
Abstract
Introduction
The vast majority of cases of neonatal herpes simplex virus (HSV) infections are acquired intrapartum or postpartum, with only 5% of cases transmitted in utero. 1 Among affected neonates, ocular manifestations occur in about 13% of cases. 2 Given this low overall incidence, congenital HSV with retinal involvement is rarely reported in the literature.
In 1977, Komorous et al described 2 neonates with congenital HSV-2 infection and chorioretinal scarring, noting that 4 other cases of congenital HSV infections with chorioretinal involvement had been previously described in the literature. We identified 2 more cases, published in 1965 and 1972, describing congenital HSV infection with chorioretinal involvement. 3 As acyclovir was not approved by the United States Food and Drug Administration until 1982, none of these neonates were treated with acyclovir. 4
Table 1 lists 10 case reports published between 1986 and 2023 that describe congenital HSV-2 infections with associated retinal findings treated with acyclovir. Our case presents findings similar to 3 previously reported cases of bilateral chorioretinal scarring. In 1986, Reynolds et al 5 described a neonate with congenital HSV infection who exhibited large, bilateral atrophic macular scars. Malik et al reported a neonate born with skin lesions resembling excoriations who was initially discharged home but readmitted 6 days later owing to concern of HSV infection. Fundus examination revealed bilateral macular chorioretinal scarring without systemic involvement. 6 In 2019, Ames et al described a neonate with encephalomalacic loss of the bilateral frontal, temporal, and parietal lobes, a nearly absent corpus callosum, and a hypoplastic brainstem. At 8 weeks of age, fundus examination demonstrated multiple bilateral pigmented chorioretinal scars and no signs of active retinitis. 7
Overview of 10 Reported Cases of Congenital Herpes Simplex Virus-2 Infection With Retinal Pathology.
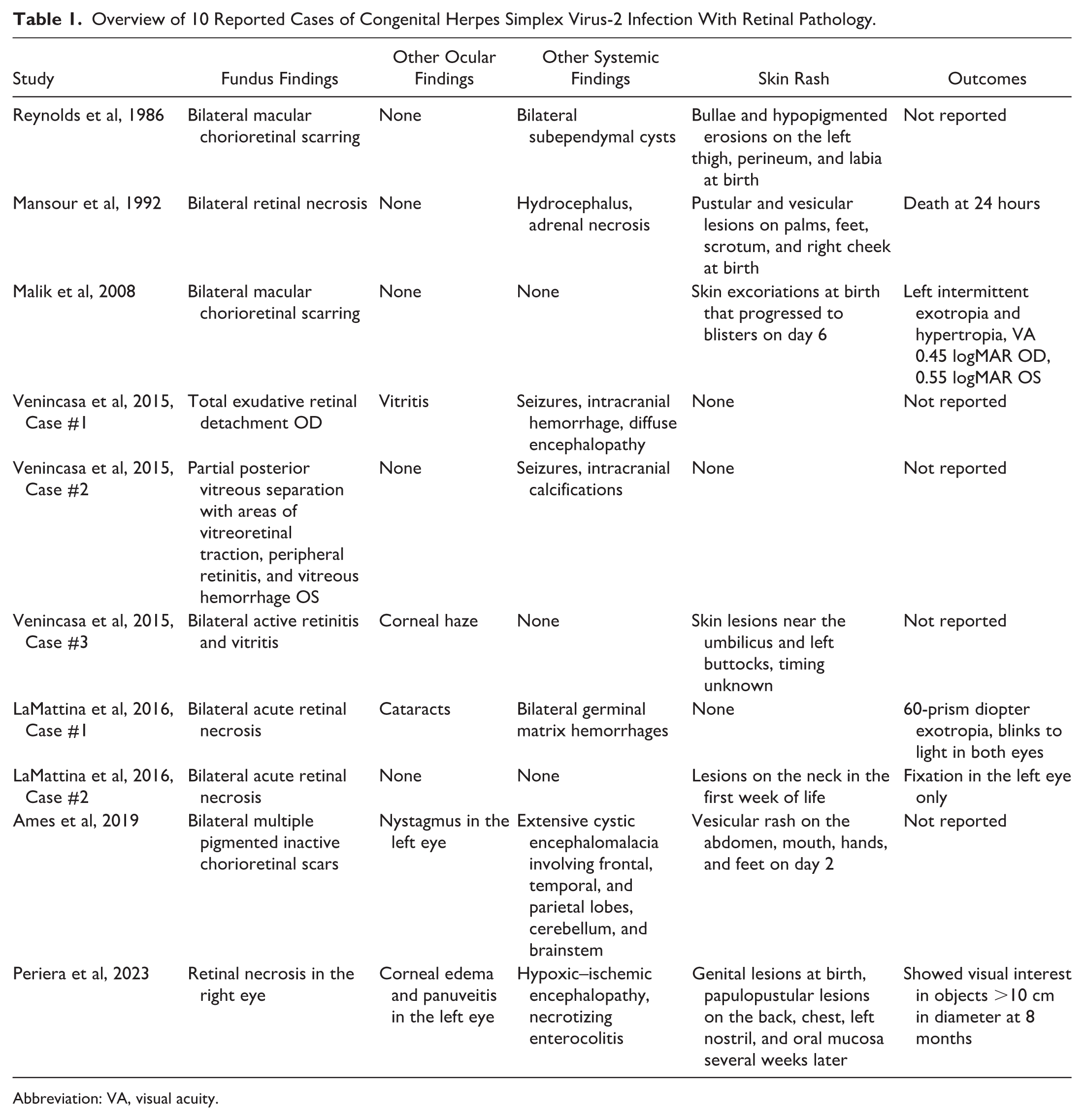
Abbreviation: VA, visual acuity.
In this case report, we describe a neonate with congenital HSV-2 infection associated with extensive neurologic abnormalities and bilateral chorioretinal scarring. Written informed consent for publication of clinical information and images was obtained from the patient’s parents.
Case Report
A male infant was delivered at 27 weeks’ gestation by cesarean section to a 22-year-old G4P2 woman after premature rupture of membranes. The mother had undergone treatment for chlamydia during pregnancy, and multiple fetal anomalies had been identified on the 20-week ultrasound. At delivery, testing for human immunodeficiency virus, syphilis, and Group B streptococcus was negative. The neonate had a birth weight of 760 g and a head circumference of 23 cm (5th percentile). Skin examination (Figure 1) revealed scattered areas of erosion and ulceration on the occipital, right parietal, and right temporal regions of the scalp, resulting in alopecic patches at the vertex consistent with aplasia cutis congenita. Similar lesions in different stages of healing were noted on the right upper extremity, left ventral wrist, central chest, and right medial thigh.

Clinical photograph of the neonate at delivery demonstrates scattered areas of erosion and ulceration involving the occipital, right parietal, and right temporal regions of the scalp, as well as the right upper extremity, left ventral wrist, central chest, and right medial thigh.
The skin findings were initially thought to be secondary to amniotic band syndrome, and bacitracin ointment was started. Empiric intravenous ampicillin and gentamicin were also started. On day 4 of life, rectal and wrist wound cultures returned positive for HSV, prompting initiation of intravenous acyclovir at 60 mg/kg/day. Cerebrospinal fluid (CSF) HSV polymerase chain reaction testing was negative, as were urine, blood, placental, and CSF cultures.
Magnetic resonance imaging of the brain (Figure 2) demonstrated marked lissencephaly with significant white matter deficiency. Small cystic foci were noted bilaterally in the regions of the basal ganglia and thalami, and the midbrain was severely hypoplastic.
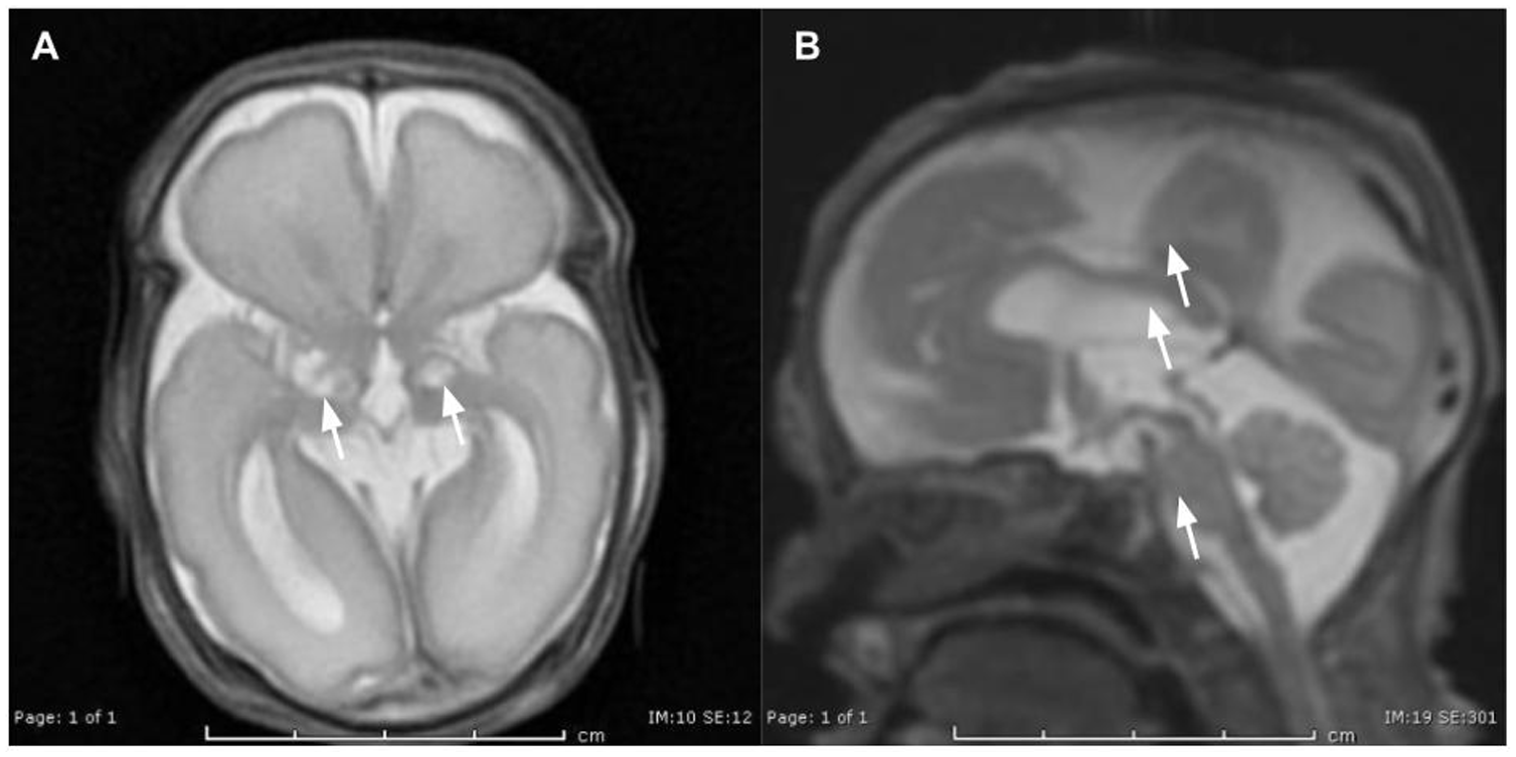
Brain magnetic resonance imaging demonstrates (A) lissencephaly with small cystic foci in the bilateral basal ganglia and thalami (white arrows), and (B) a hypoplastic midbrain (white arrows).
Ophthalmic examination revealed mild bilateral cortical cataracts. On initial fundus examination (Figure 3), the vitreous was hazy, and large, bilateral chorioretinal scars with associated hyperpigmentation were observed. There was no evidence of active retinitis in either eye.
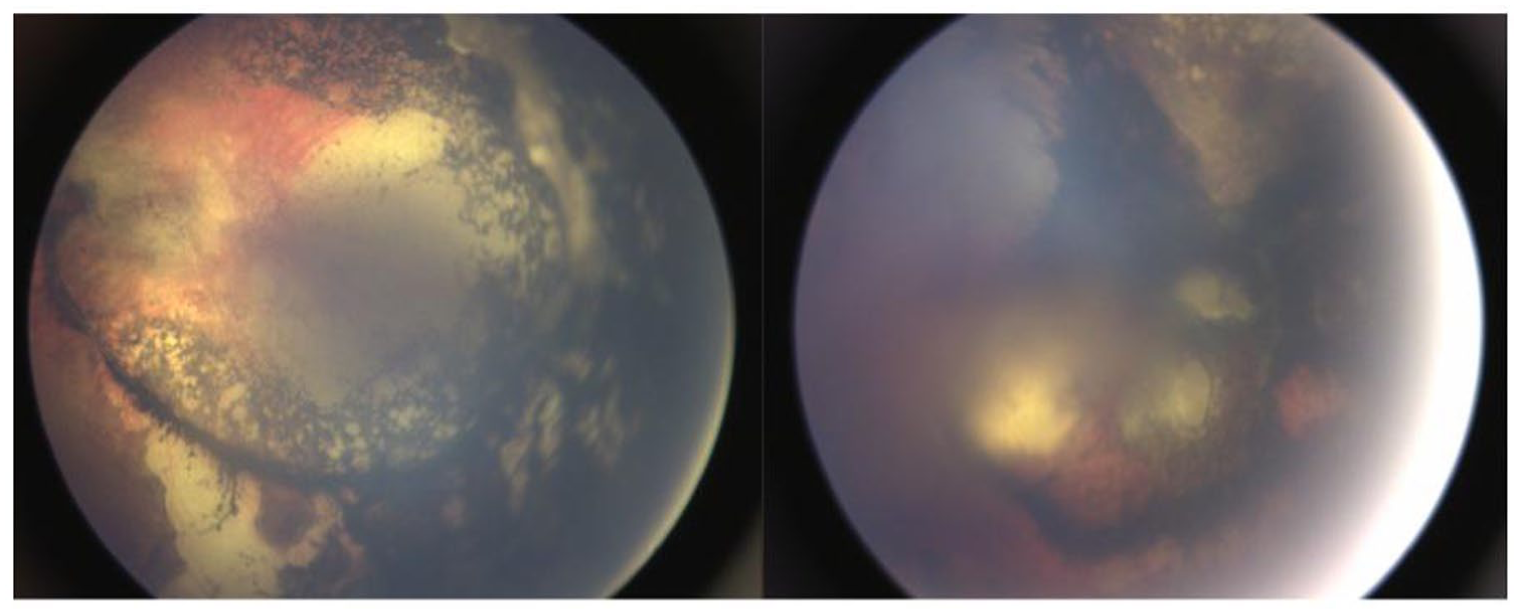
Fundus examination demonstrates large, bilateral hyperpigmented chorioretinal scars.
After 4 weeks of intravenous therapy, the neonate was switched to oral acyclovir at 300 mg/m2 per dose 3 times daily. One week later, new pustules developed on the right arm and knee, raising concerns for HSV reactivation, and intravenous acyclovir was restarted. The neonate was discharged at 5 months of age on oral acyclovir at 300 mg/m2 per dose 3 times daily. Subsequent fundus examinations have remained stable at the time of writing.
Conclusions
Based on the limited number of reported cases, congenital HSV-2 with retinal involvement appears to have a heterogeneous clinical presentation. Of the 10 cases described, 8 demonstrated bilateral retinal findings, and 7 had active retinitis or retinal necrosis. Atypical neurologic findings were reported in 7 cases. Consistent with previous literature, 8 the majority of neonates presented with a skin rash, although the morphology and timing of cutaneous manifestations varied.
Given its rarity, the pathophysiology of congenital HSV infection remains poorly understood. It may share mechanisms with acute retinal necrosis, in which the virus invades cells in all retinal layers, resulting in cell necrosis, inflammation, and vaso-occlusion of the retinal and choroidal vasculature, ultimately leading to retinal necrosis. 9 In later stages, fibrocellular membrane formation may occur, with retinal detachment reported in up to 75% of cases. 10 In our case, the constellation of extensive neurologic abnormalities and inactive bilateral chorioretinal scarring at birth, rather than evidence of active necrosis, suggests infection likely occurred in the second trimester.
Neonatal HSV infection carries a high mortality rate. Without antiviral treatment, the 1-year mortality rate is approximately 85% for disseminated disease (reduced to 29% with treatment) and 50% for central nervous system disease (reduced to 4% with treatment). 11 Early recognition is therefore critical, particularly in neonates who demonstrate clinical instability after birth, especially when accompanied by skin lesions. Although classic herpetic lesions typically progress from vesicles to ulcers, crusting, and eventual healing, intrauterine infection may present with variable cutaneous presentations. Secondary skin findings, including erosions or scarring, may indicate intrauterine disease. 12 Accordingly, HSV infection should be considered in neonates presenting with vesicles, pustules, erosions, or unexplained scarring. While congenital toxoplasmosis is the “TORCH” infection most commonly associated with chorioretinitis, 13 HSV must also be included in the differential diagnosis. Diagnostic evaluation should consist of viral culture and polymerase chain reaction testing of swabs from the conjunctiva; nasopharyngeal, oral, and anal mucosa; as well as cultures of urine, stool, blood, and CSF. 1
The American Academy of Pediatrics Committee on Infectious Diseases advises prompt initiation of high-dose acyclovir (60 mg/kg/day) for a minimum of 21 days in neonates with central nervous system or disseminated disease and for 14 days in those with disease limited to the skin, eyes, and/or mouth, followed by oral suppressive acyclovir for 6 months. 14 When clinical suspicion is high, antiviral therapy should be initiated before culture confirmation, as the risk of mortality increases with each day of delayed treatment. 15
In this case, the patient’s mother was unaware of her HSV-2 infection. Routine screening of asymptomatic pregnant patients for HSV-2 currently has limited clinical utility, as there is no curative treatment, and available serologic tests are associated with relatively high false-positive rates. 16 Nevertheless, careful evaluation at the time of labor is essential, as the presence of active genital lesions warrants delivery by cesarean section to reduce the risk of neonatal transmission.
In this case report, we present the 11th documented case of congenital HSV-2 with retinal involvement, which manifested as bilateral, inactive chorioretinal scarring. Given the limited number of reported cases, data regarding long-term visual outcomes and optimal monitoring strategies remain scarce. HSV should be included in the differential diagnosis for neonates presenting with skin lesions and chorioretinitis. Prompt initiation of antiviral therapy in cases of high degree of suspicion is essential to reduce morbidity and mortality.
Footnotes
Ethical Considerations
Our institution does not require ethical approval for the publication of individual case reports or case series. This case report was conducted in accordance with the Declaration of Helsinki. The collection and evaluation of all protected patient health information were performed in a US Health Insurance Portability and Accountability Act–compliant manner.
Consent to Participate
Informed consent, including permission for publication of all photographs and images included herein, was obtained from the patient’s parents before the procedure was performed.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Data Availability
Any data pertaining to this manuscript may be requested by emailing the corresponding author.