MR pulse sequences as the pose (orientation) of the object changes during scanning. 94,97 It is critical that future neuroimaging studies report methods for motion correction, including the parameters for motion threshold, so that effective methods can be adopted to improve the quality of images and increase the validity of statistical analyses based on imaging results. 69
A third methodological problem of many of the studies reviewed pertains to statistical power and risk of type I or II error. Power analysis requires an estimate of the effect size. 98 In the present review, only five of the studies (17.8%) acknowledged statistical power or effect size. 27,39,41,49,50 Adequate sample size is necessary for a study to have sufficient power. In the present review, 35.7% of studies (10 out of 28 articles) had total sample sizes of 20 participants and under. 26–28,40,47–52 Only 4 of the 28 studies (14%) conducted analyses with total sample sizes greater than 50. 30,33,43,44 To increase transparency and interpretation of research findings, future studies are encouraged to report power analyses conducted to determine sample size and effect sizes of research outcomes in conjunction with p values.
Further, many of the studies used multiple hypothesis tests comparing brain voxel activations to zero for each voxel of the brain. Functional neuroimaging data can consist of 100,000 voxels, each voxel corresponding to specific spatial locations in the brain with different intensity values and the more hypothesis tests conducted, the higher likelihood of a false positive. 86–88 Future studies are encouraged to employ statistical methods to reduce the likelihood of false positives; use built-in automated processes for image segmentation; use theory to select apriori brain regions of interest for analysis; and employ multiple comparison corrections. 99 –101 Notably, of the 28 studies in this review, less than 50% used a priori ROIs based on previous literature to guide neuroimaging data collection and analysis. 25,29,30–33,35,37,39,40,41,43–46,49,51
Additional methods that are often used for whole brain analysis to quantify the likelihood and thus control for false positives, include the family-wise error rate (FWER) which may include Bonferroni correction, random field theory (RFT), and permutation tests, as well as the false discovery rate (FDR). FWER Bonferroni correction is a conservative method of controlling for type I error by determining the rate of false positives among all statistical tests. 102 Due to the stringency of Bonferroni adjustment for multiple tests and strict significance levels, it is possible that researchers may not detect statistically significant differences. 86 By contrast, FDR controls for false positives among statistically significant tests where the null hypothesis is rejected. 86 For exploratory studies and health studies, FDR is a more liberal correction method compared to Bonferroni adjustment that provides more sensitivity and power for detecting statistical differences while correcting for type I errors. 103 RFT is commonly used for cluster-level corrections of neuroimaging data. 86 The specific methods employed to account for false positive findings included FDR, FWER, and Monte Carlo simulations, as well as broadly termed whole brain methods. Only three of the studies reviewed here controlled for FDR, which typically involves rejecting a number of hypotheses in order to maintain the FDR below a predetermined level, or specified a more sophisticated known approach for controlling for FDR (i.e. a hidden Markov Random Field model). 28,38,52,87,104 FWER with a Bonferroni correction was employed by one study and two studies used Monte Carlo simulations to establish more stringent thresholds to account for assumptions of independence. 32,105,106 We direct readers to reviews of methods for analysis of neuroimaging data for further information about statistical approaches. 107,108
Lastly, an important methodological consideration pertains to data registration. Due to the global and local neuroanatomical changes that occur during development in children and adolescents, it is necessary that researchers use age-specific MRI templates rather than adult templates for accurate registration, spatial normalization, and segmentation. 66 A commonly used practice for registering pediatric neuroimaging data to a reference template is registration to adult brain atlases MNI305 and MNI152 followed by corrections for pediatric brain anatomy. 109,110 The disparities in shape, morphology, and size of an adult brain compared to a brain of a child brain result in errors in segmentation and increased deformations in nonlinear transformations when adult templates are used as a reference for pediatric neuroimaging, generating variabilities and less robust registration. 111 Warping or applying nonlinear deformations to fit linear brain atlases to neuroimaging data from individuals with morphometric differences results in more accurate registration. 112 Furthermore, registering pediatric brain scans to adult brain atlases or templates can result in inaccurate classification of brain tissue. 113 Researchers have the option of using open-access brain atlases constructed from pediatric datasets from Cincinnati Children’s Hospital Medical Center, IDEA group, and Johns Hopkins University, among other resources for normalization and segmentation of neuroimaging acquired from pediatric populations. 66 Furthermore, Richards et al. generated a Neurodevelopmental MRI Database of age-specific MRI reference templates ranging in age from 2 weeks to 89 years old. 113
In addition to the methodological problems characterizing many of the studies discussed herein, there are several limitations of the review that are important to acknowledge. It is possible that studies not meeting inclusion criteria for the present review may have yielded different findings. Available research may be biased toward positive results, that is, data not supporting neuroplastic effects are less likely to be published.
A major shortcoming is that this review was unable to produce findings concerning potential age effects within the child and adolescent samples, and information was lacking in the studies concerning racial and ethnic diversity as well as other forms of diversity (e.g. socioeconomic status [SES], gender, and disabilities). This shortcoming is not unique to neuroplasticity studies and is unfortunately common within the field of neuroimaging. 10,114
Neuroimaging research supports the presence of neuroplasticity among children and adolescents in the context of experience-dependent interventions
Recent neuroimaging technology has allowed for an enhanced understanding of experience-dependent changes in the human brain in relation to various environmental experiences (e.g. musical training, cognitive interventions, reading and math interventions, and motor interventions). Although other animal and human adult literature provides evidence of experience-dependent neuroplasticity, a comprehensive account of these processes in the developing brain of children and adolescents is currently lacking. The purpose of the present study, therefore, was to conduct a systematic review of neuroimaging studies that have examined neuroplasticity among children and adolescents in response to a treatment intervention and to evaluate the methodological strengths and weakness of those studies. In response to the first aim, results of this review support the presence of neuroplastic changes among children and adolescents in the context of experience-dependent interventions.
Three clinical categories such as Neurotypical (N-Typ), Neurodevelopmental (N-Dev), and Neurological Injury (N-Inj) emerged from the review. Results supported that a variety of experience-dependent interventions that we defined as cognitive-based (i.e. social skills training, behavioral, or academic intervention) or sensory-motor training (i.e. music or motor-based training) were associated with neuroplastic changes across all three clinical categories. Collectively, 22 of the 28 studies included in the present review provided evidence that both structural and functional neuroplastic changes occur among children and adolescents as a result of experience-dependent intervention (see Table 2). Three of the remaining studies identified significant functional improvement across the nonclinical/clinical and nonclinical comparison groups, but no significant neuroplastic changes. 29,35,46 The other three identified significant neuroplastic changes but no significant functional improvements. 26,40,49 Although there was diversity across the populations studied regarding nonclinical versus clinical and a mix of comparison and control groups, racial, economic, and other forms of diversity remain a limitation across all studies with only 7 of the 21 studies reporting diversity information (e.g. race or SES). 43
Collectively, these studies support that children and adolescents are capable of responding to cognitively to interventions, and these cognitive changes correspond with neuroplastic changes—as measured by neural connectivity, alterations in neuronal activation across multiple areas, and increased cortical thickness in regions that are functionally related to the focus of the cognitive intervention employed. 25,30,41–43 The studies tentatively support the hypothesis that the capacity for training-induced changes related to activation, connectivity, or structure may also serve to mitigate or counteract local gray matter volumetric decreases seen in neurodevelopmental disorders such as ADHD or aberrant network connectivity as seen in individuals with MLD. 115,116
In addition to neuroplastic changes, environmental interventions were typically associated with corresponding cognitive and behavioral changes such as increased attention, planning, and memory performance, as well as improvements in motor functioning, math and reading performance. 25–31,35,39,40–43,46–52 Cognitive behavior therapy for children with OCD and anxiety was also associated with neuroplastic changes in both grey and white matter relative to a control group and these changes were positively associated with symptom severity. 44,45 As a whole, findings across the 28 studies support previous animal and adult human studies documenting the neuroplastic effects of experience-dependent activities and response to injury. 117 –120
Integrating principles of neuroplasticity in the implementation of experience-dependent activities, whether they are cognitive or sensory-motor, may be a critical component to the success of an intervention. Principles such as specificity, repetition, intensity, and salience are just a few key principles outlined by Kleim and Jones and these principles were represented among several of the studies reviewed. 121 A critical limitation, however, that needs to be addressed in future studies concerns the length of time (intensity and duration) of the studies and timing of neuroimaging studies. All studies integrated pre- and post-intervention measures. However, the overall length of the intervention varied from fairly short duration at 2 to 4 weeks (n = 9), moderately longer at 6 to 16 weeks (n = 13), and relatively few longitudinal studies that were 1 to 3 years (n = 6) (see Table 2). Critical to understanding and interpreting neuroplastic changes in brain structures, gray and/or white matter volumes, and other definitions of neuroplasticity is the inclusion of a follow-up imaging session in addition to a post-intervention imaging session. Including a long-term follow-up imaging session (third time point) allows researchers to assess the retention of changes observed at the imaging session that took place directly after an intervention or therapy program. Of the 28 articles that we reviewed, 25% of the studies reported a follow-up imaging session post-intervention, ranging from 12-weeks post-intervention to 1-year post-intervention. 34,42,48–52
Research in adult populations supports a wide range of temporal-related neuroplasticity from transient structural gray matter changes to more persistent changes which may be delayed and require several weeks to months to generate the necessary structural adaptations that might be revealed on imaging. 122,123 Integrating adequate time durations for both delivery and assessment of interventions along with neuroimaging will be important to more accurately capturing these temporal components of neuroplasticity.
Implications for future research
It is clear that there are many challenges related to studying the complexities of brain neuroplasticity in children and adolescents. However, there are also many opportunities to minimize and mitigate certain limitations, including the development of clearer guidelines for defining and measuring neuroplasticity. Based on the methodological limitations identified in the present review, future studies are encouraged to (1) increase and report racial, ethnic, and additional forms of diversity within the populations studied; (2) assess the potential age effects within the child and adolescent samples; (3) integrate defined principles of neuroplasticity (i.e. intensity, duration, and saliency) and analyze the impact of those variables on intervention and imaging outcome measures; (4) report the brain registration and extraction method and use those appropriate to pediatric samples; (5) pursue longitudinal studies with multipoint neuroimaging and behavioral and/or motor outcome assessment periods; and (6) describe the analysis workflow followed in each study. We also refer readers to the thorough review of methods in neuroimaging research by Poldrack et al. for a comprehensive list of suggestions for increasing transparency in reporting methods. 64 Inadequate reporting of analysis workflows reduces reproducibility of studies, as there are a multitude of possible pipelines for processing and analysis of neuroimaging data that can lead to variable results. 124 Implementation of these recommendations would facilitate greater understanding of the underlying factors involved in neuroplastic changes and the degree to which these morphological and neurochemical changes correspond with cognitive and behavioral change.
Conclusion
Findings of the present systematic review provide evidence of neuroplasticity in children and adolescents in response to experience-dependent interventions. However, clearer guidelines for defining and measuring neuroplasticity are sorely needed. Although neuroimaging findings shed light on structural and functional changes following a wide variety of cognitive and sensory-motor interventions, it remains unclear whether these differences are a direct consequence of molecular neuroplastic changes, the degree and direction of these differences, and the clinical implications of these findings. In order to draw meaningful conclusions about neuroplasticity in children and adolescents as a result of experience-dependent interventions, future studies should (a) explicitly and rigorously define the construct of neuroplasticity; (b) clearly describe guidelines for measurement of neuroplasticity; (c) examine questions of whether and how neuroplasticity occurs based on experimental and longitudinal designs; (d) identify the functional and structural neuroplastic mechanisms that correspond with changes in cognition and behavior; and (e) provide information about software, preprocessing of data, and analytical procedures to increase reproducibility and transparency of studies.
Footnotes
Author contributions
LW and MM conceived and designed the study. CC and SM researched the literature. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Data availability statement
Data sharing is not applicable to this article as no datasets were generated or analyzed during the current study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research reported in this publication was supported by the National Center for Research Resources of the National Institutes of Health under Award Number G20RR030883. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.