
Abstract
Purpose
Psoriasis is a chronic immune-mediated disease with global prevalence of 2-3% that is associated with significantly reduced quality of life (QoL) and worsened mental health. Despite this, there is a lack of research in African psoriasis populations, with no modern epidemiological studies conducted in Kenya to examine these factors. This study aims to identify demographic and clinical features associated with dermatology-related QoL and mental health among psoriasis patients enrolled in the newly established Kenyan Psoriasis Registry (KPR), based at Moi Teaching and Referral Hospital in Eldoret, Kenya.
Patients and Methods
In a cross-sectional analysis of 97 adult psoriasis patients enrolled in the KPR, we evaluated associations of demographic and disease characteristics with independent outcomes of dermatology-associated QoL (Dermatology Life Quality Index, DLQI), anxiety (Generalized Anxiety Disorder 7-item, GAD-7), and depression (Patient Health Questionnaire 9-item, PHQ-9). Univariate and multivariate linear regression models were used to identify associations, with P < 0.05 considered statistically significant.
Results
In univariate analyses, age, female gender, marital status, certain subethnicities, high-impact body sites, itch and pain, sleep disturbance, and disease severity were factors associated with worse QoL, anxiety, and depression scores. In multivariate analyses, younger age, Itch Numeric Rating Scale, and Patient-Reported Outcomes Measurement Information System (PROMIS) Sleep Disturbance T-score remained significantly associated with worse DLQI. Both PROMIS Sleep Disturbance and separated marital status were associated with worse GAD-7 and PHQ-9.
Conclusion
Kenyan psoriasis patients experience significant QoL and mental health burden, with younger age, itch, sleep disturbance, and separated marital status associated with worse outcomes.
Introduction
Psoriasis is an inflammatory, systemic, and multifactorial disease with increasing prevalence in both adults and children across the globe, affecting approximately 100 million people worldwide.1,2 It is classically characterized by a cutaneous presentation of erythematous plaques with scales, though the appearance can vary significantly based on skin tone. While plaques appear silvery white or pink on lighter skin tones, plaques may be more violaceous or grey and associated with more extensive scaling with hyper- and hypopigmentation in darker skin tones. Beyond its cutaneous presentation, psoriasis has increasingly been recognized to increase risk for a number of systemic conditions, including psoriatic arthritis (PsA) — occurring in approximately 30% of patients with psoriasis — cardiovascular disease, and metabolic syndrome. 3 These comorbidities, combined with pain, itch, social stigmatization, and emotional stress cause significant, measurable, and detrimental reductions in quality of life (QoL), particularly health-related QoL (HRQoL). HRQoL is a multidomain concept that represents a subset of QoL specifically linked to health status, including impacts on physical, psychological, and social functioning. For example, psoriasis patients report similar or even worse reductions in HRQoL compared to other serious chronic illnesses, such as hypertension, cancer, chronic pulmonary disease, diabetes, and ischemic heart disease. 4 Moreover, psoriasis has been associated with increased anxiety, depression, suicidal ideation, feelings of guilt and shame, reduced workplace productivity, and greater personal and national economic burden.5-9
Although psoriasis has a global prevalence of 2-3% and affects individuals of all backgrounds, 1 there are significant racial disparities.10-14 In particular, there are significant gaps in research investigating psoriasis in Africa, with most studies conducted thus far focused on populations in North America and Europe.15,16 The International Psoriasis Council (IPC) has highlighted the urgent public health need to quantify psoriatic disease burden in global populations, especially in resource-poor settings, so that resources can be appropriately allocated to produce equitable improvements in psoriasis healthcare globally. 17 In fact, a systematic analysis by the Global Psoriasis Atlas found that 81% of all countries globally lack basic epidemiologic data about psoriasis, particularly low- and middle-income countries. 18 This limits the generalizability of current treatment and diagnostic guidelines and exacerbates inequities in care.
Psoriasis research on the African continent is scarce despite estimated prevalence of the disease ranging from 1.9–3.5% in East Africa to 0.025–0.9% in West Africa. 19 To our best knowledge, fewer than 10 studies have examined HRQoL and the mental health burden of psoriasis in Africa, with existing research limited to Ethiopia, Madagascar, and North Africa.20-26 In these limited studies, disease severity and comorbidities were identified as factors associated with lower QoL, though results have been mixed regarding the effects of age, gender, educational status, and treatment modality.21-23,25 These studies were limited by their reliance on chart review, lack of control group, and limited generalizability due to hospital-based recruitment.
Notably, we found no modern epidemiological studies of psoriasis in Kenya, a country in East Africa that has a population of 55 million people. To address this major research gap in Kenya and the broader African continent, the University of California, San Francisco (UCSF) recently partnered with Moi Teaching and Referral Hospital (MTRH), one of Kenya's two national referral hospitals that serves approximately 24 million people, to establish the first clinical and genetic psoriasis registry in Kenya, termed the Kenyan Psoriasis Registry (KPR). The KPR prospectively enrolls both psoriasis patients and healthy controls using broad community recruitment strategies and employs comprehensive, validated methods of assessment. Prior work by our group confirmed Kenyan psoriasis patients to have significantly lower educational attainment and worse HRQoL, sleep disturbance, anxiety, and depression compared to controls. However, factors predicting worsened dermatology-related QoL and mental health in this population have remained unexamined. Consequently, in the present study, we present a cross-sectional analysis of patients enrolled in the KPR to identify demographic and clinical determinants of mental health and QoL, aiming to be one of the first to explore these relationships among Kenyan psoriasis patients.
Methods
Study Population, Setting, and Design
A total of 108 psoriasis patients were enrolled into the KPR at MTRH between October 2024 and August 2025 through broad recruitment strategies, including from outpatient MTRH dermatology clinics and community advertisements. Inclusion criteria for psoriasis subjects included history of dermatologist-confirmed psoriasis of any type (plaque, guttate, inverse, palmoplantar, pustular, and/or erythrodermic) and age greater than 3 months, while exclusion criteria included inability to provide informed consent and/or comply with study procedures. For this analysis, we restricted our study sample to 97 adult participants aged 18 years or older, as the instruments used to measure mental health, QoL, and sleep disturbance have been validated primarily in adult populations. Written informed consent was obtained by study investigators in either English or Swahili prior to all study activities.
All study participants were confirmed to have a diagnosis of psoriasis by a dermatologist and completed a self-administered survey to collect information on sociodemographics (age, gender, race/ethnicity, education level, marital status, health insurance status, employment, residence), alcohol and smoking history, environmental exposures, psoriasis clinical and treatment history, family history, comorbidities, and validated instruments for itch and pain (Itch and Pain Numeric Rating Scale, NRS), anxiety (Generalized Anxiety Disorder 7-item, GAD-7), depression (Patient Health Questionnaire 9-item, PHQ-9), PsA screening (Psoriatic Epidemiology Screening Tool, PEST), HRQoL (Dermatology Life Quality Index, DLQI), and sleep disturbance (Patient-Reported Outcomes Measurement Information System, PROMIS, Sleep Disturbance 8b). Physician assessment of patients included height, weight, blood pressure, psoriasis subtype(s), anatomical area(s) affected, psoriasis disease severity (Psoriasis Area and Severity Index, PASI and Investigator’s Global Assessment, IGA), and body surface area (BSA). All subjects were assigned a unique identifier and confidential data were entered and securely stored in REDCap.
Statistical Analysis
We conducted univariate and multivariate linear regression analyses to evaluate the associations of demographic and disease characteristics with independent outcomes of DLQI, GAD-7, and PHQ-9, with three separate multivariate models constructed for each outcome. Prior to finalizing multivariate models, multicollinearity was evaluated using the adjusted generalized variance inflation factor (GVIF), calculated as GVIF1/(2xdf) (df, degrees of freedom), with values above 2 considered indicative of potential collinearity. Final adjusted multivariate linear regression models were then constructed using covariates satisfying one or both of the following criteria: (1) variables with P < 0.10 in univariate analysis and (2) variables determined a priori based on prior literature and clinical significance. Covariates selected a priori included demographics (age, gender, and education), substance use (alcohol and tobacco use), disease duration, psoriasis severity (PASI and IGA), PROMIS Sleep Disturbance, itch severity, pain severity, and comorbid health conditions (BMI and PsA). The final number of patients included in multivariate models was 95, with two patients excluded due to missing covariate data. Results were reported as adjusted β-coefficients and 95% confidence intervals, with P < 0.05 considered significant.
Additionally, exploratory analyses were performed to examine correlations between PROMIS Sleep Disturbance and clinical variables, including itch severity, pain severity, and PASI. All statistical analyses were performed using R software, Version 4.1.3.
Results
Cohort Characteristics
A total of 97 adult Kenyan psoriasis patients were included in the study, with sociodemographic characteristics of the study population summarized in Table S1. The mean (standard deviation, SD) age was 45.9 (14.8) years, and most participants were female (58.8%). Clinical characteristics are summarized in Table S2, with the mean (SD) age of psoriasis onset being 32.5 (16.0) years and the mean (SD) age of diagnosis being 41.9 (15.4) years. 13.4% of participants had a family history of psoriasis, and 10.3% had a medical diagnosis of PsA by patient report. The arms and legs (83.5%), trunk (57.7%), and scalp (53.6%) were the most common body sites affected, while plaque (85.6%), palmoplantar (6.2%), and guttate (5.2%) psoriasis were the most common subtypes. Clinical measures of disease severity included a mean (SD) PASI score of 9.9 (9.3) and IGA score of 2.9 (1.0). In regard to sleep disturbance, QoL, and mental health, patients reported a mean (SD) PROMIS Sleep Disturbance T-score of 41.3 (13.0), DLQI score of 7.5 (6.9), PHQ-9 score of 4.8 (4.9), and GAD-7 score of 3.1 (3.7).
Univariate and Multivariate Regression Model Results for DLQI, GAD-7, and PHQ-9
Univariate and multivariate linear regression analyses were performed to identify associations with HRQoL (DLQI), depression (PHQ-9), and anxiety (GAD-7) in 95 adult Kenyan psoriasis patients (see Methods).
Univariate and Multivariate Linear Regression Analysis for Factors Associated With DLQI
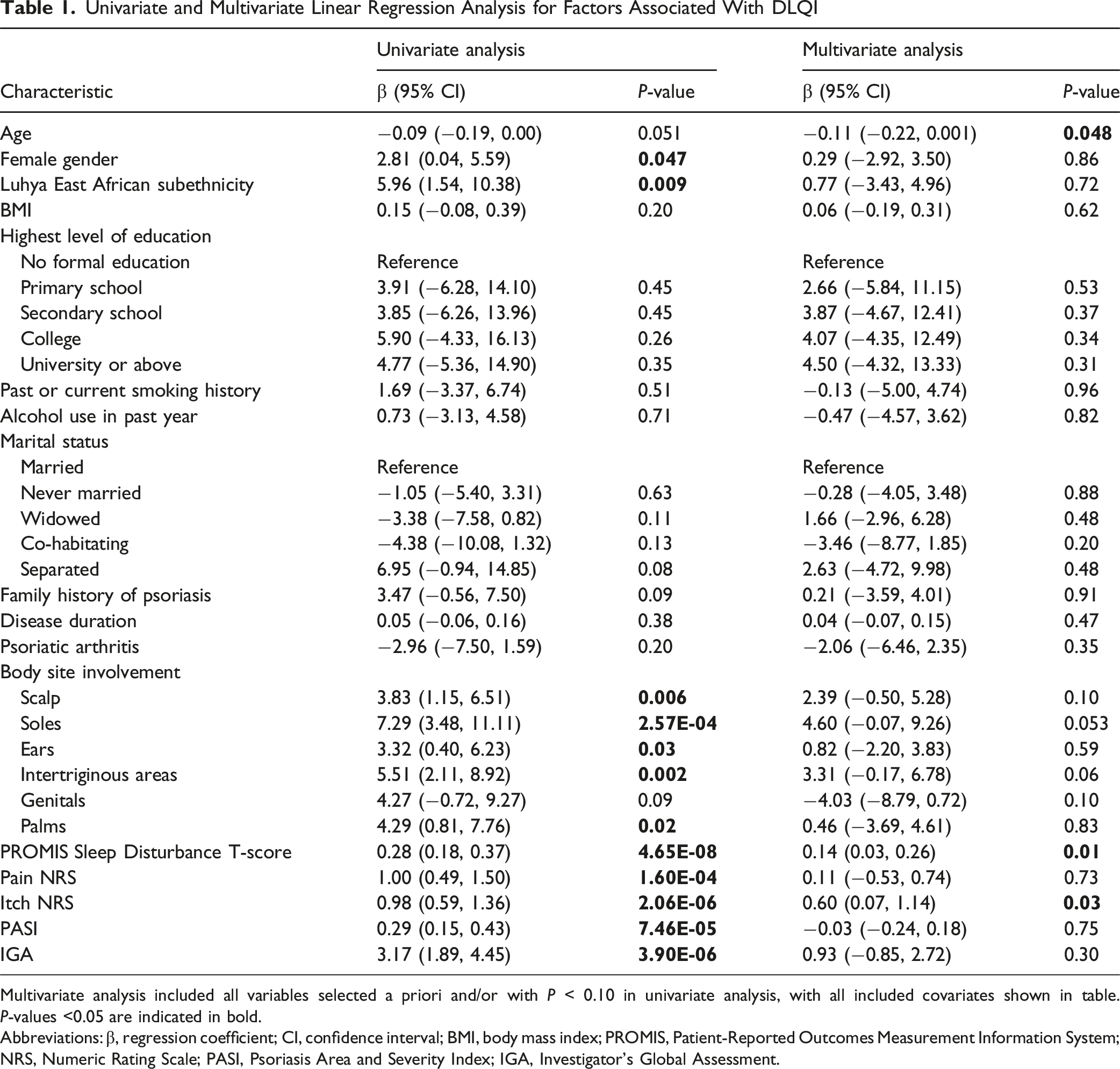
Multivariate analysis included all variables selected a priori and/or with P < 0.10 in univariate analysis, with all included covariates shown in table. P-values <0.05 are indicated in bold.
Abbreviations: β, regression coefficient; CI, confidence interval; BMI, body mass index; PROMIS, Patient-Reported Outcomes Measurement Information System; NRS, Numeric Rating Scale; PASI, Psoriasis Area and Severity Index; IGA, Investigator's Global Assessment.
Univariate and Multivariate Linear Regression Analysis for Factors Associated With GAD-7
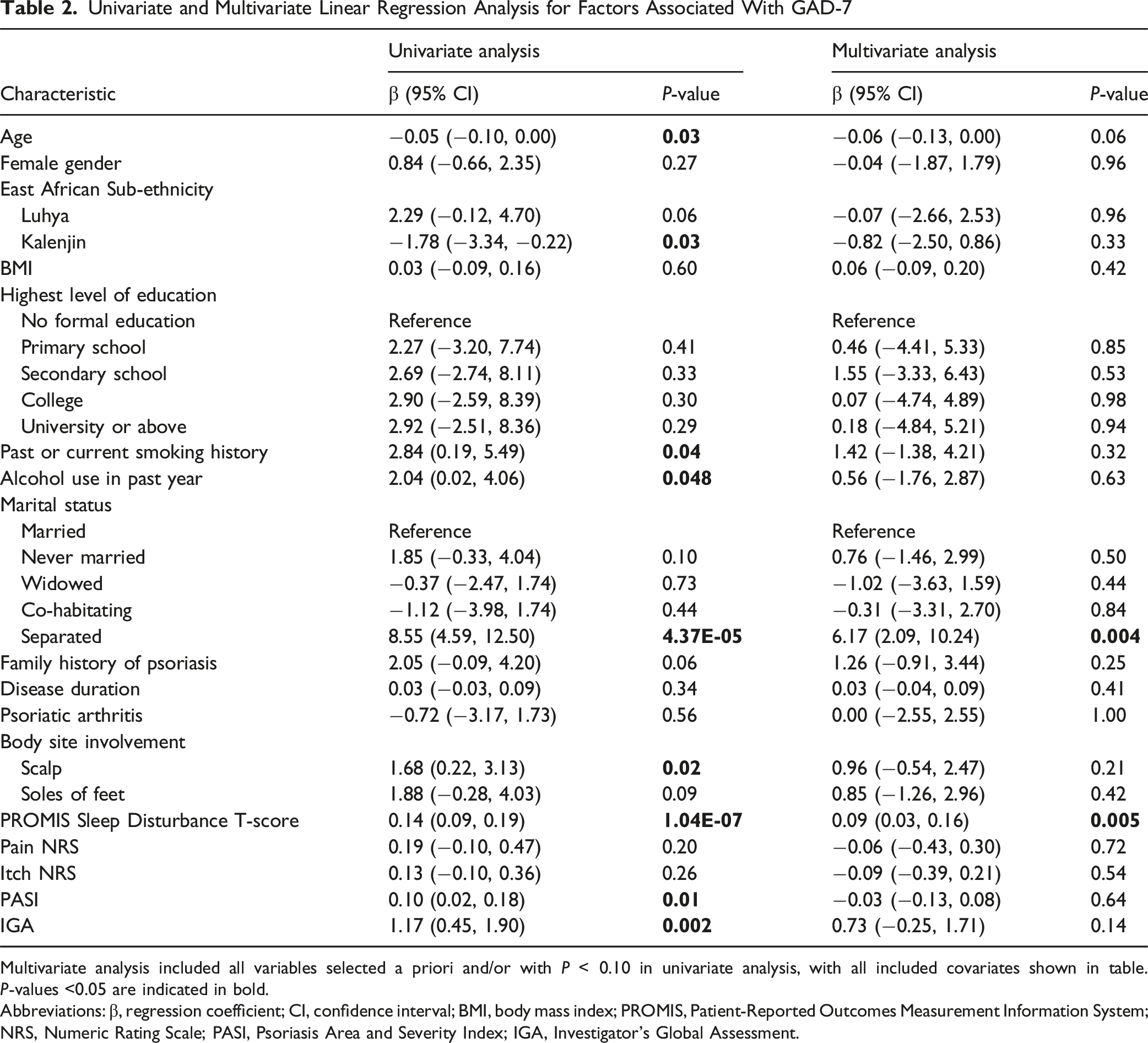
Multivariate analysis included all variables selected a priori and/or with P < 0.10 in univariate analysis, with all included covariates shown in table. P-values <0.05 are indicated in bold.
Abbreviations: β, regression coefficient; CI, confidence interval; BMI, body mass index; PROMIS, Patient-Reported Outcomes Measurement Information System; NRS, Numeric Rating Scale; PASI, Psoriasis Area and Severity Index; IGA, Investigator's Global Assessment.
Univariate and Multivariate Linear Regression Analysis for Factors Associated With PHQ-9
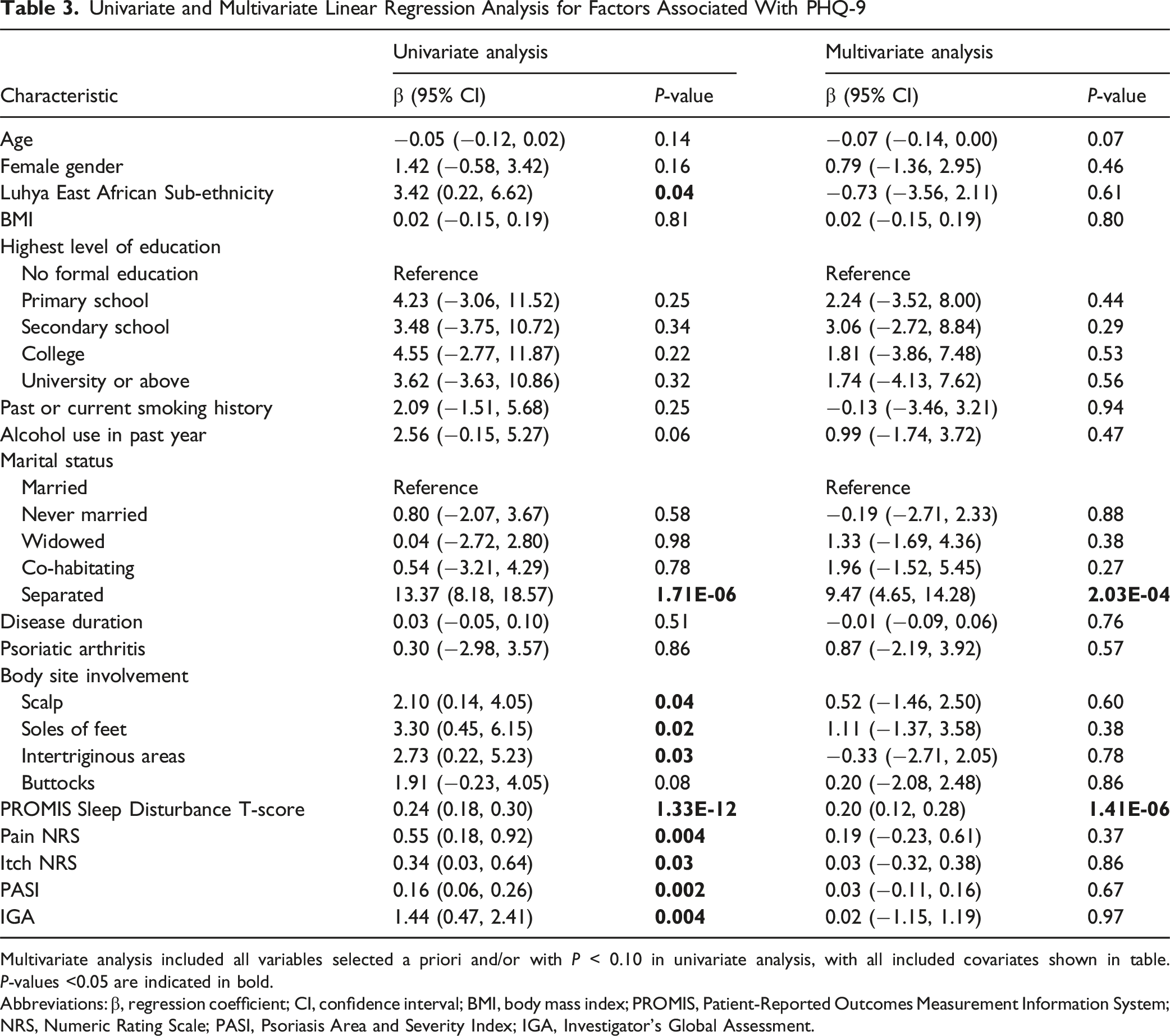
Multivariate analysis included all variables selected a priori and/or with P < 0.10 in univariate analysis, with all included covariates shown in table. P-values <0.05 are indicated in bold.
Abbreviations: β, regression coefficient; CI, confidence interval; BMI, body mass index; PROMIS, Patient-Reported Outcomes Measurement Information System; NRS, Numeric Rating Scale; PASI, Psoriasis Area and Severity Index; IGA, Investigator's Global Assessment.
Correlation of PROMIS Sleep Disturbance with Psoriasis Clinical Characteristics
Given that PROMIS Sleep Disturbance emerged as consistently associated with DLQI, GAD-7, and PHQ-9 in multivariate regression models, we explored its relationship with psoriasis severity and symptom measures (Figure 1). PROMIS Sleep Disturbance T-score was significantly positively correlated with PASI (β = 0.38, 95% CI 0.11–0.66, R2 = 0.08, P = 0.006), IGA (β = 3.21, 95% CI 0.58–5.83, R2 = 0.06, P = 0.02), and pain severity (β = 1.07, 95% CI 0.07–2.07, R2 = 0.05, P = 0.04), and trended towards significance with itch severity (β = 0.74, 95% CI −0.06–1.54, R2 = 0.03, P = 0.07). Correlation plots between PROMIS Sleep Disturbance T-score and psoriasis clinical characteristics. (A) PROMIS T-score vs. PASI. (B) PROMIS T-score vs. IGA. (C) PROMIS T-score vs. Itch NRS. (D) PROMIS T-score vs. Pain NRS. Linear regression lines with 95% confidence intervals are shown, with R2 and P-values indicated on each plot. Abbreviations: PROMIS, Patient-Reported Outcomes Measurement Information System; PASI, Psoriasis Area and Severity Index; IGA, Investigator's Global Assessment; NRS, Numeric Rating Scale.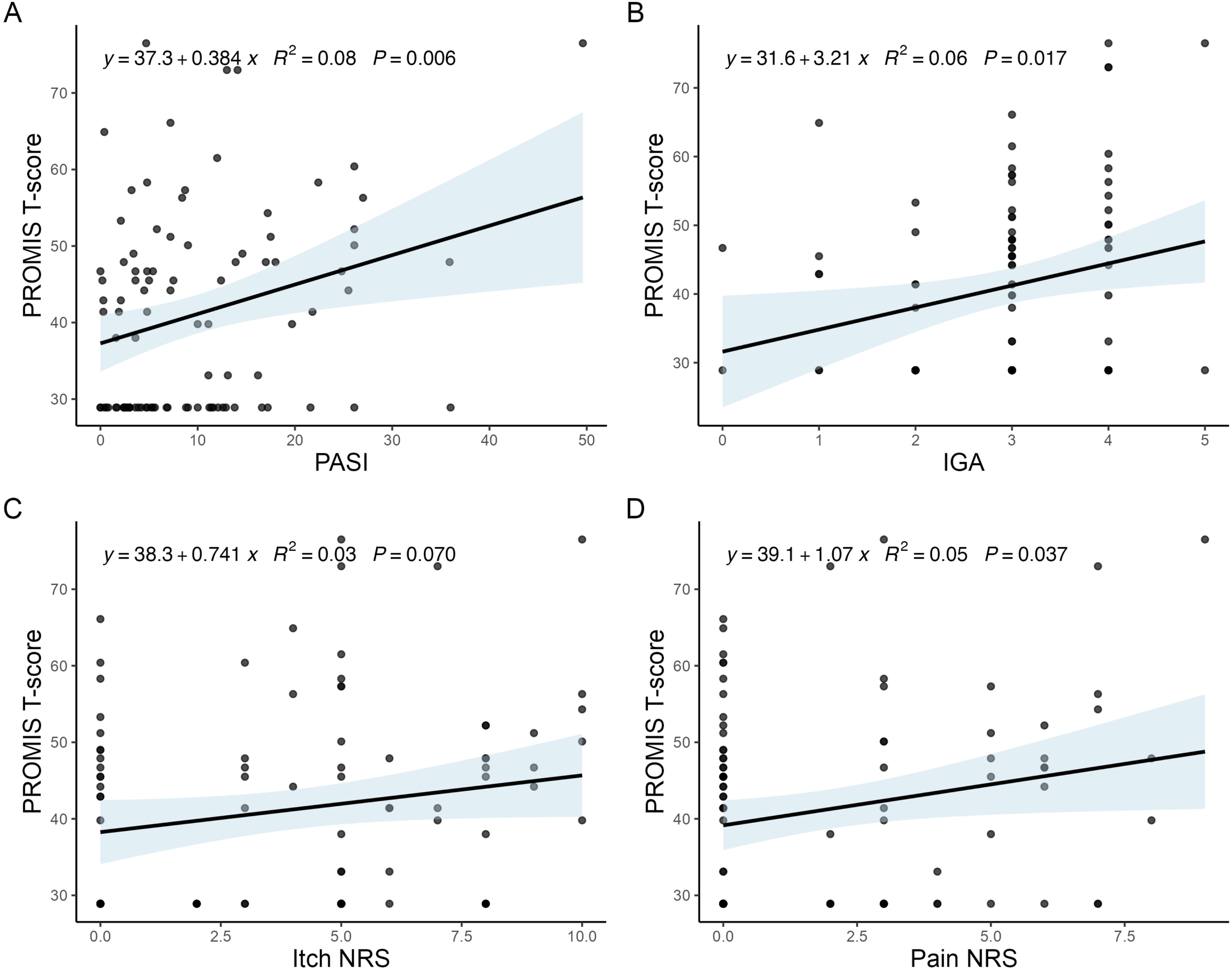
Discussion
This study aimed to examine factors associated with reduced HRQoL and mental health in Kenyan psoriasis patients, a population that remains greatly understudied. Sleep disturbance was consistently associated with worse DLQI, depressive symptoms, and anxiety symptoms in multivariate models, confirming the central role of sleep disturbance as a factor associated with psychosocial burden experienced by Kenyan psoriasis patients. Further analyses to explore the relationship of sleep disturbance with psoriasis disease severity and symptom burden found correlations with PASI, IGA, and pain severity. These results suggest that sleep dysfunction may represent a metric that incorporates aspects of psoriasis severity and pain.
These findings are consistent with prior studies demonstrating that poor sleep is significantly more prevalent in psoriasis patients compared to controls and that sleep impairment, assessed using both objective biometric data as well as patient-reported instruments like the Pittsburgh Sleep Quality Index and newer PROMIS tool, is associated with significantly worse mental health and HRQoL.27-29 Mediation analyses have suggested sleep to be a mediating factor in the causal relationship between psoriasis and psychiatric disorders, accounting for one-third of the association between psoriasis and depression.30,31 It is well established that sleep is critical for normal metabolic, immunologic, and neurological functioning.32,33 In psoriasis, sleep disturbance may exacerbate inflammatory pathways, increase disease activity, and contribute to increased risk of both physical and psychological comorbidities.27,34 Thus, our findings highlight the potential impact of poor sleep on depression, anxiety, and overall QoL in psoriasis patients in Kenya, and suggest that interventions to enhance sleep may be a meaningful and underutilized strategy to improve patient well-being.
Other independent factors associated with negative mental health and QoL in our cohort included younger age (DLQI), itch severity (DLQI), and separated marital status (anxiety and depression). The association between younger age and higher DLQI scores aligns with prior studies conducted in Taiwan and Norway which found that younger patients experience greater psychological distress and lower QoL,35,36 with a prospective cohort study showing that the impact of psoriasis on HRQoL decreases over time, potentially due to improved coping, decreased social rejection, and greater acceptance of the disease. 37 However, other studies in Poland and Italy have found older patients to have worse QoL.38,39 These differences suggest the effect of age on psoriasis-related QoL could thus vary based on country and be influenced by contextual and cultural factors. Itch severity also emerged to have a significant independent association with decreased QoL, consistent with the increasing recognition of pruritus being one of the most prevalent and burdensome symptoms of psoriasis. 40 Prior literature has shown itch severity to correlate strongly with the magnitude of HRQoL,41,42 with itch contributing not only to emotional distress but also to sleep disturbance and disruptions in daily activities and relationships. 43 Given our finding that itch independently associates with DLQI as well as prior studies establishing a link between itch and impaired sleep,27,34,44 these results underscore the reciprocal interaction of pruritus, sleep disturbance, and psychosocial burden in psoriasis, emphasizing the importance of comprehensive management approaches aimed to improve both sleep and itch.
Our finding that separated marital status is associated with greater anxiety and depression should be interpreted with caution, due to the small number of patients who fell into this category (3) and the large confidence interval of the calculated β-coefficient. However, worse body image and reduced self-esteem have been associated with both decreased marital quality and depression in psoriasis patients, consistent with our results. 45
While not reaching statistical significance, involvement of sensitive regions, specifically the soles of the feet and intertriginous areas, showed trends towards association with DLQI. This aligns with a growing body of literature recognizing the impact of specific body sites on QoL and function. In fact, the IPC issued a consensus statement recommending reclassification of psoriasis severity to account for the involvement of high-impact sites such as the face, intertriginous zones, genitals, and soles when considering eligibility for systemic therapy, challenging conventional severity thresholds based on BSA. 46 This consensus was based on multiple studies confirming the disproportionate impact of high-impact sites on HRQoL, even with minimal BSA involvement (≤3%),47,48 and has been increasingly adopted in both clinical trials and real-world practice. 49
There are several limitations to this study. First, part of the data — including patient clinical and treatment history, sleep disturbance, and psychosocial outcomes — relied on participant self-reporting, introducing the potential for recall and reporting bias. For example, the prevalence of many comorbidities in our cohort was lower than expected and less than estimates in the general population, suggesting possible underreporting, which may have influenced our observed relationships. While PHQ-9 and GAD-7 have been validated in Kenyan adult populations,50,51 other instruments used in this study, such as PROMIS and DLQI, have not yet been formally validated in Kenya. The DLQI, however, has demonstrated validity and reliability in other African populations, including Ethiopia and South Africa,52,53 suggesting it is likely culturally adaptable in Kenyan settings, though population-specific validation would increase confidence in our findings. As well, the observational, cross-sectional design of our study limits conclusions about causal relationships between mental health and QoL outcomes and identified associated factors. The small sample size also limits statistical power and precision, reducing the reliability of our estimates and our ability to detect significant associations, particularly for less common factors. The single-center study design limits generalizability to other regions of Kenya. Despite these limitations, this study is one of the first to characterize and explore factors impacting psychosocial burden of psoriasis in Kenya and Africa, contributing to a growing body of literature that explores patient-centered outcomes in diverse global settings and guiding future efforts to improve QoL and mental health outcomes in African psoriasis populations.
Conclusion
In summary, this study identifies sleep disturbance as a key factor associated with reduced QoL, depression, and anxiety among Kenyan psoriasis patients, consistent with prior studies elucidating the mutual and complex interplay of sleep, psoriasis symptoms, and mental health in psoriasis. Additional factors, including younger age, pruritus severity, and separated marital status, were also independently associated with greater psychosocial burden. As such, these findings suggest the multifactorial impact of psoriasis and highlight the need for holistic therapeutic approaches that not only address skin concerns but also incorporate strategies to improve sleep quality and itch symptoms, which should be considered important therapeutic goals and may lead to improvements in overall patient well-being. To our knowledge, this is one of the first studies to examine factors contributing to mental health and QoL in Kenya. Future research with larger, longitudinal cohorts and culturally validated instruments is warranted to confirm these findings, clarify potential causal pathways, and inform contextually relevant care approaches for patients with psoriasis in Kenya and the broader African continent.
Supplemental Material
Supplemental Material - Determinants of Quality of Life and Mental Health in Kenyan Psoriasis Patients: A Cross-Sectional Analysis from the Kenyan Psoriasis Registry
Supplemental Material for Determinants of Quality of Life and Mental Health in Kenyan Psoriasis Patients: A Cross-Sectional Analysis from the Kenyan Psoriasis Registry by Miranda K. Chen, Petronilla Biwott, Isabel Muraguri, Georgia Marquez-Grap, Gian Carlo Baldonado, Payton Smith, Toby Maurer, Tina Bhutani, Samson Kiprono, Wilson Liao in Journal of Psoriasis and Psoriatic Arthritis®.
Supplemental Material
Supplemental Material - Determinants of Quality of Life and Mental Health in Kenyan Psoriasis Patients: A Cross-Sectional Analysis from the Kenyan Psoriasis Registry
Supplemental Material for Determinants of Quality of Life and Mental Health in Kenyan Psoriasis Patients: A Cross-Sectional Analysis from the Kenyan Psoriasis Registry by Miranda K. Chen, Petronilla Biwott, Isabel Muraguri, Georgia Marquez-Grap, Gian Carlo Baldonado, Payton Smith, Toby Maurer, Tina Bhutani, Samson Kiprono, Wilson Liao in Journal of Psoriasis and Psoriatic Arthritis®.
Footnotes
Acknowledgments
The authors thank the research participants of the study.
Ethical Considerations
This observational, cross-sectional, single-center study was approved by the Moi-MTRH Institutional Research and Ethics Committee (Approval number 0004848) and UCSF Institutional Review Board (#24-42250) and was performed in accordance with the Declaration of Helsinki.
Consent to Participate
Written informed consent was obtained by study investigators in either English or Swahili prior to all study activities.
Author Contributions
MKC contributed to statistical analysis and writing the manuscript. PB, IM, and SK contributed to participant recruitment and data collection. GMG, GCB, PS, TM, TB, and SK contributed to study design. WL contributed to study conception, design, and overall supervision. All authors reviewed and approved the final version of the manuscript.
Funding
This work was supported by the National Psoriasis Foundation Discovery Grant.
Declaration of Conflicting Interests
WL has received research grant funding from Amgen, Janssen, Leo, and Regeneron. TB has received research funding from Amgen, Castle, CorEvitas, Novartis, Pfizer, and Regeneron. She has served as an advisor for Abbvie, Apogee, Arcutis, Aslan, Boehringer-Ingelheim, Bristol Myers Squibb, Castle, Dermavant, Galderma, Incyte, Janssen, Leo, Lilly, Oruka, Pfizer, Novartis, Sanofi, Sun, Takeda, Taxa, and UCB. She is a speaker for Abbvie, Amgen, Arcutis, BMS, Dermavant, Galderma, Janssen, Lilly, Leo, Mindera, Ortho, Sanofi, and UCB. MKC, PB, IM, GMG, GCB, PS, TM, and SK report no conflicts of interest in this work.
Data Availability Statement
The data underlying this study will be made available from the corresponding author upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.