
Abstract
Background
Psoriasis is a chronic disease with increased risk of numerous comorbidities. Known differences exist regarding treatment outcomes for psoriasis patients with skin of color (SOC). Factors contributing to these differences are relatively unknown.
Objectives
This study aims to compare the comorbidity burden in SOC psoriasis patients vs White patients, as measured by the Charlson Comorbidity Index (CCI).
Methods
We utilized the National Ambulatory Medical Care Survey (NAMCS) to identify visits for adult psoriasis patients occurring in the years 2002-2016 and 2018. The CCI was used to objectively measure comorbidity burden. Patients were identified by race, and SOC was defined as any reported race besides White Only. A multiple linear regression was run to compare the CCI among adult psoriasis patients based on race and ethnicity, controlling for age, sex, insurance status, and geographic region.
Results
A total of 39, 176, 928 weighted visits were analyzed. Compared to White patients, patients with SOC did not have statistically significant differences in comorbidity burden, as measured by CCI (P = .073 for Black/African American Only vs White Only, P = .073 for American Indian/Alaska Native Only vs White Only, P = .435 for Asian Only vs White Only, P = .403 for Native Hawaiian/Pacific Islander Only vs White Only, P = .195 for Other vs White Only).
Conclusion
Patients with SOC were not found to have differences in comorbidity burden compared to White patients. These results highlight that social factors such as socioeconomic status and access to health care may contribute more directly to psoriasis treatment outcomes than patient race.
Introduction
Psoriasis is a chronic disease that affects patients of various races and skin color.1-3 Known differences exist regarding treatment outcomes for psoriasis patients with skin of color (SOC), with SOC patients reporting increased risk for hospitalization due to psoriasis and greater negative impact on quality of life.4,5 Several possible explanations exist for this phenomenon. First, previous studies have suggested that dermatologists may underestimate the severity of psoriasis in patients with SOC due to differences in their cutaneous presentations compared to those in White patients.
6
For example, psoriasis plaques may be mistaken for post-inflammatory hyperpigmentation on black skin.4-6 Patients with SOC may be underrepresented in clinical trials for psoriasis.4,5,7 Furthermore, differences in socioeconomic status, access to health care
One area that is understudied is the comorbidity burden that psoriasis patients of different races may experience. For example, 20%-30% of patients with psoriasis develop psoriatic arthritis, and some may also develop cardiovascular disease and depression.1,8 However, little is known regarding differences in comorbidity burden based on patient race in psoriasis patients. This subject is important to study because potential differences in comorbidity burden based on race may contribute to patient outcomes. Here, the study aim was to compare the comorbidity burden in psoriasis patients with SOC vs White patients, as measured by the Charlson Comorbidity Index (CCI), to determine whether comorbidity burden differs based on race in psoriasis patients.
Methods
We performed a population-based, cross-sectional study to evaluate the comorbidity burden in psoriasis patients with SOC vs White patients. This study was classified “exempt” by the Institutional Review Board of the University of Southern California because it utilizes publicly available information provided by the Centers for Disease Control and Prevention. We utilized the National Ambulatory Medical Care Survey (NAMCS) to identify visits for adult psoriasis patients (≥18 years old) occurring from the years 2002 to 2016 and 2018. The NAMCS, administered by the Center for Disease Control, provides nationally representative samples of health care visits to physician offices and hospitals across the United States. 9 Physicians were randomly selected and asked to collect information on practice and physician characteristics. 10 The NAMCS utilizes a complex probability survey design with masked weighting variables to estimate a nationally representative sample of patient visits. 9 For each patient visit, the NAMCS queries 3-5 free-entry patient diagnoses. In addition, the NAMCS specifically queries for other common comorbidities including Alzheimer’s disease, COPD, cancer, congestive heart failure, diabetes mellitus, and HIV/AIDS.
For this study, we identified patients with psoriasis by using the International Classification of Diseases, Ninth Revision (ICD-9) code 696.1 and the International Classification of Diseases, Tenth Revision (ICD-10) codes L40.0-L40.9. The CCI was selected as a method to objectively measure comorbidity burden. The CCI is a validated model for quantifying the mortality risk of patients by assigning a numerical score based on the presence or absence of 19 medical conditions. 11 This tool has proven to be useful for a variety of other purposes, including prognosis assessment for research purposes among different individuals with the same medical diagnosis.12,13 Different conditions carry scores of either +1, +2, +3, or +6 if they are present: for example, conditions that are more chronic and less immediately life-threatening such as rheumatologic disease carry a score of +1, while more acute and immediately life-threatening diseases such as metastatic malignancy carry a score of +6. 11 Stepwise increases in CCI are associated with stepwise increases in comorbidities and patient mortality. 13
The CCI was calculated for all outpatient visits for adult psoriasis patients, using previously established comorbidity codes from the ICD-9 and ICD-10. 12 In the NAMCS, adult patients with SOC were identified by their race as either Black/African American Only, Asian Only, Native Hawaiian/Pacific Islander Only, American Indian/Alaska Native Only, Multiracial, or Other. Adult White patients were defined by their race as White Only. A multiple linear regression was run to compare the CCI among adult psoriasis patients based on race and ethnicity, while adjusting for age, sex, geographic region, and insurance type. Sensitivity analyses were also run to evaluate the effect of insurance status on CCI for adult psoriasis patients based on race.
Results
Sociodemographic Characteristics of Psoriasis Patient Visits Between 2002-2016 and 2018 in NAMCS Database.
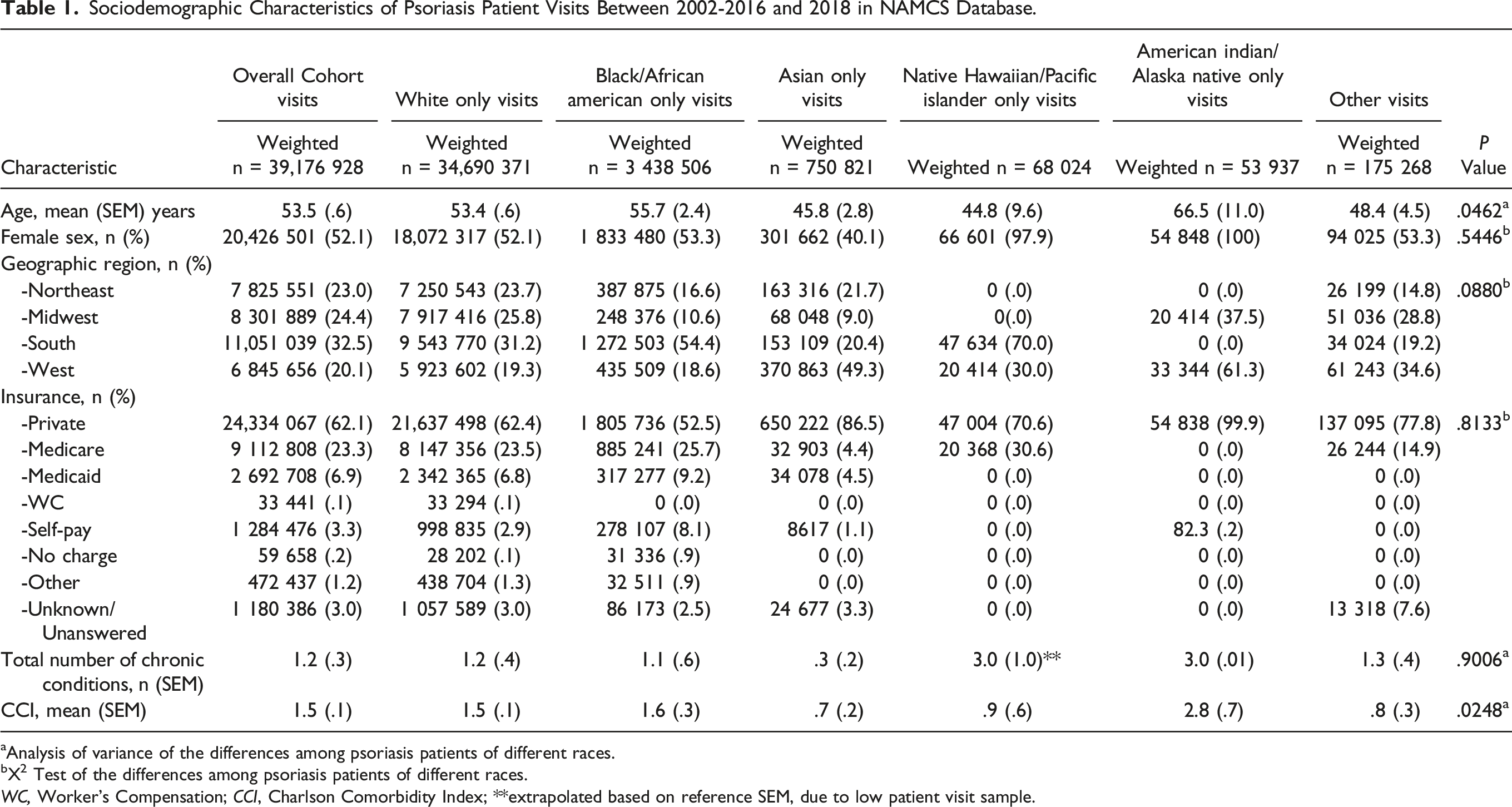
aAnalysis of variance of the differences among psoriasis patients of different races.
bX2 Test of the differences among psoriasis patients of different races.
WC, Worker’s Compensation; CCI, Charlson Comorbidity Index; **extrapolated based on reference SEM, due to low patient visit sample.
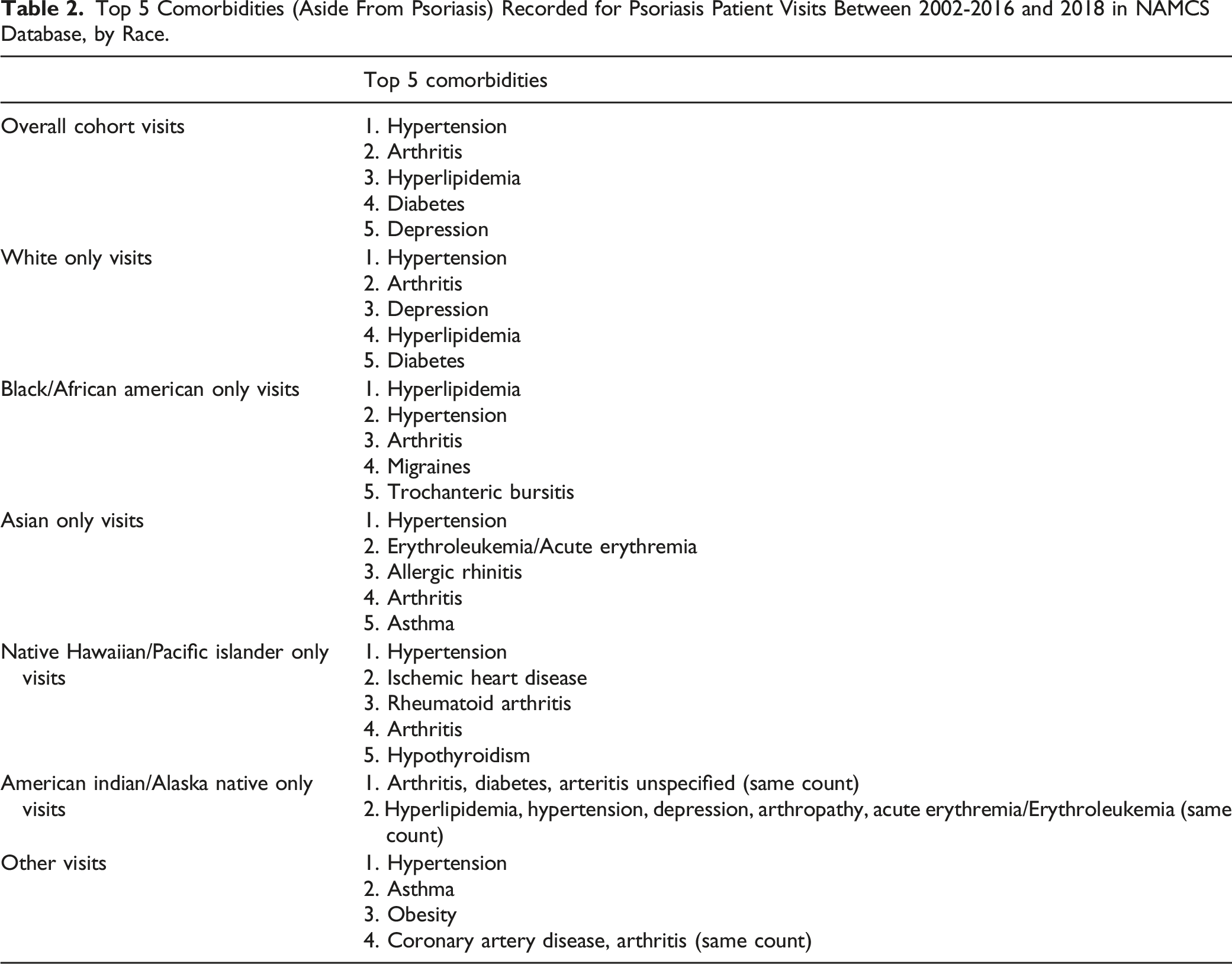
Top 5 Comorbidities (Aside From Psoriasis) Recorded for Psoriasis Patient Visits Between 2002-2016 and 2018 in NAMCS Database, by Race.
Multiple Linear Regression Analysis of Association Between CCI and Race in Psoriasis Patients, Adjusting for Insurance Type.
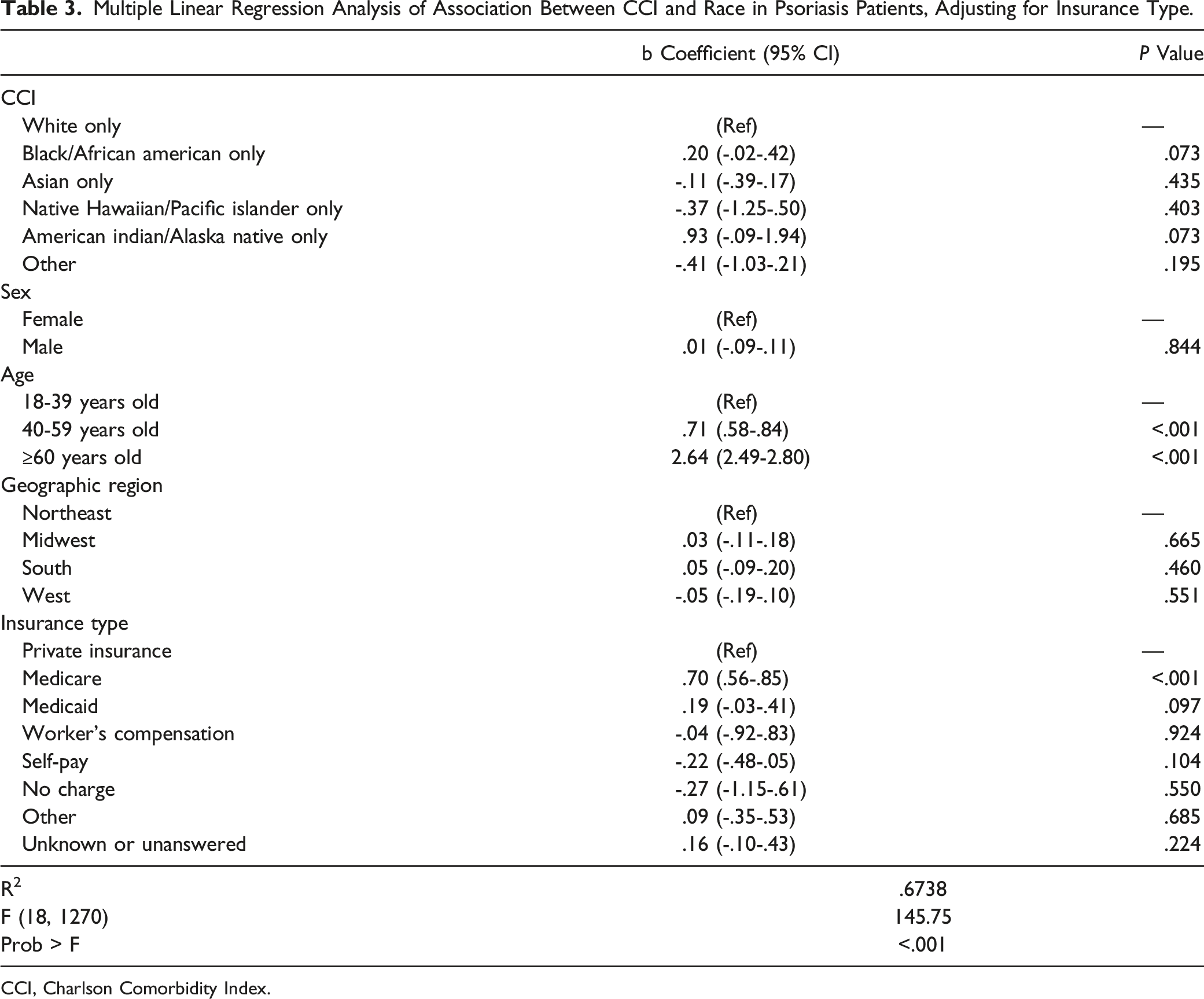
CCI, Charlson Comorbidity Index.
Additionally, we also examined other factors that are associated with comorbidity burden. In this NAMCS study we found that patient visits with an Insurance Type of Medicare were associated with a significantly higher CCI for psoriasis patients than Insurance Type of Private Insurance (P < .001) (Table 3). Also, patient visits with age of 40-59 and age of 60+ were associated with a significantly higher CCI (P < .001 and P < .001, respectively) (Table 3).
Multiple Linear Regression Analysis of Association Between CCI and Race in Psoriasis Patients.
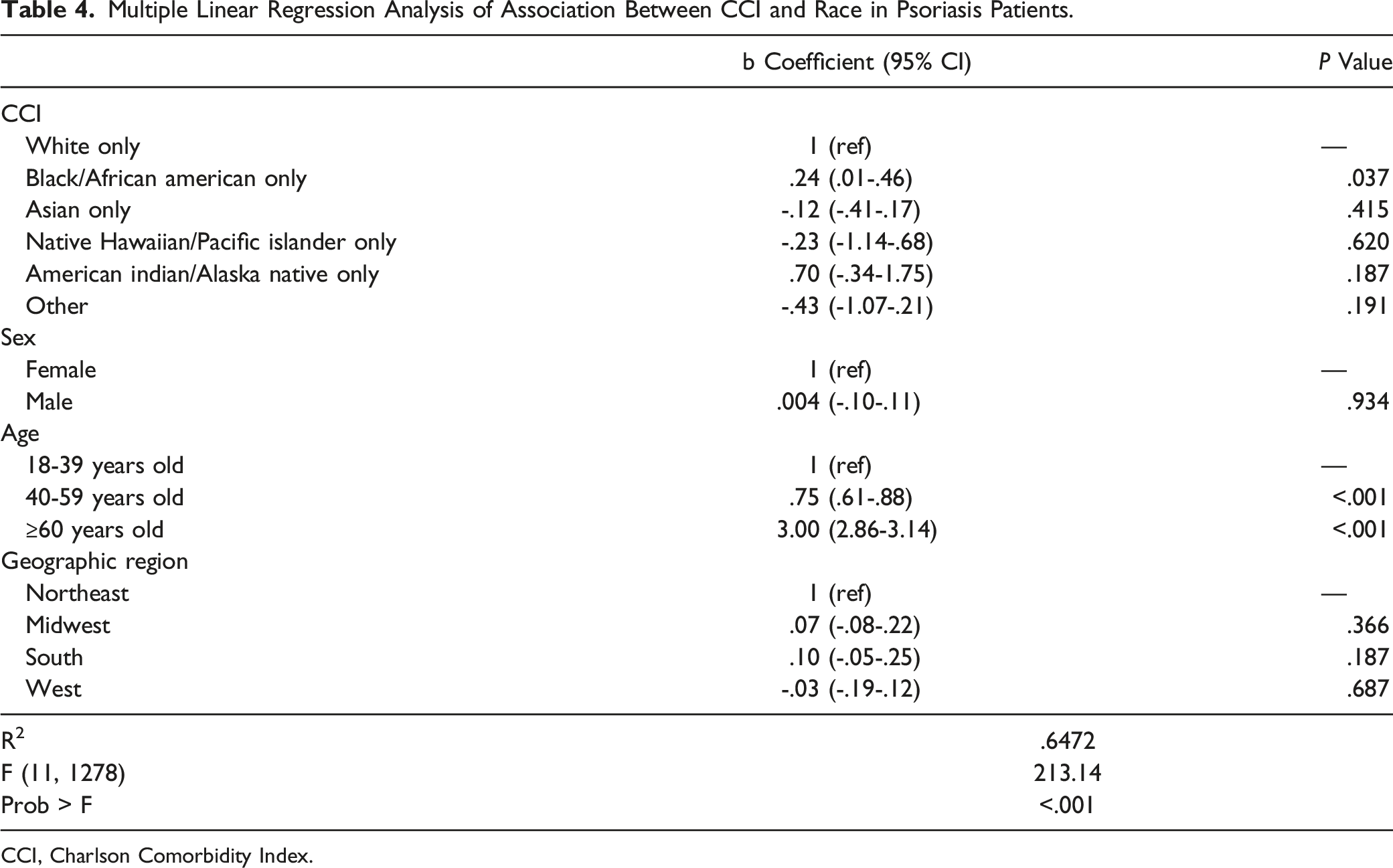
CCI, Charlson Comorbidity Index.
Discussion
Potential differences in comorbidity burden based on race may contribute to differences in psoriasis patient outcomes; this study is among the first to examine the relationship between comorbidities and race in psoriasis patients. Using the NAMCS database, we found no differences in comorbidity burden between psoriasis visits of SOC patients and White patients (Table 3). When insurance is not accounted for, we may see a higher comorbidity burden among Blacks vs Whites (Table 4).
Insurance type has often been used as a proxy for socioeconomic status in a variety of study types, ranging from database studies looking at health outcomes in women with breast cancer to analyses comparing individual clinics in their medication management of coronary artery disease.14-19 Insurance status can be used to estimate socioeconomic status because it reflects patient ability to overcome the financial barriers to health care.16,19 The fact that the significant difference in comorbidity burden between Black/African American Only race and White Only race resolves when controlling for insurance type as a proxy for level of care shows that differences in health outcomes in psoriasis patients with SOC are more likely due to factors external to patient race. These findings align with the previously established consensus that race does not affect health due to biologic differences, but rather because race affects a variety of other social factors that then impact health, such as socioeconomic status.20-25
In our model, we also observed that increasing age correlated with a higher comorbidity burden: patients with an age of 40-59 or 60+ demonstrated a significantly higher comorbidity burden than patients ages 18-39 years old. This may be related to an increased likelihood of developing multiple chronic diseases with increased age, 26 which validates our model.
This study’s findings must be considered within the context of the NAMCS database design. The variables for race are overall established by NAMCS and may not be sufficiently granular for evaluation of racial subgroups. For example, the Asian race encompasses a wide variety of racial subgroups, including South Asians, East Asians, and Southeast Asians. Differences in cultural heritages, values, and lifestyles among these subgroups may affect comorbidity burden. Additionally, most of the weighted patient visits contributing to the NAMCS database were for White patients. Future studies can obtain more data for less represented races as well as specify different subsets of race to obtain a comprehensive understanding of the differences in health status of psoriasis patients of various races in the United States.
Conclusion
In conclusion, psoriasis patients with SOC were not found to have differences in comorbidity burden compared to White patients. These results highlight that race itself is not a central determinant of health status for psoriasis patients in the United States. Rather, social factors such as socioeconomic status and access to health care contribute more directly to health status than patient race.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Authors HP, MYH, KL, PK, DY, EK, and RA have no conflicts of interest to disclose. AWA has served as a research investigator, scientific advisor, and/or speaker to AbbVie, Almirall, Arcutis, ASLAN, Beiersdorf, BI, BMS, EPI, Incyte, Leo, UCB, Janssen, Lilly, Mindera, Nimbus, Novartis, Ortho Dermatologics, Sun, Dermavant, Dermira, Sanofi, Regeneron, and Pfizer.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.