
Abstract
Introduction
Acute retinal necrosis (ARN) is characterized by rapidly progressive necrotizing retinitis, retinal arteritis, and a prominent inflammatory reaction in the vitreous and anterior chamber. 1 The most common cause of ARN is varicella-zoster virus (VZV), followed by herpes simplex virus 1 and 2 (HSV-1, HSV-2), and, uncommonly, cytomegalovirus (CMV). While rare, concomitant infections causing ARN have been reported in the literature.2 –4 Recognition of concomitant infections is important to ensure that proper treatment is initiated in these patients. Complications of ARN include retinal detachment, macular ischemia, and optic atrophy.4,5 Polymerase chain reaction (PCR) of intraocular fluid samples is used to confirm the diagnosis.
Here, we describe a novel case of an immunocompromised patient with bilateral concomitant CMV retinitis and ARN due to VZV. He initially deteriorated to an uncorrected distance visual acuity of no light perception (NLP) in his left eye, which improved after systemic and intravitreal antiviral therapy. We discuss the clinical presentation, management, and outcomes of this rare concomitant infection.
Case Report
A 36-year-old man with HIV and AIDS not adherent to highly active antiretroviral therapy (HAART) presented to the emergency department with painful vision loss in the left eye that began 3 days prior. He had no history of opportunistic infections or any prior episodes of herpes zoster. The patient’s viral load was 632 000 copies/mL, and his CD4 count was 25 cells/mm3. On examination, the patient’s uncorrected distance visual acuity was 20/20 in the right eye and counting fingers at 3 feet (≈1 m) in the left eye. Intraocular pressure (IOP) was 16 mm Hg and 18 mm Hg, respectively. The patient had an afferent pupillary defect in the left eye. Extraocular movements were intact. On anterior segment examination, the patient had a conjunctival injection and +1 mixed cell in the anterior chamber and anterior vitreous of both eyes. Fundus examination was notable for a healthy-appearing optic nerve in the right eye and disc edema in the left eye (Figure 1). The right eye had multiple foci of punctate, intraretinal hemorrhages (Figure 2A). The left eye had areas of confluent retinal necrosis and occlusive vasculitis in the peripheral retina that extended to the posterior pole (Figure 2B). There were also areas of granular retinitis in the periphery. Magnetic resonance imaging of the brain without contrast demonstrated no abnormalities that were concerning for encephalitis. Based on clinical examination, bilateral ARN was suspected. A diagnostic anterior chamber paracentesis of the left eye and intravitreal foscarnet injections (2.4 mg/0.1 mL) in both eyes were performed. The patient was admitted to the hospital and started on intravenous acyclovir (15 mg/kg) every 8 hours.
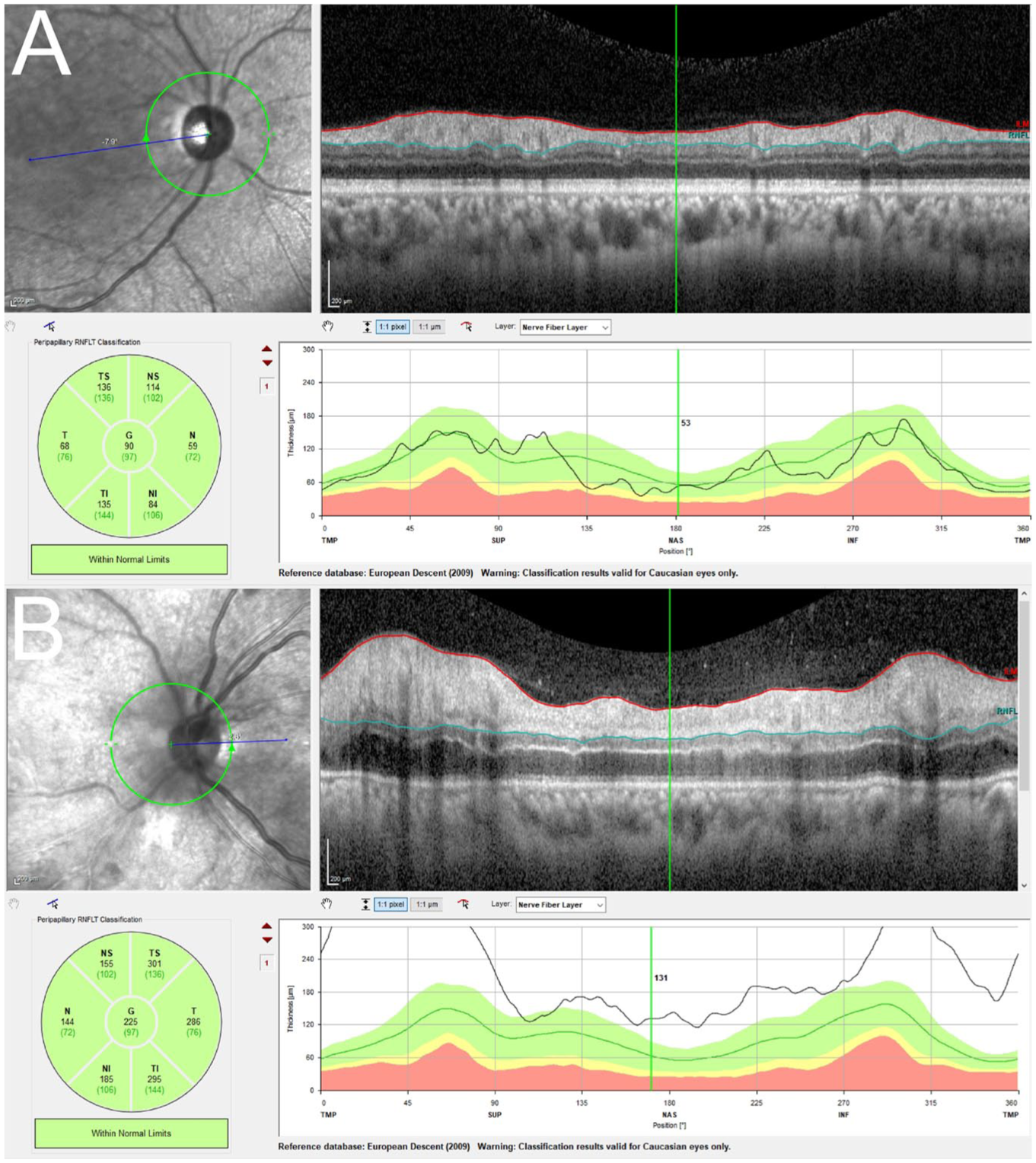
(A and B) Right and left eye, respectively. Optical coherence tomography of the retinal nerve fiber layers of both optic nerves at initial presentation, demonstrating a normal optic disc in the right eye (90 µm) and a swollen optic disc in the left eye (225 µm).
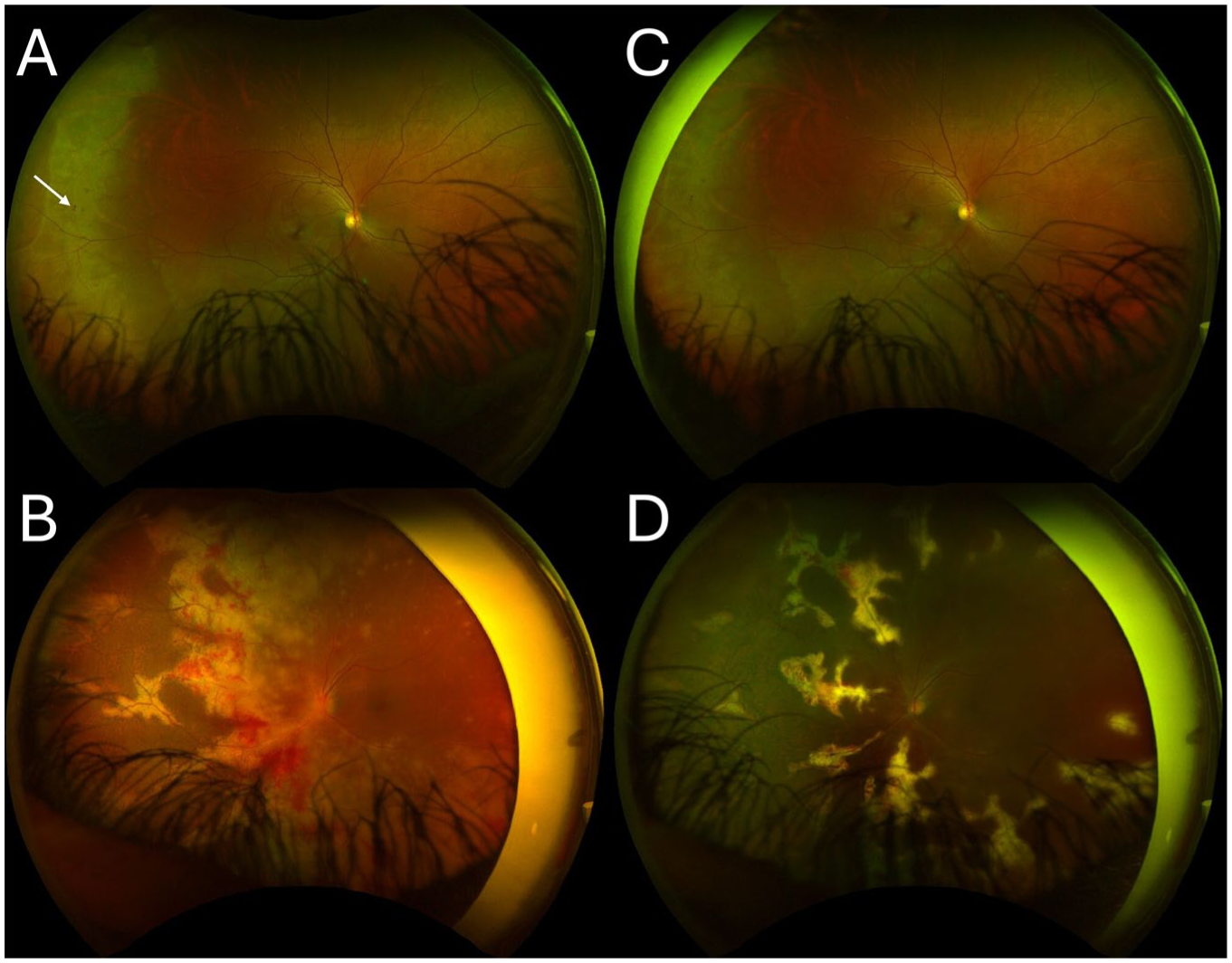
(A) Color fundus photograph of the right eye at initial presentation before treatment, demonstrating multiple foci of punctate, intraretinal hemorrhages (arrow). (B) Color fundus photograph of the left eye at initial presentation before treatment, demonstrating diffuse yellow white retinal lesions with scattered retinal hemorrhages. (C and D) Color fundus photographs of the right and left eyes, respectively, 5 weeks after initial presentation, demonstrating interval improvement of retinitis in both eyes and improvement of left optic nerve edema after systemic and intravitreal antiviral therapy.
Five days after the onset of symptoms and 2 days after the intravitreal foscarnet injection, the uncorrected distance visual acuity in the left eye worsened to NLP. The right eye uncorrected distance visual acuity remained 20/20. The patient was switched to oral valganciclovir 900 mg twice per day and received 2 additional intravitreal foscarnet injections (2.4 mg/0.1 mL). The diagnostic anterior chamber paracentesis PCR testing was positive for VZV (7.5E+7 copies/mL) and CMV (1423 IU/mL) but was negative for HSV-1 and HSV-2. Over the next week, the patient was treated with 2 additional intravitreal foscarnet injections in the right eye.
Two weeks after the initial onset of the symptoms, the patient’s uncorrected distance visual acuity in the left eye improved to hand motions at 3 feet (≈1 m) with an examination notable for resolution of the optic nerve edema and improvement in retinal whitening. The uncorrected distance visual acuity and examination remained stable in the right eye. The patient was continued on oral valganciclovir and restarted on HAART.
The patient missed scheduled follow-ups but presented again 5 weeks after the initial onset of symptoms. Visual acuity remained stable at 20/20 and hand motions in the right and left eye, respectively. On fundus examination, interval improvement in retinitis was observed after systemic and intravitreal antiviral therapy (Figure 2, C and D). The patient has since missed subsequent follow-ups.
Conclusions
We present the case of an immunocompromised patient with bilateral concomitant CMV retinitis and ARN secondary to VZV. This concomitant infection is rare, and to our knowledge, only 1 other case has been reported in the literature. 2 Our case is the only reported case with these concomitant infections in an immunocompromised patient.
CMV is a common opportunistic infection in immunocompromised patients. The incidence of CMV retinitis has decreased as a result of modern HAART, but it can still cause significant morbidity in those who remain untreated. 6 Several variants of CMV retinitis have been described, including the classic, or fulminant, form with marked retinal hemorrhage and necrosis in the posterior pole; a granular variant, more common in the retinal periphery; and a perivascular form, also known as frosted-branch angiitis. A suspicion of CMV retinitis is generally made clinically and can be confirmed by PCR testing of intraocular fluids. Treatment for CMV retinitis includes oral valganciclovir, intravenous ganciclovir, foscarnet, or cidofovir.
ARN often presents with arteritis and phlebitis of the retina and choroidal vasculature, confluent necrotizing retinitis commonly affecting the peripheral retina, and vitritis. Retinal detachment is a common complication, occurring in approximately 70% of cases. It is a rare, vision-threatening disease that can affect both immunocompetent and immunocompromised patients. 7 Like CMV retinitis, the diagnosis of ARN is based on clinical examination but can be confirmed with PCR testing. Treatment for ARN includes intravenous acyclovir, oral valacyclovir, and oral corticosteroids.
Concomitant infections in the setting of ARN are rare, though they have been described in the literature before. Chen et al and Cheraqpour et al reported 2 separate cases of concomitant HSV and VZV retinitis in an immunocompetent patient and an immunocompromised patient, respectively.3,4 Furthermore, Nakamura et al described a case of VZV and CMV concomitant infections in an immunocompetent patient. 2 Synergistic interactions between viral pathogens have been found to facilitate increased replication and severity of concomitant viruses through modulation of cellular and immune defenses. 8
Notably, our patient was infected with CMV and VZV, 2 members of the Herpes viridae family, which have been reported in cases of corneal endotheliitis and encephalitis.9,10 There may be potential synergistic effects between the 2 herpes viruses that led to more severe disease progression in this case. Our patient may have had concomitant infections given his severely immunocompromised state, but further research is necessary to understand the risk factors and expected outcomes for concomitant infections in both immunocompromised and immunocompetent patients.
In the 3 patient cases reported in the literature, all patients developed subsequent rhegmatogenous retinal detachments necessitating surgery. Retinal detachments are a common complication of viral retinitis, reported at rates of 50% per patient per year or 33% per eye per year, but were not seen in this case. The patient missed subsequent follow-ups, however, so it is unknown (although likely) whether a detachment developed after the initial treatment period. 11 Outcomes after ARN are poor, as was seen in the 3 cases reported prior.
Return of vision after worsening to NLP has been described in the settings of ocular trauma but has not been well studied in settings of infection. 12 To our knowledge, it has never been described in the setting of retinitis resulting from viral concomitant infections. A multicenter study on bilateral ARN outcomes included 2 patients with uncorrected distance visual acuity of NLP at initial presentation who did not regain vision after receiving appropriate medical and surgical treatment. 13 Our case documents vision improvement from NLP after systemic antiviral treatment for CMV retinitis and ARN secondary to VZV, with resolution of the optic nerve edema in the left eye. Improvement from NLP vision is documented in cases with inflammatory etiologies like giant cell arteritis and optic neuritis; in these cases, the resolution of severe optic nerve edema coincided with improvement from NLP vision.14,15 The mechanism of vision loss in optic nerve edema is thought to be related to mechanical disruption causing nerve fiber dysfunction as a result of localized swelling. 16 Therefore, we theorize the improvement from NLP vision in this patient may be more related to the resolution of optic nerve edema versus improvement in retinitis.
In conclusion, VZV and CMV DNA were detected in the aqueous of a patient with bilateral concomitant CMV and VZV retinitis. Prompt diagnosis and antiviral treatment lead to vision improvement. This case suggests that combined systemic and local treatment can lead to vision improvement for patients with viral retinitis, even in cases of NLP vision.
Footnotes
Ethical Approval
Institutional review board approval was waived.
Statement of Informed Consent
Informed consent was obtained from the patient.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.