
Abstract
Introduction
Ocular syphilis is a rare but potentially sight-threatening manifestation of syphilis infection caused by Treponema pallidum, with ocular involvement reported in about 6% to 9% of syphilis cases.1–3 Aptly termed “the great masquerader,” ocular syphilis continues to present diagnostic challenges as it mimics a wide range of other infectious and inflammatory conditions. Maintaining a high index of clinical suspicion is essential, as timely diagnosis and appropriate treatment are often curative and may prevent further vision loss and complications. Ocular manifestations of syphilis include posterior uveitis, panuveitis, chorioretinitis, retinal vasculitis, retinal artery or vein occlusion, serous retinal detachment (RD), and, less commonly, necrotizing retinitis.3–5 We report a challenging case of ocular syphilis initially presenting with panuveitis and placoid retinitis with subsequent RD that initially masqueraded as bilateral endogenous endophthalmitis versus acute retinal necrosis (ARN) in a patient with a history of intravenous drug use.
Case Report
A 35-year-old woman presented to the emergency department with a 3-week history of right eye redness, pain, photophobia, decreasing vision, and floaters. She reported no symptoms in the left eye and had no prior ocular history. She had no fever, viral prodrome, or history of uveitis. Her medical history was significant for gonorrhea, hepatitis C infection, and multiple skin and soft tissue infections with associated abscesses, empyema, and pneumonia. Blood cultures obtained 2 years earlier were positive for methicillin-resistant Staphylococcus aureus, for which she refused treatment. She also had a history of polysubstance use disorder, including intravenous drug use and regular inhalational use of high-dose fentanyl.
At presentation, the best-corrected visual acuity (BCVA) was hand motions in the right eye and 20/25 in the left eye. Intraocular pressure was 23 mm Hg OD and 14 mm Hg OS. The right pupil measured 3 mm and was minimally reactive to light, while the left pupil was appropriately reactive. No relative afferent pupillary defect was noted. Anterior examination of the right eye revealed 4+ conjunctival injection and inferior keratic precipitates. The anterior chamber demonstrated 4+ cells and flare, a 0.5 mm hypopyon with dense fibrinoid material, and posterior synechia. There was neovascularization of the iris. There was no view of the posterior segment owing to dense vitritis. Anterior examination of the left eye showed keratic precipitates and 3+ cells in the anterior chamber. Dilated fundus examination of the left eye revealed a mildly hyperemic optic disc. Peripheral retinal whitening was noted in the supratemporal quadrant, accompanied by vitreous opacities, small ghost vessels, and a few dot-blot hemorrhages.
A diagnosis of probable endogenous endophthalmitis versus ARN was made. Urgent right eye diagnostic and therapeutic pars plana vitrectomy (PPV) with anterior chamber washout, along with bilateral intravitreal antibiotic and antiviral injections, was recommended. After discussion of the proposed management plan, the patient left against medical advice. She returned later that night and subsequently consented to surgery.
Intraoperatively, the retina appeared intact. However, a well-defined, non-necrotizing placoid lesion was observed in the supratemporal quadrant, extending from 9 to 12 o’clock and spanning from the periphery to the superior arcade. Retinal whitening was observed along the border of the lesion, without the associated hemorrhage or vascular occlusion typically seen in ARN. There was no retinitis, disruption of the inner retinal surface, or Roth spots. A vitreous biopsy from the right eye was obtained and sent for Gram stain, bacterial and fungal cultures, and polymerase chain reaction (PCR) testing for viral pathogens. The right eye received intravitreal ceftriaxone, vancomycin, and ganciclovir to provide coverage for both endogenous bacterial infection as well as possible viral etiologies, including ARN, given the clinical findings in the left eye. The left eye was injected with intravitreal ceftriaxone and ganciclovir.
Although hospital admission was planned for further diagnostic evaluation and management, the patient left against medical advice after the vitrectomy. She did not return on postoperative day 1 but re-presented the following day. On postoperative day 2, BCVA was hand motions in the right eye and 20/400 in the left eye. Intraocular pressure was 7 mm Hg OD and 14 mm Hg OS. Bilateral keratic precipitates and 2+ anterior chamber cells were noted. There was no view of the posterior segment in the right eye on dilated fundus examination, and no interval changes were noted in the left eye. Vitreous biopsy of the right eye returned negative for varicella-zoster virus (VZV) and herpes simplex virus (HSV). Bacterial and acid-fast bacilli cultures showed no growth. Hospital admission was again strongly recommended, but the patient declined. On postoperative day 5, treponemal chemiluminescent microparticle immunoassay returned reactive, and the rapid plasma reagin test was positive with a titer of 1:32. The patient was referred to the Department of Infectious Diseases; however, she did not attend her initial appointment.
The patient returned 2 weeks postoperatively, reporting a new shadow in her right eye’s vision. BCVA was limited to counting fingers in the right eye and 20/200 in the left eye. Examination of the right eye revealed focal opacification of the lens, and B-scan ultrasonography demonstrated a macula-off RD (Figure 1). She subsequently underwent a 25-gauge PPV with silicone oil tamponade, endolaser photocoagulation, and cataract extraction with intraocular lens insertion. Intraoperatively, the retina was noted to be highly mobile, with flocculent material suggestive of necrotic retina and several breaks within areas of necrosis.
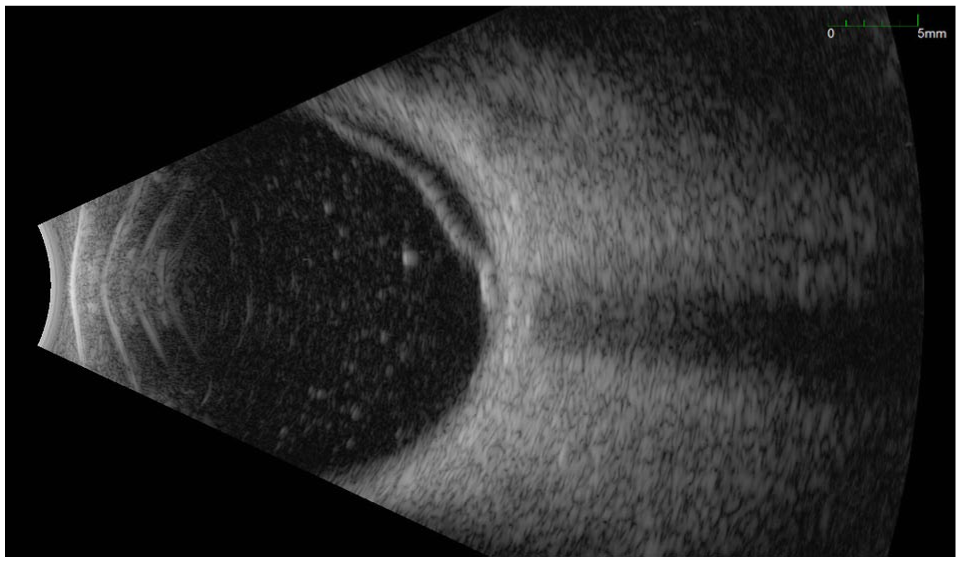
B-scan ultrasonography of the right eye demonstrates a macula-off retinal detachment with associated dense vitritis.
Another appointment with the Department of Infectious Diseases was arranged, and the patient was prescribed 3 weekly doses of 2.4 million units of intramuscular benzathine penicillin G for syphilis. A course of intravenous vancomycin was recommended; however, given concerns regarding the feasibility of prolonged intravenous therapy, oral doxycycline was also prescribed for methicillin-resistant S. aureus (the patient reported an allergy to trimethoprim-sulfamethoxazole [Bactrim]). The Department of Infectious Diseases also arranged for a lumbar puncture to evaluate for neurosyphilis, but the patient did not attend the appointment. She had no fixed address, and despite repeated efforts by the public health unit’s community outreach team, she could not be located to complete the treatment or follow-up.
Conclusions
As the global incidence of syphilis continues to increase worldwide, eye care providers are increasingly likely to encounter ocular syphilis as a cause of ocular inflammation.6,7 Its presentation lacks uniformity, encompasses a wide variety of clinical manifestations and symptoms, and frequently mimics other infections and inflammatory conditions, thereby creating a diagnostic dilemma.8,9 This variability in presentation underscores the importance of maintaining a high index of suspicion for ocular syphilis, particularly in high-risk populations.
In our case, the presence of localized peripheral whitening of the retina with occluded arterioles raised concern for ARN. 10 ARN is more likely to affect the peripheral retina first, as observed in this patient, whereas syphilitic retinitis often starts at the posterior pole. 10 Additionally, the severe anterior inflammation with hypopyon was unusual for syphilis. 11 Several reports have highlighted the diagnostic challenges in differentiating ARN from syphilitic retinitis.12–14 In cases of diagnostic uncertainty, an aqueous diagnostic tap may be obtained and stored for PCR testing for HSV, VZV, and cytomegalovirus until syphilis serologic results. 10 If syphilis serology is negative, these results may help guide antiviral therapy. However, longer laboratory turnaround times in some healthcare settings may delay appropriate treatment. Empiric treatment is therefore often warranted in progressive and vision-threatening infections. 10 Given the concern for severe and rapidly progressive ARN in this patient, both eyes were injected with intravitreal ganciclovir to provide coverage against herpes viruses typically associated with ARN, such as HSV and VZV.8,10,15,16
Accurate diagnosis is important, as it guides different management approaches. For example, if ARN is suspected, treatment may include antiviral and/or steroid therapy, often without appropriate antibacterial coverage. In previous reports, misdiagnosis of syphilitic uveitis as ARN and subsequent treatment with steroids led to complete vision loss in the affected eyes.13,14 The recommended treatment for ocular syphilis is identical to that for neurosyphilis: intravenous aqueous crystalline penicillin G, 18 to 24 million units daily, administered for 10 to 14 days.17–19 However, in this case, the Department of Infectious Diseases team prescribed 3 weekly doses of intramuscular benzathine penicillin G, given the high likelihood of nonadherence to a prolonged course of intravenous antibiotics.
The patient’s fentanyl use, history of intravenous drug use, and untreated methicillin-resistant S. aureus infection further raised concern for endogenous bacterial endophthalmitis. To provide broad antimicrobial coverage, she received intravitreal ceftriaxone and vancomycin, as well as intravenous vancomycin and oral doxycycline. At the end of her initial assessment, she disclosed that she was recently treated for gonorrhea. Given the high co-infection rates among sexually transmitted diseases, this disclosure greatly increased our suspicion of syphilis. 20 Previously published cases have highlighted frequent co-infection between syphilis and other sexually transmitted diseases. A particularly strong association exists with HIV infection, with studies reporting 40% to 50% of ocular syphilis cases in HIV-positive patients.2,18,21 –23 Some researchers have suggested that HIV co-infection may lead to more severe ocular manifestations and more frequent posterior segment involvement. 24 In this case, the patient had previously tested negative for HIV. Other infectious masqueraders, such as tuberculosis and toxoplasmosis, may also present as necrotizing retinitis and should be considered in the differential diagnosis.
Exudative RD is an uncommon manifestation of ocular syphilis. Jumper et al 25 described 3 cases of exudative RDs and retinal infiltrates associated with syphilis. In 2 cases, the subretinal fluid (SRF) resolved with intravenous penicillin alone. In a third case involving a total RD, the SRF did not resolve until adjunctive treatment with oral steroids and a posterior sub-Tenon injection was administered. More recently, Shughoury et al 26 described a series of 23 cases of syphilitic rhegmatogenous RDs. Only 2 eyes had an RD at the time of presentation, with the remainder developing an RD at a median of 4 weeks after initiation of therapy (range, 1–41 weeks). Our patient was found to have an RD 2 weeks after presentation, corresponding to at least 5 weeks since symptom onset. The detachments in the case series had severe features, with 10 classified as total or subtotal RDs. Retinal breaks were often found in areas of previous retinitis. Proliferative vitreoretinopathy (PVR) was present in 70% of cases at the time of diagnosis, and some eyes demonstrated combined tractional and rhegmatogenous RDs.
Surgical repair was performed with PPV and scleral buckle in 12 cases and scleral buckle alone in 2 cases. Silicone oil (n = 12) or perfluoropropane (C3F8; n = 3) was used for tamponade; recurrence occurred in 25% of silicone oil cases and in all cases treated with C3F8. Final visual outcomes were guarded, with 50/5 of eyes achieving 20/200 or worse, highlighting the challenges of managing these RDs. Notably, our patient did not demonstrate PVR or significant traction and was managed with vitrectomy, silicone oil tamponade, and 360-degree laser barricade. Given the potential for delayed development of retinal tears and detachment, patients with syphilitic uveitis may benefit from closer monitoring. Although the small number of reported cases restricts definitive conclusions, consideration of prophylactic laser, silicone oil tamponade, or early vitrectomy may be warranted in selected high-risk cases.15,26
The diagnosis of syphilis is based on clinical history, examination findings, and serologic testing, including both non-treponemal and treponemal assays.27–29 While serologic testing remains the primary diagnostic tool, cases of seronegative ocular syphilis have been reported, particularly in patients co-infected with HIV and in early stages of infection. 30 This emphasizes the need for comprehensive ophthalmological examination and sound clinical judgment when suspicion remains high despite negative serologic results. Although syphilis is a curable condition, poor visual outcomes are still possible. Unfortunately, our patient presented for medical attention at least 3 weeks after symptom onset. During this time, she developed severe panuveitis and significant vision loss, further complicating the diagnostic picture. Additionally, owing to laboratory turnaround times, treatment for syphilis was not initiated immediately. A retrospective study demonstrated that lower VA at diagnosis and treatment delays of more than 12 weeks were associated with poorer VA at 6-month follow-up. 31 Similarly, a case series of 6 patients described 2 cases of permanent blindness attributable to delayed treatment. 32
Numerous factors were likely at play in our patient’s delayed presentation and subsequent poor visual outcome. She had no fixed address and no reliable means of communication, significantly limiting continuity of care. Individuals who are under-housed or homeless are at a particularly increased risk for syphilis, and clinicians should maintain a high index of suspicion in these vulnerable populations. Unfortunately, these individuals are also less likely to seek or continue medical care.33,34 A recent study in Ontario, Canada, found a high prevalence of undiagnosed ocular pathology in homeless adults, with 15% having non-refractive ocular abnormalities on examination and 8% requiring urgent ophthalmology referral. 35 Significant barriers, such as a lack of access to transportation, competing priorities such as housing and food insecurity, and fear of stigma, may further prevent patients from seeking care. 34
In this case, adherence to treatment recommendations was also challenging, and the close follow-up typically required to prevent vision loss was not possible.
In conclusion, ocular syphilis remains a diagnostic challenge owing to its highly variable presentations. Although it is a treatable disease, delayed presentation or misdiagnosis may result in poor visual outcomes. Eye care providers must maintain a high index of suspicion for syphilis as a cause of intraocular inflammation, even in atypical presentations, especially given the increasing incidence of the disease.
Footnotes
Acknowledgements
None.
Ethical Approval
Ethical approval was not required for the current study as it is a case report.
Statement of Informed Consent
Informed consent was not obtained because no patient identifiers were included.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Data Availability
Data are shared throughout the main body of this case report.