
Abstract
Keywords
Introduction
The evolution of viewing systems in vitreoretinal surgery has progressed from traditional handheld planoconcave lenses to contemporary wide-angle viewing systems. These wide-angle systems provide a detailed, panoramic intraoperative view of the retina even in the presence of small pupils, intraocular lenses, or keratoprostheses. This technologic innovation has significantly enhanced the efficiency and success rates of complex vitreoretinal procedures.
Currently, 2 primary types of wide-angle viewing systems are in use: noncontact and contact. 1 Noncontact systems offer several advantages, including the elimination of intraoperative corneal trauma, independence from a skilled surgical assistant, and improved visualization during air–fluid exchange or in patients with steep corneas. A key disadvantage of this approach is the risk of condensation forming on the undersurface of the lens as it approaches the cornea, in addition to the need for continuous application of viscoelastic material to prevent corneal desiccation.
Contact systems deliver a wider field of view, superior image resolution, and stereopsis by mitigating natural corneal aberrations and minimizing the number of reflective surfaces. 2 Despite these advantages, limitations include reliance on a skilled assistant for lens positioning, time lost during manual adjustment of the microscope head when switching fields, and crowding of the operative field in complex bimanual surgeries, particularly when additional assistants are needed to manage the lens and chandelier light.
A hybrid viewing system that integrates the advantages of both noncontact and contact systems can provide surgeons with enhanced flexibility when managing complex vitreoretinal cases. To our knowledge, only 2 reports have described an approach integrating both types of visualization, but the adoption of a hybrid system has been limited, possibly due to high costs or insufficient technical details.2,3
The Resight 700 Fundus Viewing System (Carl Zeiss Meditec AG) is a noncontact wide-angle viewing system that incorporates a focusing device positioned between the microscope and the lens. The distance between the focusing device and the wide-angle lens is fixed and the lens mounted on a spring-loaded arm. The focusing device can be operated via a foot pedal, a feature that has made it the most widely used inverter in clinical practice. 3
In this report, we describe a simple, inexpensive, 3D-printed holder for a high-resolution, wide-angle contact lens compatible with the Resight 700 system. This adapter allows for seamless transition between noncontact and contact viewing during surgery and obviates the need for surgical assistants.
Methods
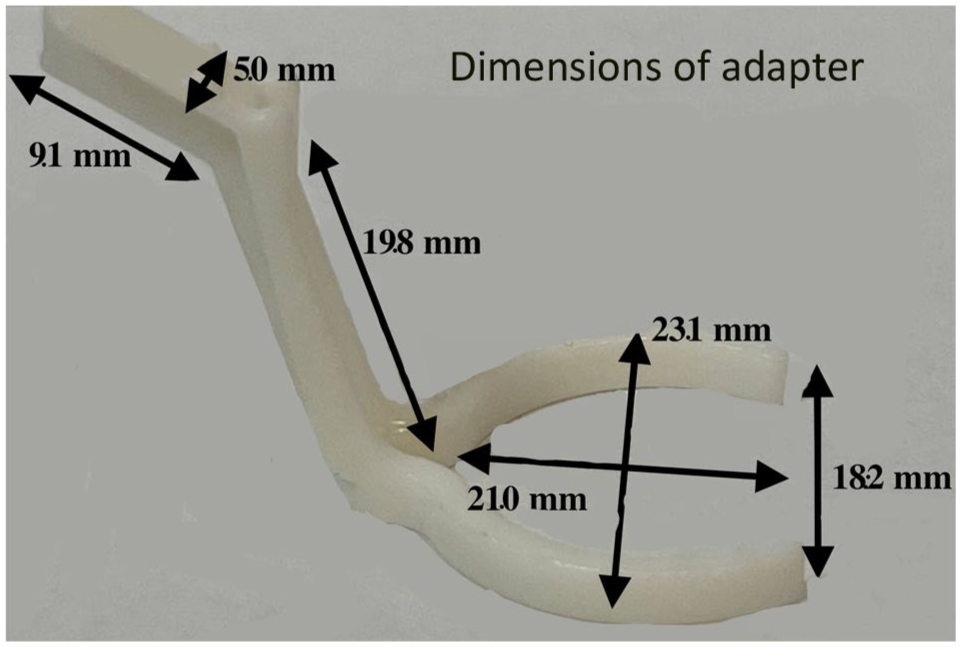
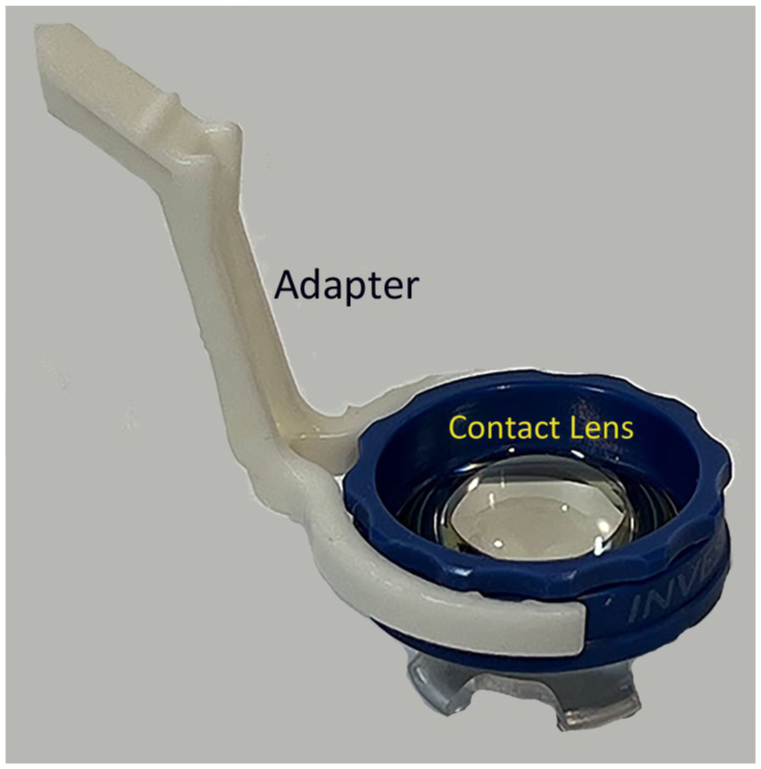
The 3D-printed adapter for the Resight 700 system consists of 2 components: an adaptive lens holder and a widefield contact lens (Figure 1). The lens holder measures 23 mm in width, 45 mm in length, and 18 mm in height, with arms designed to encircle lenses ranging from 20 mm to 22 mm in diameter (Figure 2). The lens holder was printed using a Sprint Ray Pro95s printer with sprint ray study model white 2 resin (chosen for its nonporous, sterilizable, and smooth surface finish). Postprocessing included a 2-stage wash in 99% isopropyl alcohol, followed by postcuring for 30 minutes in the Sprint Ray ProCure 1 unit at preset conditions of 50°C (122°F). The resin, with a flashpoint of 93.3°C (200°F), provides sufficient strength to firmly secure the lens in place while maintaining enough flexibility to accommodate slight variations in lens size without fracturing. Alternatively, the lens holder could be fabricated from ultraviolet light–resistant, cost-effective plastics, such as acrylonitrile butadiene styrene, polypropylene, or high-density polyethylene, which offer higher flexural strength and greater heat tolerance. The lens holder can be resterilized and reused in surgical procedures multiple times as needed.
The widefield contact lens is attached to the distal end of the adaptive lens holder. The proximal end is attached to the flexible rotating arm of the Resight system.
The dimensions of the lens holder are customized to provide secure attachment of the lens and to the viewing system, allowing sufficient flexibility for use.
A miniaturized aspheric wide-angle contact pan fundoscopic lens with 4 footplates (HRX SSV, Volk Optical) is the second component of the hybrid system. 4 The lens, along with an adaptive lens holder, is inserted into the flexible arm of the lens-positioning unit. The lens-positioning unit provides a 170-degree static field of view in phakic eyes and a 180-degree dynamic view (ora to ora). Once assembled, the Resight system is controlled in the standard fashion via the foot pedal joystick and buttons, allowing micro-adjustments in the x-, y-, and z-axes, as well as magnification and fine focus to optimize visualization of the posterior pole during surgery. This system can be interchanged with a noncontact system as needed, depending on the circumstances and surgical requirements.
Results
The proximal end of the lens adapter is designed to fit the Resight 700, replacing the standard green lens holder. The contact lens is inserted into the distal circular end of the adapter, ensuring precise alignment with the microscope’s visual axis (Figures 3 and 4). The patient’s head should be positioned such that the iris surface is aligned parallel to the microscope objective to optimize the system’s performance. A cohesive viscoelastic is applied to the corneal surface as a coupling agent, and the microscope is lowered to dock the lens into position. A change in the viscoelastic meniscus signals the onset of a clear fundus view. A prism set incorporated within the microscope allows reinversion of the image, providing a true erect stereoscopic fundus view in the standard manner. 5 The single viscoelastic application creates a stable negative suction between the contact lens and the cornea, eliminating the need for repeated administration during surgery.
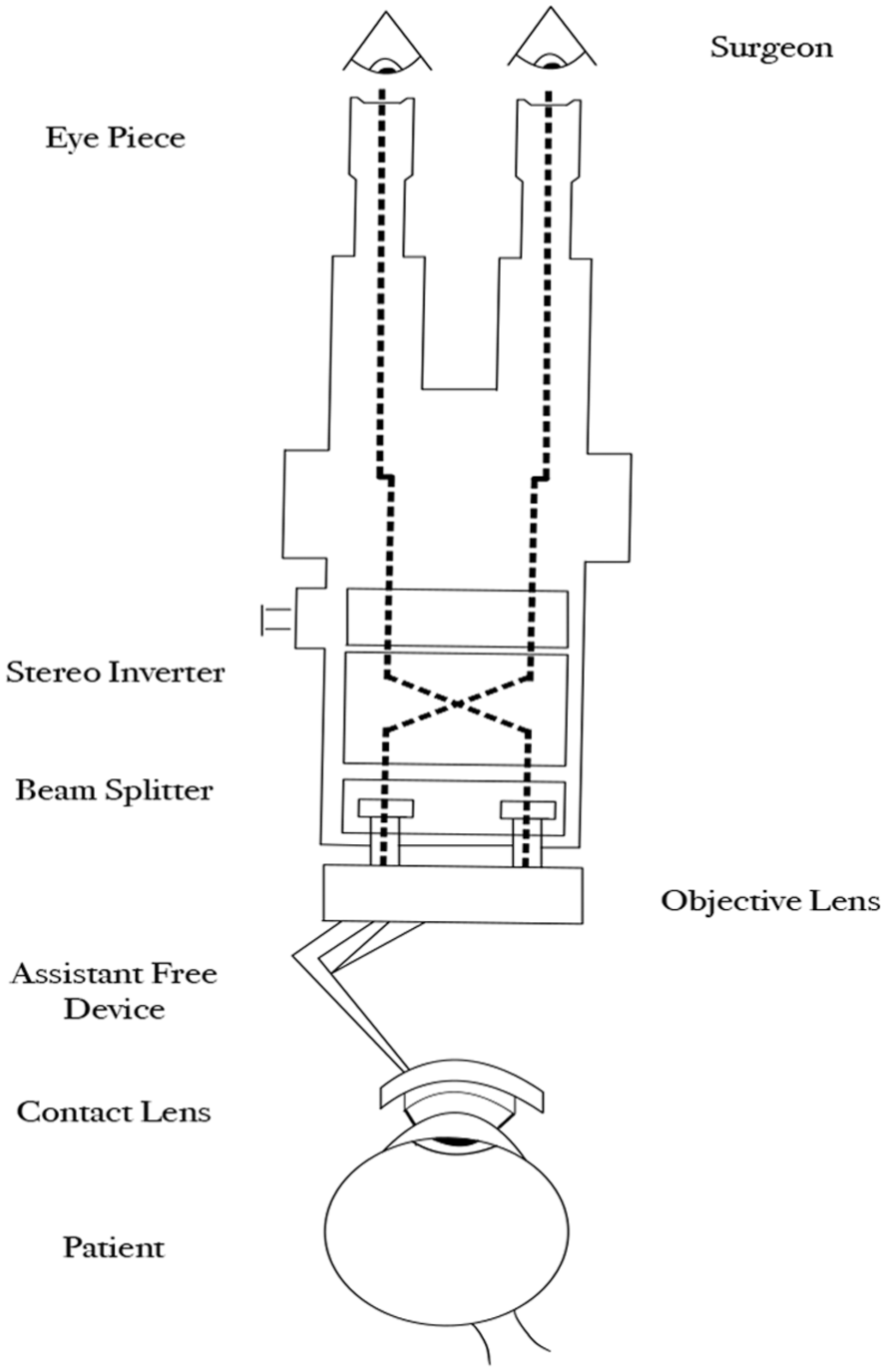
Schematic diagram of the surgical viewing system, including the widefield contact lens.
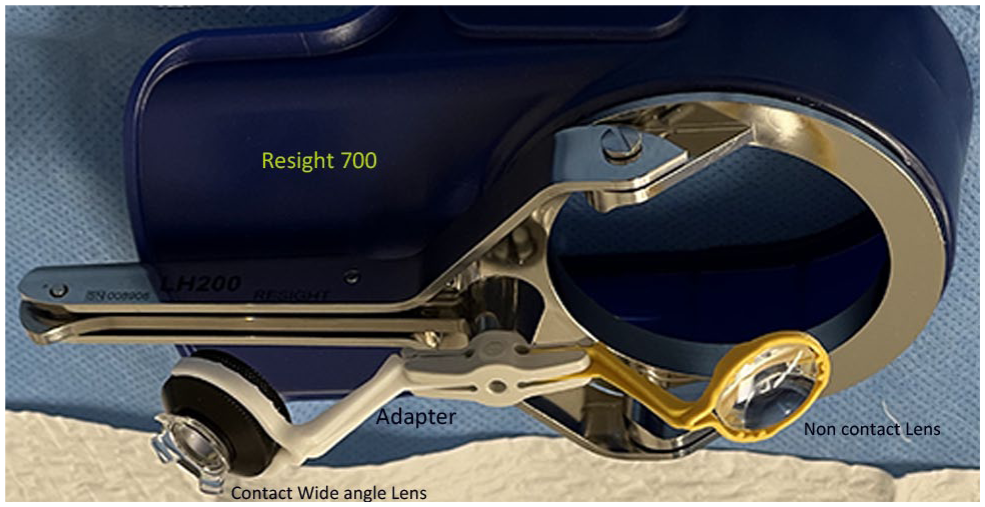
Resight system with adapters for contact as well as noncontact systems in place.
Foot plates, which are specialized extensions at the base of surgical contact lenses, enhance the stability of negative suction during ocular surgery by increasing the contact surface area between the lens and the cornea, thereby distributing suction forces more evenly and reducing the risk of localized pressure points that could lead to suction loss. This broader base also helps form a more effective seal at the interface, minimizing the possibility of air leaks or lens displacement during surgical manipulation. As a result, the lens remains stabilized and micro-movements are prevented, which maintains the negative pressure established by the initial viscoelastic application and reduces the need for repeated administration of viscoelastic material throughout the procedure. The improved retention of negative suction minimizes surgical interruptions and protects corneal integrity by reducing the risk of trauma or epithelial disruption, ultimately contributing to more efficient and safer surgical outcomes. The lens system can then be used conventionally to perform retinal surgery, with the microscope’s foot pedal controlling magnification and movement (Figure 5).
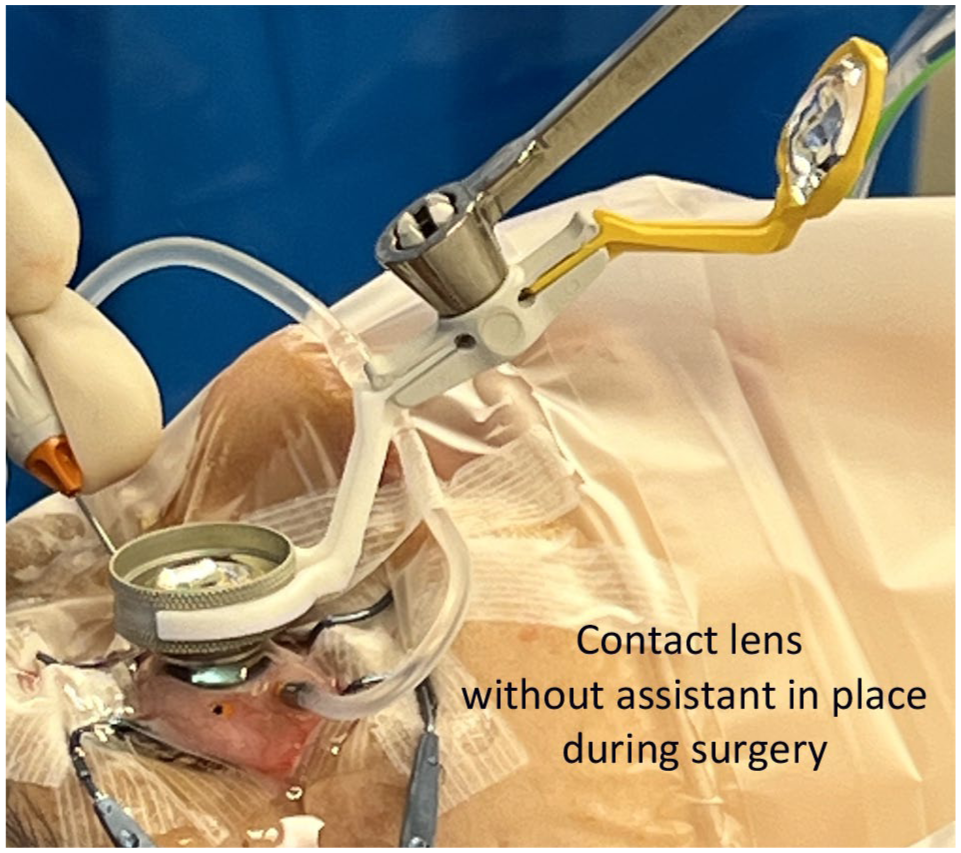
Contact lens with adapter, without an assistant in place during surgery.
Conclusions
The wide-angle viewing system has addressed many challenges encountered in vitreoretinal surgery by providing a panoramic, high-clarity view of the fundus. 6 The noncontact system incorporates indirect ophthalmoscopy within the operating microscope, whereas the contact system uses a miniaturized aspheric contact pan fundoscopic lens to achieve wide-angle fundus observation during vitreous surgery. Both systems require stereoscopic inversion of images, accomplished via a prism set housed within a lightweight, airtight container integrated into or positioned on the microscope.
The noncontact wide-angle viewing system offers the advantage of a skilled surgical assistant not being required to hold a viewing contact lens. However, image resolution and stereopsis are inferior to those of the contact system when assessing the peripheral retina due to spherical aberrations, image distortion, edge blurring, and fogging of the lens. 7 Conversely, the contact system minimizes corneal aberrations and reduces the number of reflective surfaces, thereby improving image quality. Nonetheless, maintaining precise X-Y-Z positioning during tilting maneuvers may prove challenging, potentially compromising image stability and accuracy in complex surgical procedures, particularly when the peripheral retina is involved. It is therefore imperative to adjust the head of the operating table before surgery, ensuring that the patient’s corneal plane remains parallel to the floor. 8
To combine the benefits of both systems, a 3D-printed adapter for the Resight system has been developed that allows for high-quality imaging using the contact system without the need for a skilled assistant and enables a seamless switch to noncontact mode when corneal distortion occurs with the contact lens. The 3D-printed adapter has been used in more than 500 cases of complex vitreoretinal surgery, including severe proliferative diabetic retinopathy with tractional retinal detachment and advanced proliferative vitreoretinopathy. It stabilizes and anchors the surgical lens on the patient’s corneal surface, eliminating the need for an assistant during vitreoretinal procedures. The newer design of the contact wide-angle system, which provides a 130-degree field of view, is compact and does not interfere with vitrectomy instruments (Supplemental Video 1). Throughout the surgical procedures, the fundus image demonstrated excellent clarity and field of view. The accessibility of the desired field of view during vitrectomy contributed to a reduction in surgical time. Notably, there was no compromise to the corneal surface.
In summary, we present the technical details of a 3D-printed adapter for the Resight system that effectively supports both noncontact and contact modes, ensures optimal performance, and allows customization to meet the specific requirements of each case, regardless of lens type, without the need for a skilled assistant.
Footnotes
Acknowledgements
We thank Mr. Seth Myhre for technical assistance in printing the adapter and Mr. Parsa Riazi for help with illustration.
Authors’ Note
Podium presentation at the 2024 American Society of Retina Specialists Annual Meeting, Stockholm, Sweden.
Ethical Approval
The study was conducted in accordance with the Declaration of Helsinki, and informed consent was obtained from the participant (figure and video).
Statement of Informed Consent
Informed consent for publication was provided by the participant (figure and video).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Data Availability
All data generated or analyzed during this study are included in this article. All data can be provided upon request to the corresponding author.
Supplemental Material
Supplemental material is available online with this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.