
Abstract
Keywords
Introduction
Central serous chorioretinopathy (CSCR) is a relatively common retinal condition that primarily affects the macula and is characterized by detachment of the retina due to the accumulation of serous subretinal fluid. While the exact mechanism of CSCR is unknown, its pathogenesis has been hypothesized to involve choroidal hyperpermeability, dysfunction of the retinal pigment epithelium, and mineralocorticoid receptor dysfunction. 1 It is more common among men, with an incidence of 9.9 cases per 100 000 men, compared to 1.7 cases per 100 000 women. 2 In acute CSCR, patients usually present with central vision loss, central scotoma, metamorphopsia, dyschromatopsia, or micropsia. 3
Various risk factors have been implicated in the development of CSCR, including genetic factors, corticosteroid use, endocrine system abnormalities, androgens, pregnancy, stress, and certain personality traits. 1 CSCR typically resolves spontaneously within 4–6 months of onset and is often managed with observation. Despite its self-limiting nature, CSCR can recur and result in vision loss, necessitating further investigation into the risk factors associated with its recurrence. Rates of recurrence range from 15% to 50%, and recurrence has a poor visual prognosis. 4 Several factors have been associated with CSCR recurrence and disease progression, such as corticosteroid use, untreated hypertension, a thickened subfoveal choroid, less intense hyperfluorescence demonstrated on fluorescein angiography, and shift work.5,6 Additionally, mental health conditions like depression and anxiety have been linked to an increased risk of recurrence in both acute and chronic CSCR. 7 However, the factors contributing to its recurrence, particularly in the context of different management strategies, remain ill-defined.
A wide range of treatments for CSCR have been studied in clinical practice, ranging from laser photocoagulation to photodynamic therapy (PDT). For acute and chronic CSCR, low-fluence PDT has emerged as the first-line treatment. 8 Given the significant impact of CSCR on visual acuity and quality of life, understanding the predictors of recurrence is crucial for optimizing patient management. This retrospective case–control study investigates the demographics, medical history, and retinal imaging findings among patients with first-time CSCR to elucidate the risk factors associated with recurrence. Specifically, it compares the recurrence rates and associated risk factors between patients managed with observation alone and those treated with PDT.
Methods
Data Source and Study Sample
The study was designed as a retrospective case–control analysis conducted at a single private practice retina specialist group. The patient cohort comprised individuals diagnosed as having active CSCR for the first time between January 2014 and January 2018. A total of 90 patients were included in the study, with eligibility determined according to specific inclusion and exclusion criteria.
Sample Selection
The study population consisted of patients with a first-time diagnosis of active CSCR provided by a retina specialist. Considering that most cases of CSCR resolve without treatment, the initial management of CSCR involved 4–6 months of observation for all patients. Follow-up was maintained for at least 1 year after the first episode to monitor for resolution or recurrence. If PDT was performed following initial observation, an additional year of follow-up post-PDT was required. Of note, the retina specialists did not utilize antivascular endothelial growth factor (anti-VEGF) therapy, focal laser photocoagulation, or mineralocorticoid receptor antagonists for treatment of CSCR. Patients with a history of CSCR or with incomplete medical records or incomplete follow-up data were excluded from the study.
Data Collection
Demographic data, medical history, and retinal imaging findings were recorded for all patients. Key variables included age, gender, baseline visual acuity, central subfield thickness on optical coherence tomography (OCT), steroid use, and the use of exogenous hormones. The study methods align with those used in previous studies, highlighting the importance of these parameters in CSCR research. 8 Informed consent was waived given the retrospective study design and use of de-identified data.
Outcome Measures
The primary outcome was the recurrence of CSCR, defined as the presence of new subretinal fluid following prior resolution. 9 Secondary outcomes included the association of recurrence with demographic factors, medical history, and baseline retinal imaging findings. This approach follows the standard practices in CSCR research for monitoring disease progression and treatment efficacy.
Statistical Analysis
Descriptive statistics for categorical variables are expressed as counts and percentages. Data for continuous variables are expressed as the mean (±SD) and median (interquartile range). Comparative analyses were conducted using Barnard’s exact test or t-tests, when appropriate. Kaplan-Meier survival curves were used to illustrate time to recurrence, stratified by exogenous hormone use. Odds ratios (ORs) with 95% confidence intervals (95% CIs) were calculated to assess the predictive value of different variables. Statistical significance was set at a P value < .05. Adjusted analyses were performed using generalized linear models to assess associations between change in best-corrected visual acuity (BCVA) and baseline clinical and demographic characteristics and the outcome variable of recurrence of CSCR. Explanatory variables included stress, steroid use, exogenous hormone use, tobacco use, psychiatric diseases, and subretinal hyperreflective material.
Results
Patient Demographics
The patient population consisted of 90 individuals with a diagnosis of CSCR, with 56 in the observation group and 34 in the PDT group (Table 1). A total of 67.8% of the patient population were male, while 32.2% were female, with no significant difference between groups. The mean age of the total cohort was 52.4 years, with a similar mean age between groups (P = .29). Relevant comorbidities included psychiatric disease (14.4%), cardiovascular disease (30.0%), and diabetes (13.3%), with no significant differences between groups. Notably, exogenous hormone use, including testosterone and estrogen (Table 2), was significantly higher in the PDT group than in the observation group (17.6% vs 3.6%; P = .025). Other factors, such as asthma or seasonal allergies (26.7%), history of tobacco use (28.9%), and steroid use (30.0%), showed no significant differences between groups.
Demographics and Baseline Medical History of Patients With Central Serous Chorioretinopathy in the Observation Versus PDT Group.
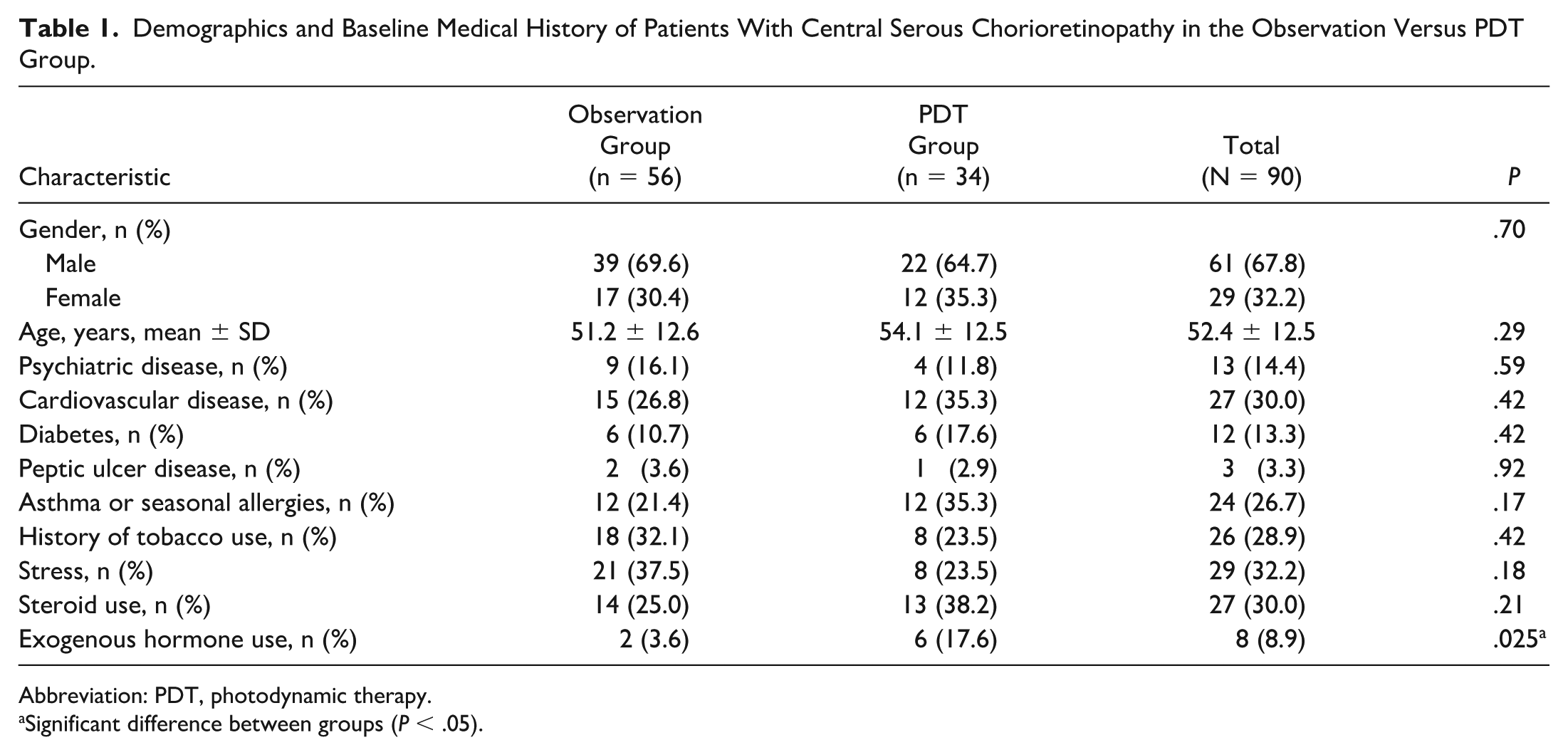
Abbreviation: PDT, photodynamic therapy.
Significant difference between groups (P < .05).
Use of Exogenous Hormones by Type in Patients With Central Serous Chorioretinopathy (N = 8).
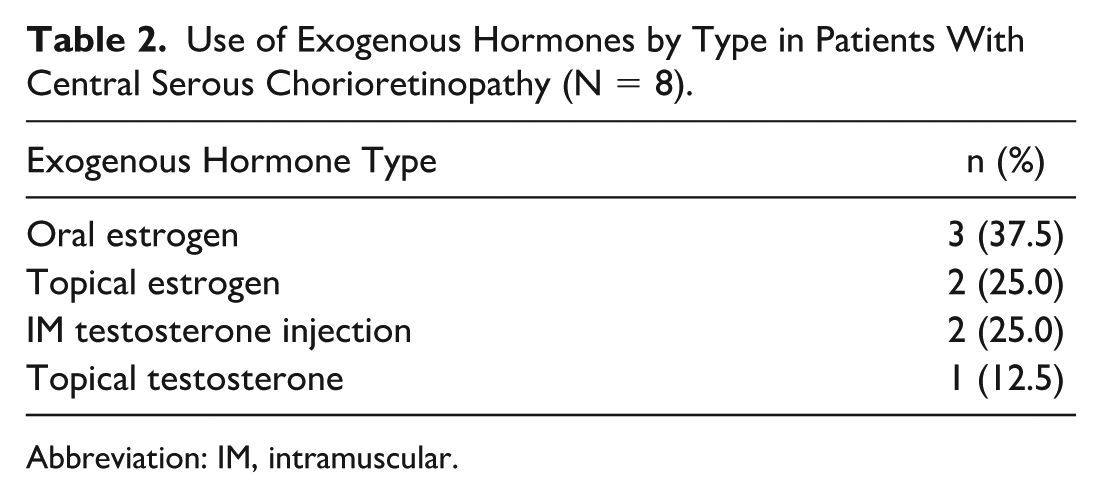
Abbreviation: IM, intramuscular.
Clinical Characteristics
The clinical and retinal imaging characteristics of the patient population revealed several notable findings (Table 3). Baseline BCVA, as displayed in Figure 1, was significantly worse in the patients who eventually underwent PDT (mean ± SD 0.41 ± 0.33 logMAR) compared to the observation group (mean ± SD 0.23 ± 0.27 logMAR; P < .001). Total length of follow-up was longer in the PDT group (mean ± SD 26.6 ± 18.2 months) compared to the observation group (mean ± SD 20.5 ± 13.9 months; P = .08). Duration of initial symptoms, recurrence rates, mean time to first recurrence, baseline central retinal thickness, and baseline fluorescein angiography patterns showed no significant differences between groups. These results are consistent with the understanding that worse visual acuity at presentation is more common in patients who ultimately require PDT. 5
Clinical and Retinal Imaging Characteristics of Patients With Central Serous Chorioretinopathy in the Observation Versus PDT Group.
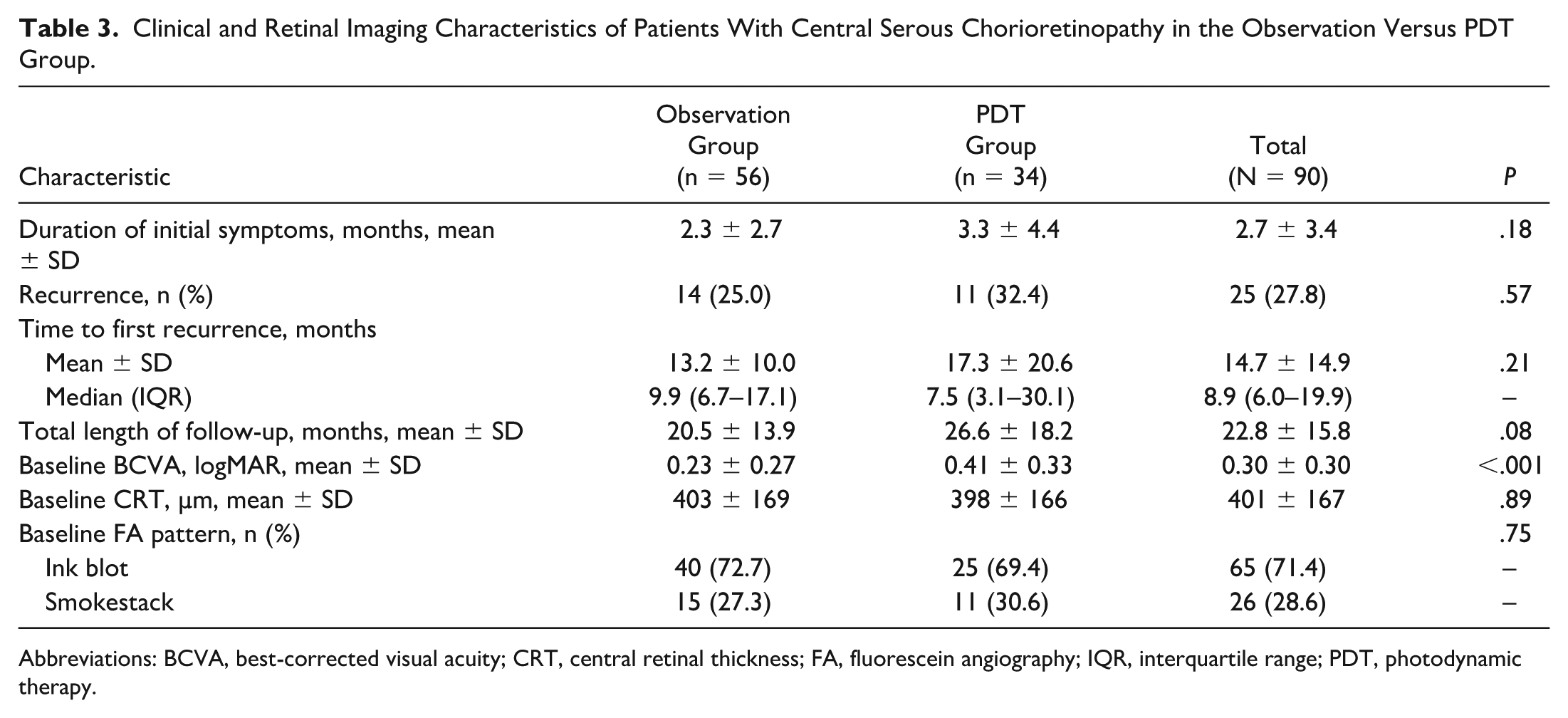
Abbreviations: BCVA, best-corrected visual acuity; CRT, central retinal thickness; FA, fluorescein angiography; IQR, interquartile range; PDT, photodynamic therapy.
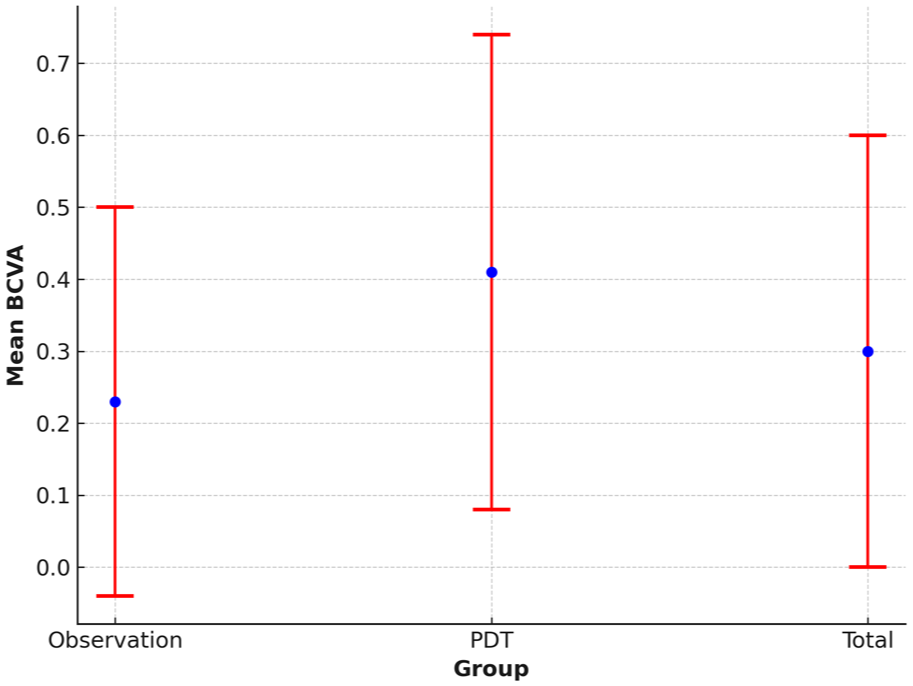
Baseline best-corrected visual acuity (BCVA) in patients with central serous chorioretinopathy in the total cohort (N = 90) and by treatment group (low-fluence photodynamic therapy [PDT], n = 34; managed by observation alone, n = 56). Bars show the mean ± SD logMAR.
Recurrence Rates
Twenty-five patients experienced CSCR recurrence: 14 in the observation group and 11 in the PDT group (P = .57). Among those who received PDT, only 5 (14.7%) experienced recurrence after treatment. Three of these 5 patients had a single recurrence within 1 year after PDT. One patient had a recurrence at more than 2 years post-PDT, and the other patient had a recurrence at more than 3 years post-PDT. Of these 5 patients, 1 subsequently received repeat PDT, which led to resolution of the subretinal fluid accumulation. Two patients had spontaneous clearance of subretinal fluid in the ensuing months post-PDT. One patient did not follow up. One patient required 2 additional sessions of PDT for recurrent CSCR and eventually developed choroidal neovascularization, prompting anti-VEGF therapy. These results are consistent with the management of severe cases of CSCR with PDT.
Figure 2 illustrates a case of CSCR that spontaneously resolved following observation, achieving stability at 10 months. Figure 3 illustrates a case of recurrent CSCR in a patient taking intramuscular testosterone who underwent PDT, resulting in good clearance of subretinal fluid and improvement in the outer retina at 10 months post-PDT.
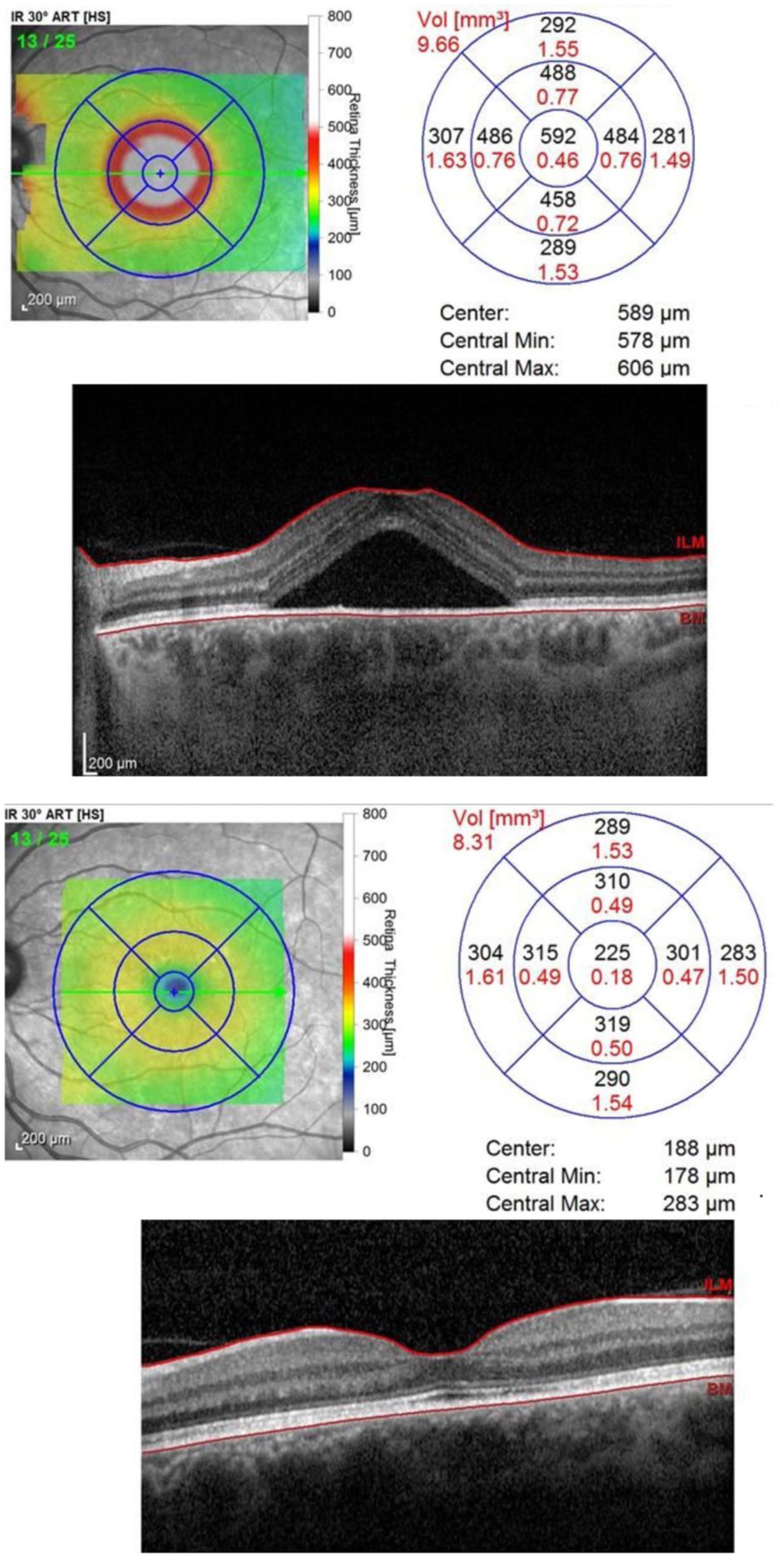
Case of central serous chorioretinopathy managed with observation, with stability achieved after 10 months. Top panels show infrared reflectance (IR) and optical coherence tomography (OCT) images of the retina before observation, demonstrating a large pocket of central subretinal fluid. Bottom panels show IR and OCT images after observation, demonstrating spontaneous resolution of subretinal fluid accumulation. Diagrams (top and bottom panels) map the retinal thickness and volume (Vol) before and after resolution. Abbreviations: ART[HS], automatic real-time tracking [high-speed]; BM, Bruch’s membrane; ILM, internal limiting membrane; Min, minimum; Max, maximum.
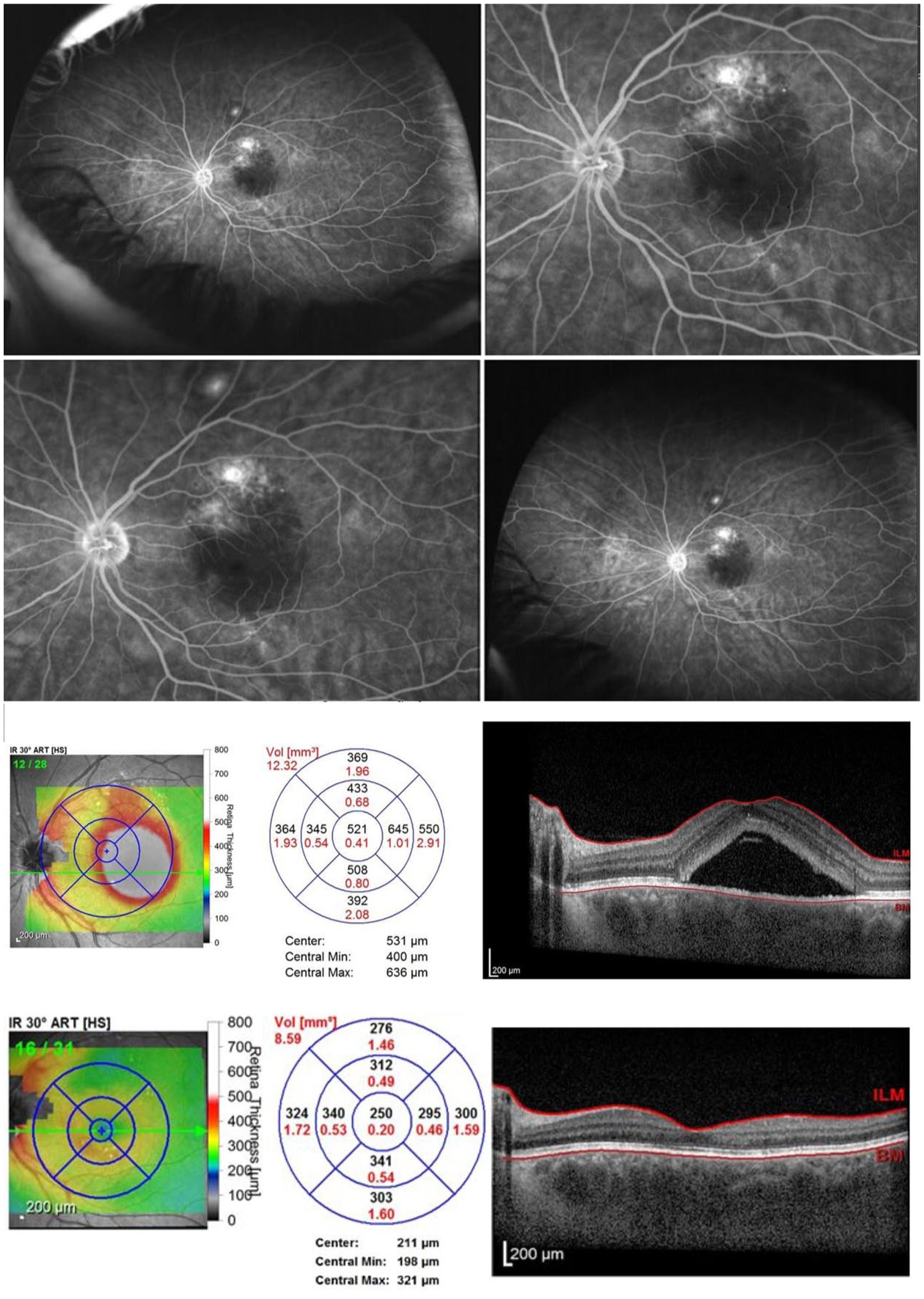
Case of recurrent central serous chorioretinopathy (CSCR) in a patient taking intramuscular testosterone who underwent photodynamic therapy (PDT). Top panels show initial fluorescein angiography images of the retina, demonstrating patchy hyperfluorescence and leakage in the superior macula. Middle panels show initial infrared reflectance (IR) and optical coherence tomography (OCT) images of the retina, demonstrating thick choroid, retinal pigment epithelium changes, and serous macular detachment secondary to CSCR. Bottom panels show IR and OCT images of the retina at 10 months post-PDT, demonstrating excellent clearance of subretinal fluid and improvement in the outer retina. Diagrams (middle and bottom panels) map the retinal thickness and volume (Vol) before and after PDT. Abbreviations: ART[HS], automatic real-time tracking [high-speed]; BM, Bruch’s membrane; ILM, internal limiting membrane; Min, minimum; Max, maximum.
Exogenous hormone use was a significant predictor of CSCR recurrence (OR 5.2, 95% CI 1.1–23.6; P = .034) (Table 4). Kaplan-Meier survival curves analyzing the time to CSCR recurrence among all patients, stratified by exogenous hormone use, suggests that a higher percentage of patients taking exogenous hormones experienced recurrence (P = .034) (Figure 4). Other factors, such as stress, steroid use, tobacco use, psychiatric disease, and subretinal hyperreflective material, did not show significant associations with recurrence in either the observation group or the PDT group (Table 4).
Factors Associated With Central Serous Chorioretinopathy Recurrence in the Observation Versus PDT Group.
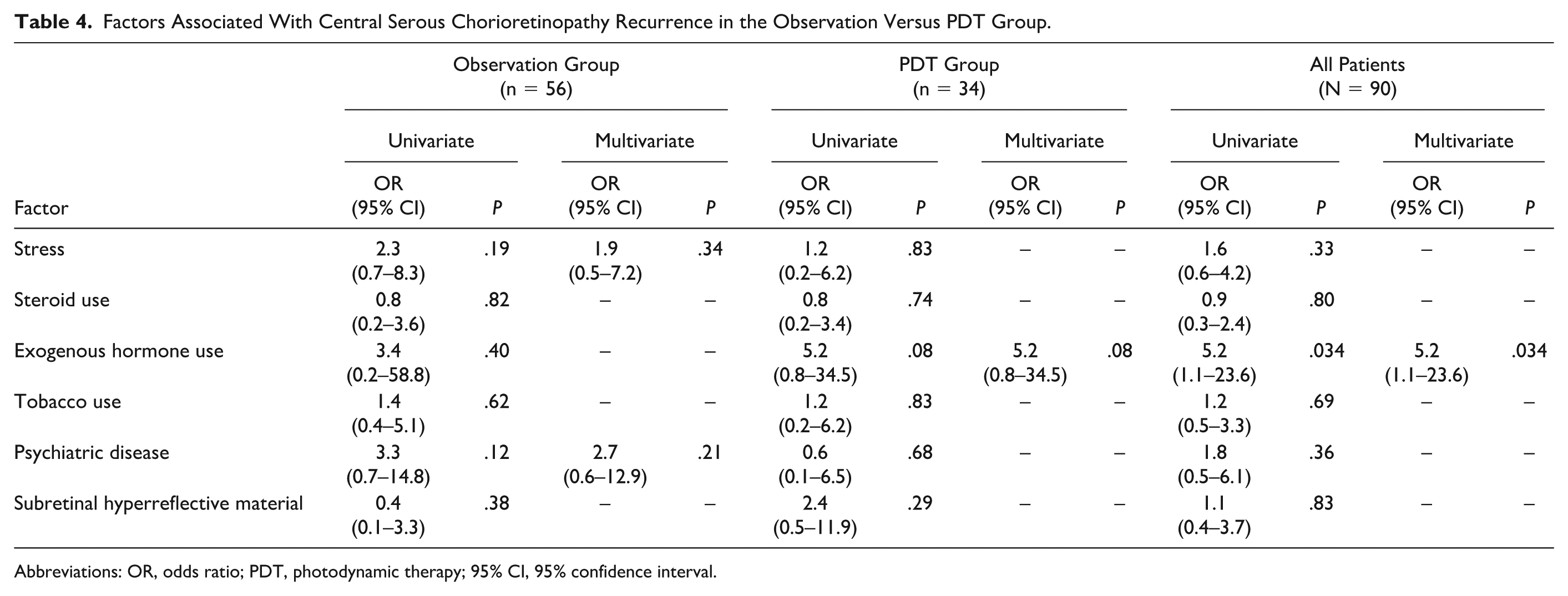
Abbreviations: OR, odds ratio; PDT, photodynamic therapy; 95% CI, 95% confidence interval.
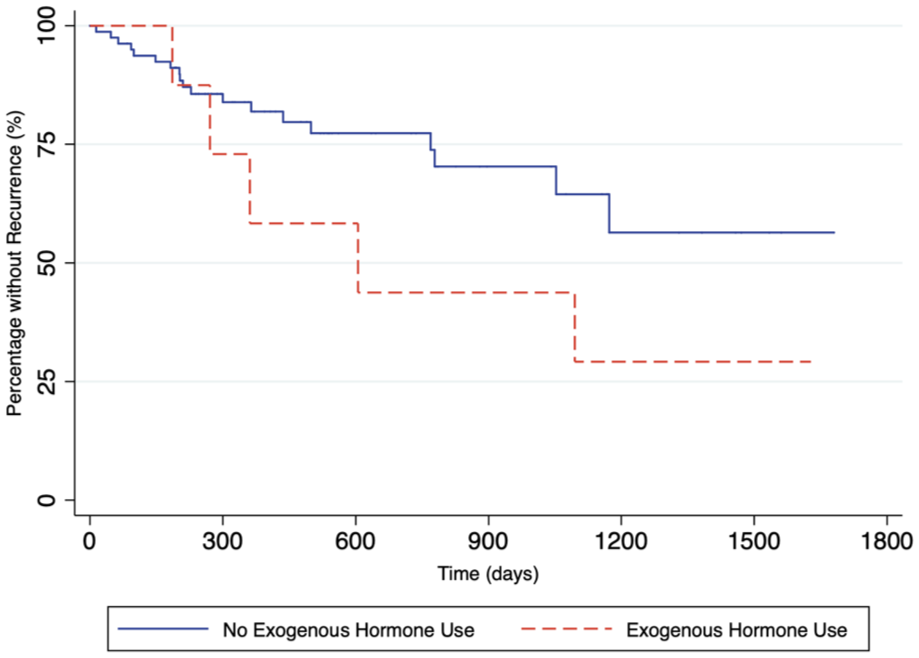
Kaplan-Meier curves of time to recurrence of central serous chorioretinopathy, stratified by exogenous hormone use (N = 90).
Conclusions
The findings from our study underscore the potential role of exogenous hormone use in the risk of recurrence of CSCR. Our data demonstrate that exogenous hormone use was associated with a notably higher risk of recurrence (OR of 5.2). This highlights the importance of considering exogenous hormone use as a potential risk factor in the management of CSCR. The presence of sex hormone receptors throughout the eye, including the retina, indicate that both endogenous and exogenous hormones can influence various ocular tissues. 10 For instance, a retrospective case series of patients experiencing blurred vision while taking exogenous testosterone (mean duration of therapy 14 months) for treatment of low-testosterone levels found that all patients had CSCR and increased choroidal thickness. 11 Additionally, 2 other studies of patients with chronic CSCR found that the levels of sex hormones were elevated in these patients.12,13
There are some other findings worth elaborating, including the fact that patients in our study who went on to have recurrence had worse baseline BCVA at initial presentation. This suggests that poorer visual acuity at the onset of CSCR may be a potential risk factor for recurrence or a sign of recalcitrant disease. Clinicians should consider baseline BCVA when assessing the risk profile of CSCR patients and thereby tailor management strategies accordingly.
While PDT is a treatment option, patients taking exogenous hormones may be at higher risk for recurrence and may benefit from strategies to reduce hormone exposure. In our study, among those who underwent PDT, only 5 (14.7%) experienced recurrence after treatment. This suggests that PDT may have a protective effect against recurrence, although the difference compared with the observation alone group was not statistically significant.
To ascertain the implications of our study on public health, it is crucial to assess the prevalence of exogenous hormone utilization. Exogenous testosterone and estrogen are commonly prescribed for various clinical indications, including hypogonadism, menopause, and oral contraception. The use of exogenous hormones has diminished from their historical peaks. Testosterone usage among men ages ≥30 years reached its highest point in 2013 at 3.2%, subsequently declining to ~1.7% by 2016. 14 Similarly, the use of hormone replacement therapy (HRT) among postmenopausal women peaked between 1999 and 2002, with 1 in 5 women ages ≥40 years receiving this treatment, but this rate decreased to fewer than 1 in 20 by 2009–2010. 15 Despite these declines, recent data indicate a marked increase in exogenous hormone use, particularly in gender-affirming care. An analysis on insurance claims data revealed a 781% increase in the use of hormone therapy among patients with gender dysphoria between 2013 and 2019. 16 As exogenous hormone use becomes more widespread for gender-affirming care, understanding the ocular risks associated with long-term hormone therapy becomes increasingly important. While the use of exogenous hormones has diminished from their historical peaks, millions of individuals still take these hormones, potentially placing them at risk for developing recurrent CSCR.
Given the findings of exogenous hormone use as a potential risk factor for the recurrence of CSCR and widespread prescription of hormone therapies, it is important for retina specialists managing CSCR to be aware of this risk and to incorporate it into their clinical decision-making processes. Educating patients on the potential ocular risks associated with exogenous hormone use is essential for informed consent and effective disease management. For clinicians managing CSCR, our findings suggest the importance of assessing hormone use as part of the patient history. In patients with a history of CSCR or those at high risk of recurrence, alternative therapies to exogenous hormones should be considered. Additionally, strategies to mitigate hormone use, such as dose reduction or discontinuation, may be beneficial in reducing recurrence risk. Furthermore, educating clinicians who prescribe exogenous hormones would be advantageous, enabling them to inform patients about the potential risks associated with these treatments.
It is important to acknowledge several limitations in our study. Our sample size was limited to patients within a single private practice in Texas in a small catchment area and further stratification of the data led to smaller sample sizes. The increased recurrence rate in the PDT group may be due to bias in selecting patients who needed PDT, given the retrospective, nonrandomized study design. That is, patients who had chronic CSCR that was more difficult to treat were more likely to receive PDT and also more likely to have had recurrent CSCR. Exogenous hormone use was self-reported, which is subject to bias, and no testosterone or estrogen levels were measured. Additionally, understanding the dosage of exogenous hormones would have been beneficial in determining a specific dose-response relationship, such as whether higher doses of HRT correlate with a higher risk of CSCR recurrence or with greater difficulty in clearing subretinal fluid. Unfortunately, we did not have access to detailed dosage information in this study. Furthermore, we did not have a consistent protocol in place to recommend dose reduction or discontinuation of exogenous hormones (or corticosteroids). Future studies should aim to include this data to provide a more comprehensive understanding of the relationship between hormone dose and severity of disease as well as relationship between hormone dose and risk of recurrence. Another limitation is that we did not specifically assess choroidal thickness as a variable.
Interestingly, our study did not identify corticosteroid use as a statistically significant risk factor for recurrent CSCR. However, there was a trend toward significance, in that patients taking corticosteroids were more likely to require PDT, presumably because they had chronic recalcitrant CSCR. The small sample size may have been responsible for the inability to detect a significant effect of corticosteroids.
Further research is warranted to explore the mechanisms by which exogenous hormones influence CSCR and to identify potential therapeutic targets for mitigating this risk. Longitudinal studies with larger sample sizes and diverse populations will be critical in confirming our findings and elucidating the interplay between different risk factors for CSCR recurrence.
Our study contributes to the growing body of literature on CSCR and underscores the need for personalized management strategies that consider individual risk factors, including exogenous hormone use. By integrating these insights into clinical practice, we can improve outcomes for patients with CSCR and enhance their quality of life.
Footnotes
Acknowledgements
We thank the staff and photographers at the Retina Consultants of Austin as well as the patients who participated in this study.
Ethical Approval
Ethical approval for this study was obtained from The University of Texas at Austin Institutional Review Board (no. 2020-02-0073). This research was conducted in accordance with the Declaration of Helsinki. The collection and evaluation of all protected patient health information was performed in a Health Insurance Portability and Accountability Act–compliant manner.
Statement of Informed Consent
Informed consent was waived given the retrospective study design and the use of de-identified data. An exemption was granted from the University of Texas at Austin Institutional Review Board.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.