
Abstract
Background
Psoriasis is believed to be a common comorbidity of type 2 diabetes mellitus (T2DM). Little is known on the impact psoriasis has on T2DM patients’ disease profiles.
Objective
To assess the impact psoriasis has on T2DM patients’ demographics, comorbidities, and health care outcomes.
Methods
We retrospectively analyzed the 2017 U.S. National Inpatient Sample (NIS) database. We utilized ICD-10 codes to determine T2DM and psoriasis patients along with associated comorbidities. Continuous variables were compared by independent-sample t-tests and categorical variables were compared via Pearson chi-square. All analysis were conducted in IBM SPSS 25.
Results
Among 7,705,988 T2DM admissions, 0.67% of them had comorbid psoriasis. T2DM psoriasis patients (64.38; SD: 12.403) were, on average, younger (64.38 vs 66.73; P < .001) and white (78.7% vs 63.1%; P < .001) and had increased foot ulcers (4.2% vs 3.8%; P < .001), hyperglycemia (22.4% vs 21.0%; P < .001), retinopathy (22.4% vs 21.0%; P < .001), hypercoagulopathy (8.5% vs 6.9%; P < .001), and hypertension (72.5% vs 70.4%; P < .001) than T2DM patients without psoriasis. T2DM psoriasis patients spent more days in the hospital (5.49 vs 5.37; P < .001), had more concurrent diagnoses (19.05 vs 16.5; P < .001), less total charges ($60,596.71 vs $61,534.66; P = 0.010) and had less in-hospital deaths (2.0% vs 2.7%; P < .001) than T2DM patients without psoriasis.
Conclusions
The presence of comorbid psoriasis significantly impacts T2DM patients’ demographics, comorbidities, and health care outcomes. These findings underscore the importance of early disease monitoring, cross-specialty collaboration, and medication monitoring in order to guide individualized management strategies and optimize patient care.
Introduction
Approximately 125 million people have psoriasis worldwide. 1 Psoriasis is an immune-mediated dermatosis characterized by dysregulated keratinocyte proliferation which presents as scattered erythematous plaques with superimposed scale. 2 Psoriasis is believed to be a risk factor for type 2 diabetes mellitus (T2DM), and 11.6% of psoriasis patients have comorbid T2DM. 3 Inflammation and chronic immune stimulation common to both diseases may contribute to diabetes-associated complications in patients with comorbid psoriasis. 4 To assess the impact psoriasis has on T2DM patients’ demographics, comorbidities, and health care outcomes, we conducted a retrospective cross-sectional study using the United States National Inpatient Sample (NIS) database.
Methods
The 2017 United States NIS database was queried using International Classification of Diseases (ICD), 10th Revision codes. ICD-10 codes E11.00-E11.99 were used to identify T2DM patients; patients were grouped based on psoriasis status using ICD-10 codes L40.0-L40.9. Patient demographics, comorbidities, and health outcomes were recorded. Demographic information included age, gender, race, household income, and insurance. Diabetes-related comorbidities included hyperosmolar hyperglycemic state (HHS), ketoacidosis, diabetic nephropathy, diabetic neuropathy, diabetic retinopathy, diabetic angiopathy, foot ulcers, hypoglycemia, hyperglycemia, congestive heart failure (CHF), hypertension (HTN), hypercoagulopathy, and depression and were defined based on their associated ICD-10 codes. Health care outcomes included length of stay (days), total charges (USD), number of total diagnoses, number of total procedures, and mortality.
Demographic factors, diabetic-related comorbidities, and health outcomes were compared between T2DM patients with and without psoriasis. The means of continuous variables were compared via independent-samples t test and categorical variables via Pearson chi-square. For t-tests, the normality of the data was verified and checked using the Shapiro-Wilk test. For the Pearson chi-square tests, all expected cell counts were greater than 5 to meet the test’s assumptions. Furthermore, we applied the False Discovery Rate correction, as proposed by Benjamini and Hochberg, to the P-values obtained from both the t-tests and Pearson chi-square tests. After correction, the significance of our results remained consistent with our initial findings. P-values less than 0.05 were considered statistically significant. Analyses were performed using Statistical Package for the Social Sciences (IBM SPSS 25, Chicago, Illinois).
Results
Univariable Analysis of demographic Variables Based on Diagnosis Status of psoriasis in Type-2 diabetes Mellitus Patients.
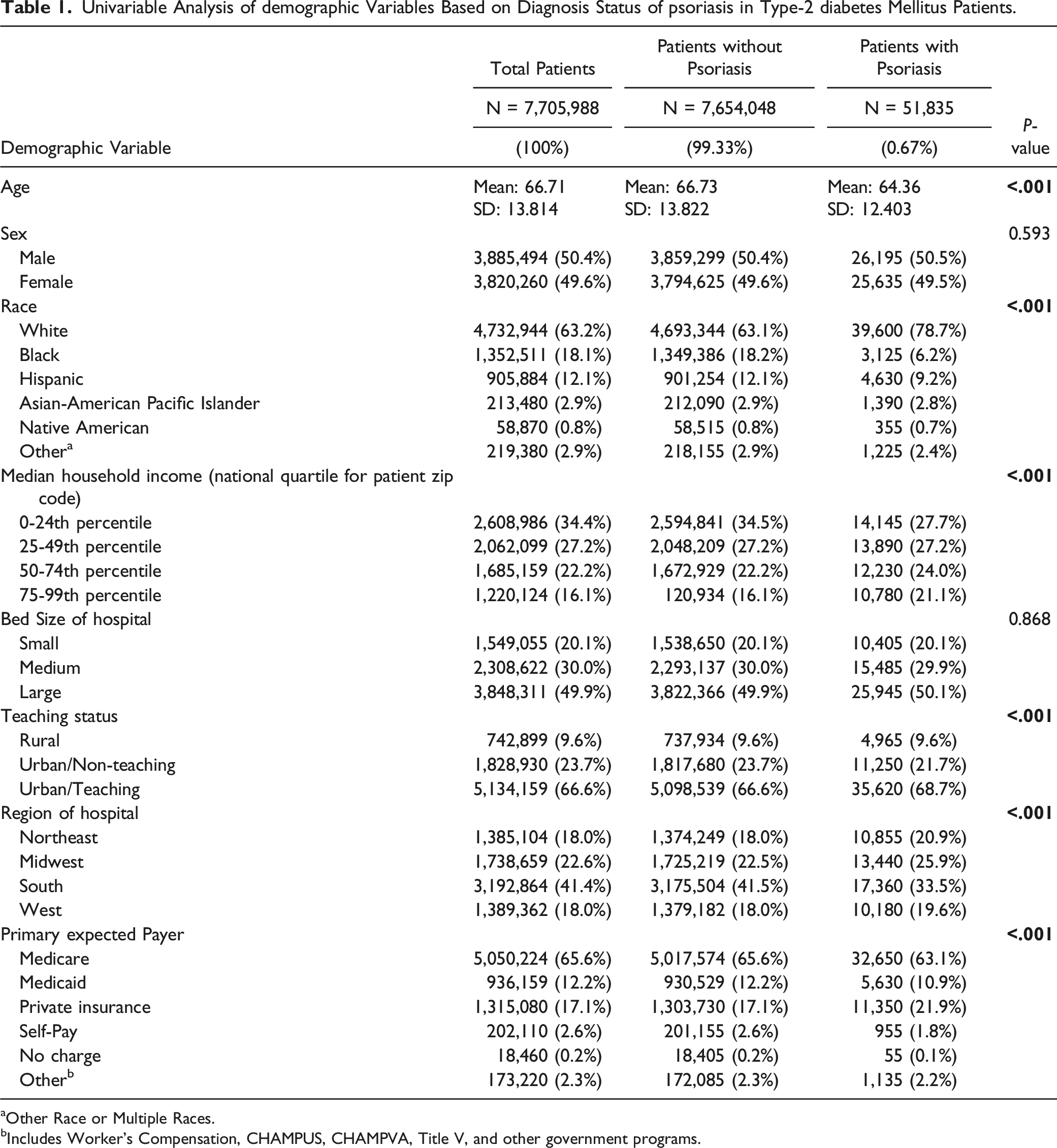
aOther Race or Multiple Races.
bIncludes Worker's Compensation, CHAMPUS, CHAMPVA, Title V, and other government programs.
Demographics
Compared to T2DM patients without psoriasis, T2DM psoriasis patients (64.38; SD: 12.403) were, on average, younger (64.38 vs 66.73; P < .001), white (78.7% vs 63.1%; P < .001), in the 50th-74th percentile (24.0% vs 22.2%; P < .001) or 75th-99th percentile (21.1% vs 16.1%; P < .001) for median household income, in urban teaching hospitals (68.7% vs 66.6%; P < .001) in the northeast (20.9% vs 18.0%; P < .001), midwest (25.9% vs 22.5%; P < .001), and west (19.6% vs 18.0%; P < .001), and had private insurance (21.9% vs 17.1%; P < .001) (Table 1).
Comorbidities
Univariable Analysis of Comorbidities Based on Diagnosis Status of psoriasis in Type-2 diabetes Mellitus Patients.
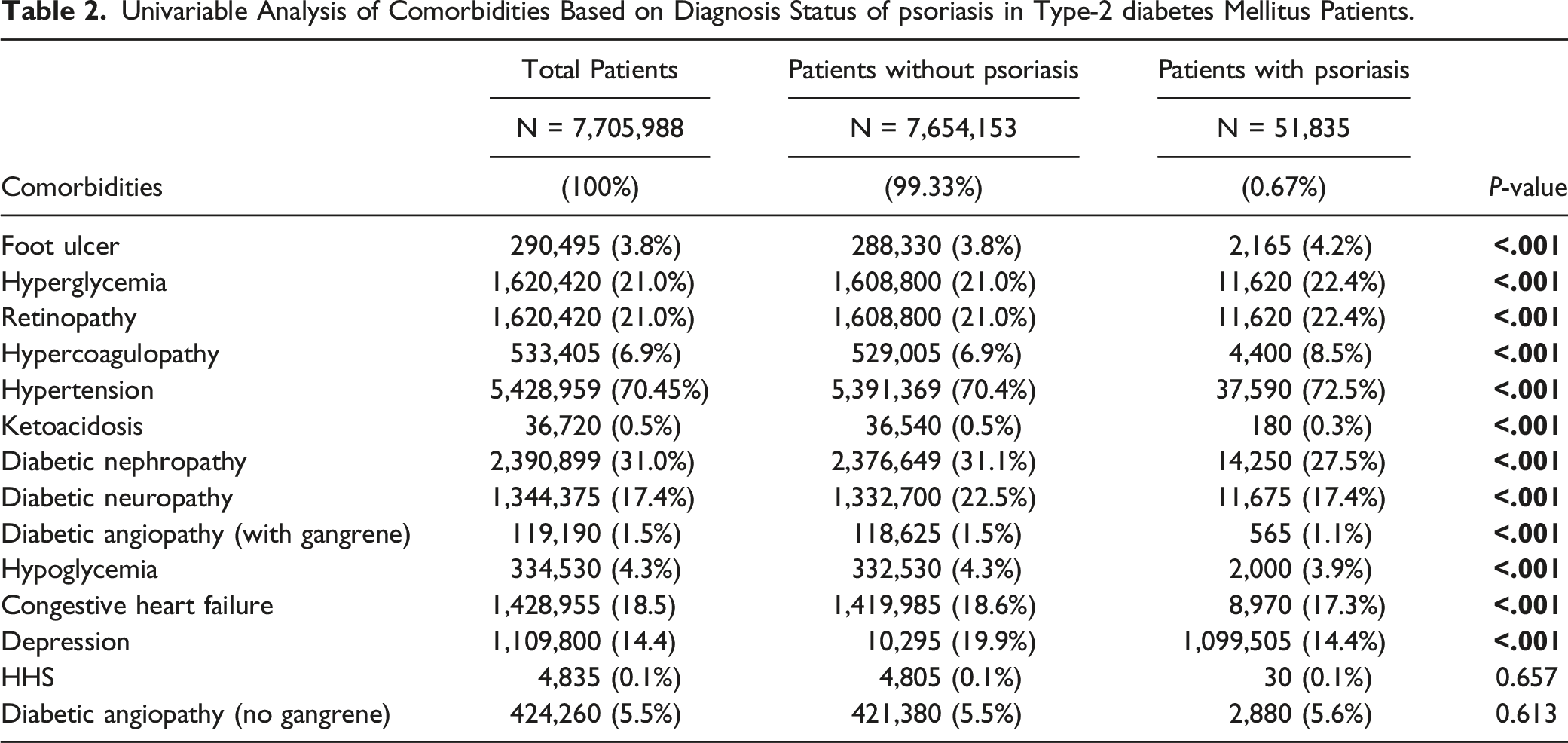
Conversely, T2DM patients with psoriasis had decreased ketoacidosis (0.3% vs 0.5%; P < .001), diabetic nephropathy (27.5% vs 31.1%; P < .001), diabetic neuropathy (17.4% vs 22.5%; P < .001), diabetic angiopathy with gangrene (1.1% vs 1.5%; P < .001), hypoglycemia (3.9% vs 4.3%; P < .001), CHF (17.3% vs 18.6%; P < .001), and depression (14.4% vs 19.9%; P < .001) when compared to T2DM patients without psoriasis. No significant difference was detected between T2DM patients with and without psoriasis for HHS (0.1% vs 0.1%; P = .657) or diabetic angiopathy without gangrene (5.5% vs 5.6%; P = .613) (Table 2).
Health Care Outcomes
Univariable Differences in health care Outcomes Based on Diagnosis Status of psoriasis in Type-2 diabetes Mellitus Patients.
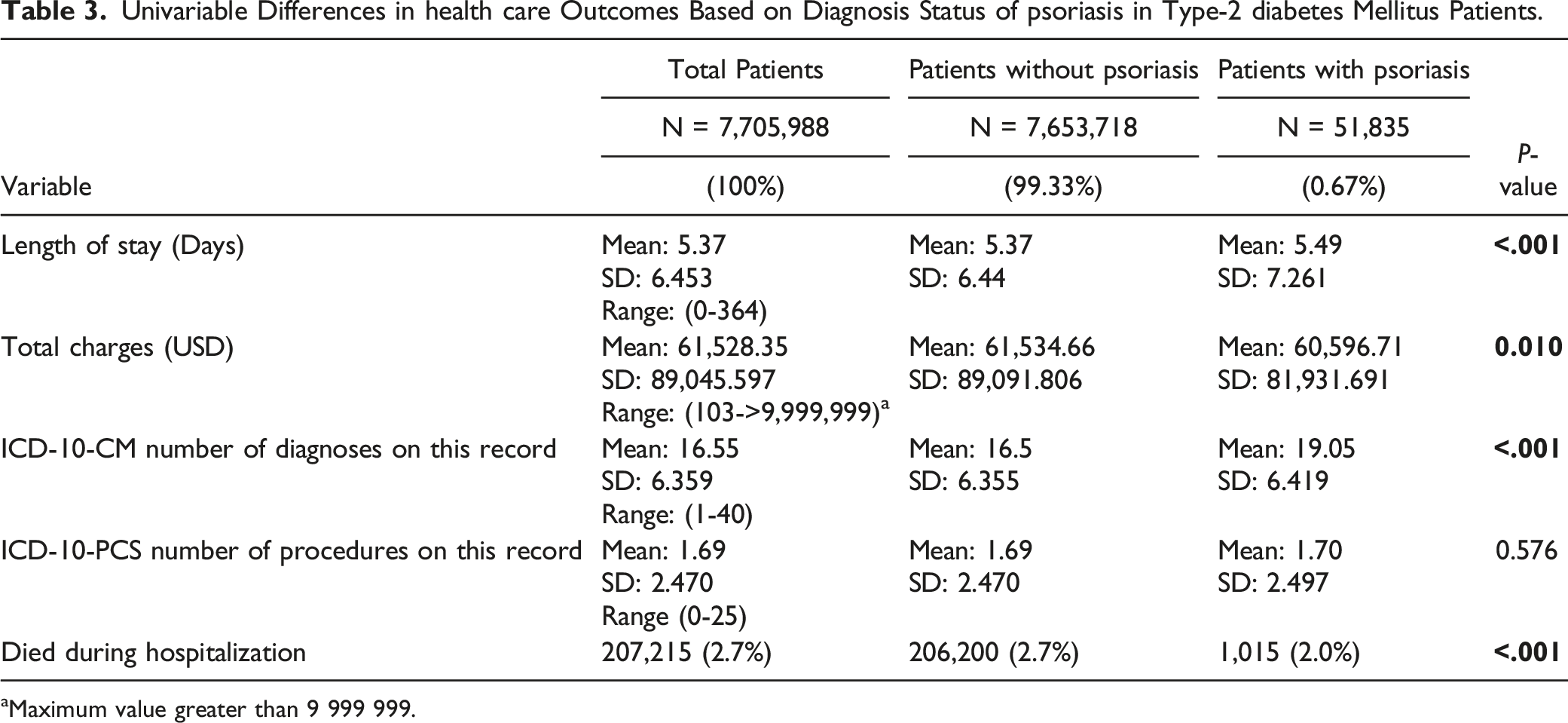
aMaximum value greater than 9 999 999.
Discussion
T2DM patient demographics, diabetic complications, and health care outcomes are impacted by the presence of comorbid psoriasis. T2DM psoriasis patients were typically younger, white, and had increased incidences of foot ulcers, hyperglycemia, retinopathy, hypercoagulopathy, and HTN than T2DM patients without psoriasis. T2DM psoriasis patients also had less deaths, which may be attributed to early disease monitoring and interventions in patients with more than one disease.
The younger overall age observed in T2DM patients with psoriasis could potentially be attributed to the accelerated metabolic dysregulation associated with psoriatic disease. Furthermore, psoriasis has been identified as a significant risk factor for T2DM and younger patients with psoriasis exhibited an augmented risk of developing T2DM. We also determined that more T2DM patients with psoriasis had private insurance and concurrent diagnoses than T2DM patients without psoriasis. It is possible that T2DM patients with psoriasis, due to factors like residing in urban areas and having private insurance, might have better access to health care facilities and thus present earlier to the health care system. As a result of this, we might expect T2DM patients with psoriasis to be younger than T2DM patients without psoriasis. We acknowledge that these interpretations come with certain challenges, such as potential confounding factors like urban vs rural residence and health care accessibility, which might influence our findings. This underscores the necessity for earlier screening and intervention strategies that mitigate the progression of T2DM in this demographic.
The heightened incidence of diabetes-associated complications such as foot ulcers, hyperglycemia, and retinopathy in this cohort can be ascribed to the additive inflammation from psoriasis, which can worsen existing T2DM. Therefore, an integrated care approach becomes vital in this cohort, where stringent psoriasis management synergized with aggressive monitoring of T2DM and diabetic complications.
Interestingly, we noted a lower incidence of depression in the T2DM cohort with psoriasis. This is most likely attributed to more frequent health monitoring due to the presence of a visual disorder in psoriasis, which can make patients feel greater control over their prognosis and reduce associated depression. Furthermore, T2DM patients without psoriasis had significantly more serious diabetes-related complications such as ketoacidosis, diabetic nephropathy, diabetic neuropathy, diabetic angiopathy (with gangrene), and CHF than T2DM patients with psoriasis, which could have exacerbated their depression.
Psoriasis severities and treatments were unavailable and not included in the analysis, which may have impacted patients’ diabetic-related complications and health outcomes. Smoking, alcohol use, obesity, and other lifestyle factors were also not included. In future work, we aim to integrate stepwise logistic regression to sharpen the analysis by controlling confounding variables and better elucidate the predictive role of psoriasis in T2DM patients’ health trajectories. Nonetheless, recognizing the impact psoriasis has on T2DM disease-related complications may be of use to support stringent psoriasis management through increased patient-visits, aggressive medication monitoring, and collaboration across specialties to improve patient care.
Supplemental Material
Supplemental Material - The Influence of Psoriasis on Type 2 Diabetes Mellitus Patient Profiles: A National Inpatient Sample Study
Supplemental Material for The Influence of Psoriasis on Type 2 Diabetes Mellitus Patient Profiles: A National Inpatient Sample Study by Nilesh Kodali, Isabella Blanchard, Keshav D. Kumar, Mallory Zaino, and Steven R. Feldman in Journal of Psoriasis and Psoriatic Arthritis®
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Feldman has received research, speaking and/or consulting support from Eli Lilly and Company, GlaxoSmithKline/Stiefel, AbbVie, Janssen, Alovtech, vTv Therapeutics, Bristol-Myers Squibb, Samsung, Pfizer, Boehringer Ingelheim, Amgen, Dermavant, Arcutis, Novartis, Novan, UCB, Helsinn, Sun Pharma, Almirall, Galderma, Leo Pharma, Mylan, Celgene, Ortho Dermatology, Menlo, Merck & Co, Qurient, Forte, Arena, Biocon, Accordant, Argenx, Sanofi, Regeneron, the National Biological Corporation, Caremark, Teladoc, BMS, Ono, Micreos, Eurofins, Informa, UpToDate and the National Psoriasis Foundation. He is founder and part owner of Causa Research and holds stock in Sensal Health. Kodali, Blanchard, Kumar, and Zaino have no conflicts of interest to disclose.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
CME Credit
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.