
Abstract
Introduction
A retinal arterial macroaneurysm is a rare acquired vascular lesion of the retina 1 characterized by a focal dilation (100 μm to 250 μm in diameter) of the retinal artery, usually in the first 3 orders of bifurcations of the retinal arterial system and often within the temporal quadrant. 2 Most cases are unilateral, and these lesions are more common in women and in patients older than 75 years. Retinal arterial macroaneurysms are strongly associated with chronic systemic hypertension, arteriosclerosis, and dyslipidemia. 3 Chronic vascular insult is thought to result in focal ischemia in the muscularis layer of the arteriolar wall, leading to fibrosis and collagen remodeling, decreased wall thickness and elasticity, and increased permeability. 4 This remodeling process predisposes the artery to saccular or fusiform aneurysmal arterial dilation.
Retinal arterial macroaneurysms can be classified into the following 3 clinical entities that dictate the type and severity of symptoms: quiescent, hemorrhagic, and exudative. 2 The quiescent type is usually discovered incidentally in asymptomatic patients. The hemorrhagic form presents with acute, rapid vision loss and is associated with larger arteries closer to the disc with a multilayered hemorrhage. Conversely, exudative retinal arterial macroaneurysms are associated with a gradual, indolent deterioration in vision that is characterized by circinate lipid deposition around the aneurysm in addition to intraretinal fluid (IRF) and subretinal fluid (SRF) accumulation resulting from increased vascular permeability.5,6 Patients with nonhemorrhagic retinal arterial macroaneurysms may have an increased risk for developing retinal vein occlusion (RVO), whereas more severe cardiovascular risk factors are typically seen in patients with hemorrhagic retinal arterial macroaneurysms.3,7
Here, we report a rare case of an exudative juxtafoveal retinal arterial macroaneurysm that was initially diagnosed as cystoid macular edema (CME) secondary to a branch RVO (BRVO). The patient was initially treated twice with empiric intravitreal (IVT) aflibercept without improvement. Further ancillary imaging with optical coherence tomography angiography (OCTA) and intravenous fluorescein angiography (FA) confirmed the presence of a juxtafoveal retinal arterial macroaneurysm in close proximity to the foveola. Treatment with light fovea-sparing focal laser photocoagulation resulted in anatomic and visual improvement.
Case Report
A 49-year-old man with a history of prediabetes and hypercholesteremia presented with an indolent history of worsening unilateral decreased vision and a paracentral scotoma. His ocular history was insignificant. His medical history did not include hypertension. His son had an incidental finding of a cerebral varix.
On presentation, the patient’s best-corrected visual acuity (BCVA) was 20/150 OD and 20/20 OS. The anterior segment was unremarkable. A retinal examination found extensive IRF and SRF associated with perifoveal exudates (Figure 1A) that were compatible with OCT B-scan findings (Figure 2B, top). Fundus autofluorescence showed an area of focal hypoautofluorescence in the macula (Figure 1B). There was no evidence of ischemia or neovascularization based on OCTA imaging, and the left eye appeared normal across all imaging modalities (Figure 2).
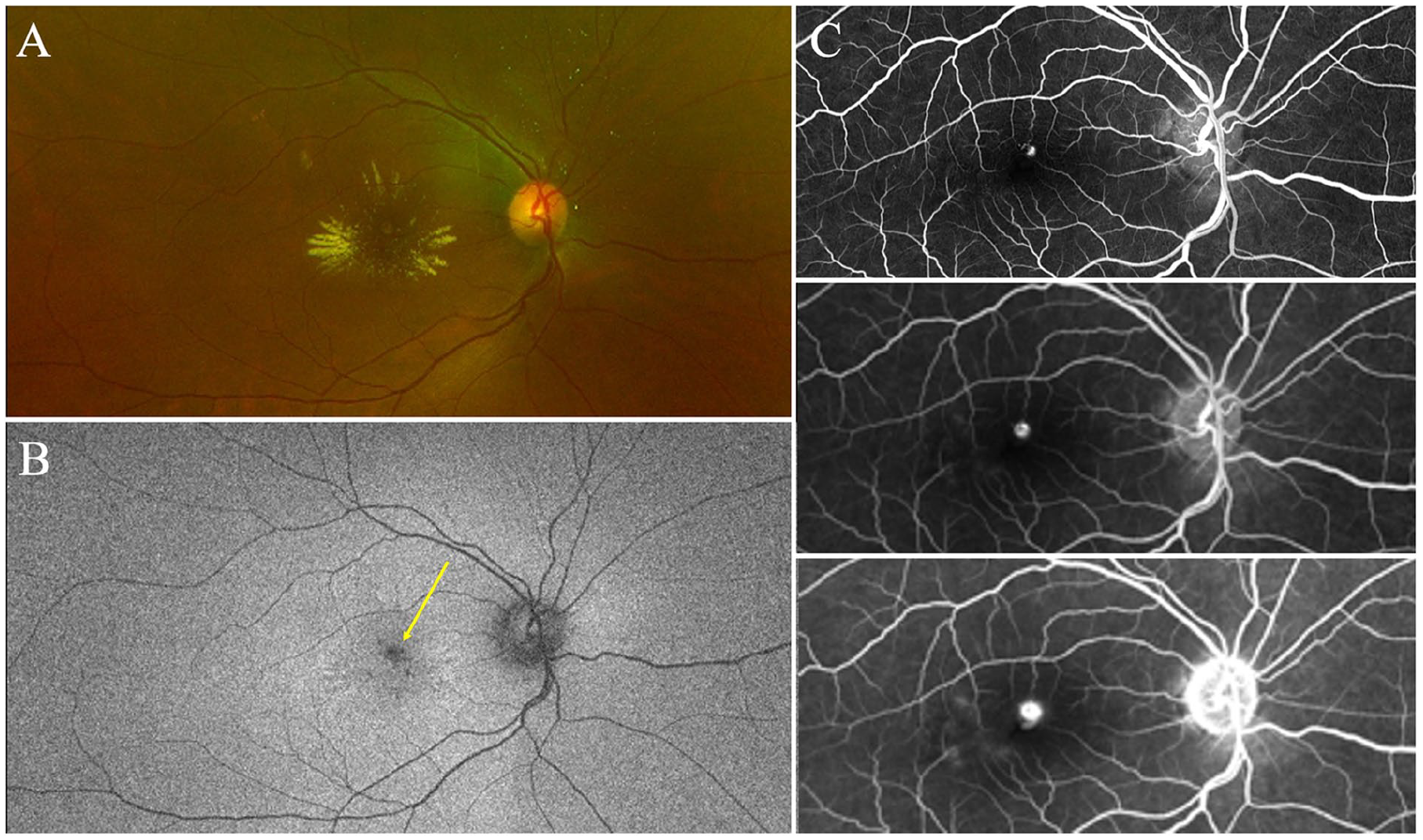
(A) Color fundus image shows extensive intraretinal exudation and edema associated with a roundish perifoveal lesion. (B) Fundus autofluorescence taken at the patient’s initial visit, illustrating extensive edema, exudation, and hypoautofluorescence (yellow arrow). The edema and hypoautofluoresence are most concentrated around the retinal arterial macroaneurysm, located directly superior to the fovea, while the exudates fan out radially. (C) Early-phase (top), midphase (middle), and late-phase (5 minutes) (bottom) intravenous fluorescein angiography performed 4 months after the patient’s initial visit (2 months after 2 injections of aflibercept).
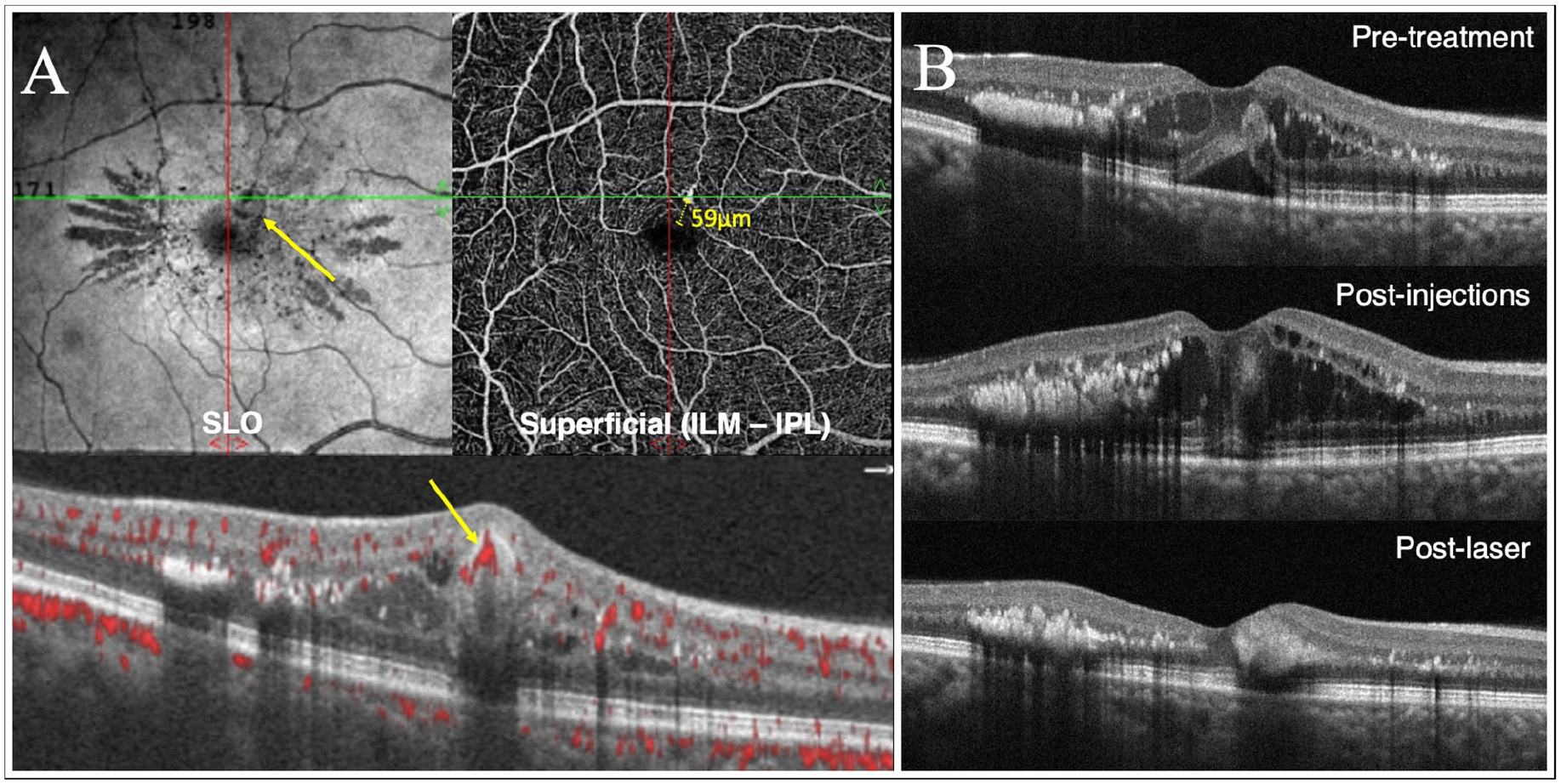
(A) Four weeks after the patient’s second intravitreal injection, optical coherence tomography (OCT) angiography scanning laser ophthalmoscopy and en face (top) images show a small, juxtafoveal retinal arterial macroaneurysm. The retinal arterial macroaneurysm lesion is also seen with blood flow on the OCT B-scan (bottom, yellow arrow) less than 60 µm from the foveal avascular zone. (B) OCT image taken at initial presentation (top), after 2 sequential monthly injections of intravitreal aflibercept (middle), and 1 month after focal laser photocoagulation (bottom).
A tentative diagnosis of CME secondary to an occult BRVO was made. The patient was treated with 2 sequential monthly IVT injections of aflibercept with no visual or anatomic improvement (Figure 2B, middle).
Two months after the final IVT injection, FA imaging showed a small fusiform microcapillary dilation in the foveal center of the right eye, with early pooling and late leakage (Figure 1C). OCT B-scans confirmed the presence of blood flow through the lesion, which was visualized less than 60 µm from the foveal avascular zone (FAZ) (Figure 2A, bottom). The retinal arterial macroaneurysm was seen as a round hyperreflective lesion in the inner retinal layer with associated shadowing on OCT B-scans. Six months after initial presentation, the patient returned to the clinic. A faint threshold burn, but no surrounding burns, was applied with a 532 nm (green) SupraScan laser (Quantel Medical) using the following settings: spot size, 50 μm; laser duration, 0.01 seconds for 5 shots; and power, 80 to 100 mW power until a faint gray burn was achieved.
One month later, resolution of SRF and IRF was seen on OCT B-scans (Figure 2B, bottom), and the BCVA improved to 20/80 OD. There was a significant reduction in exudation and ME, and the central retinal thickness had decreased from 433 μm at the baseline visit to 316 μm. Six months later (approximately 1 year after the patient’s original presentation), results remained stable. Figure 3 shows the postlaser color and autofluorescence images.
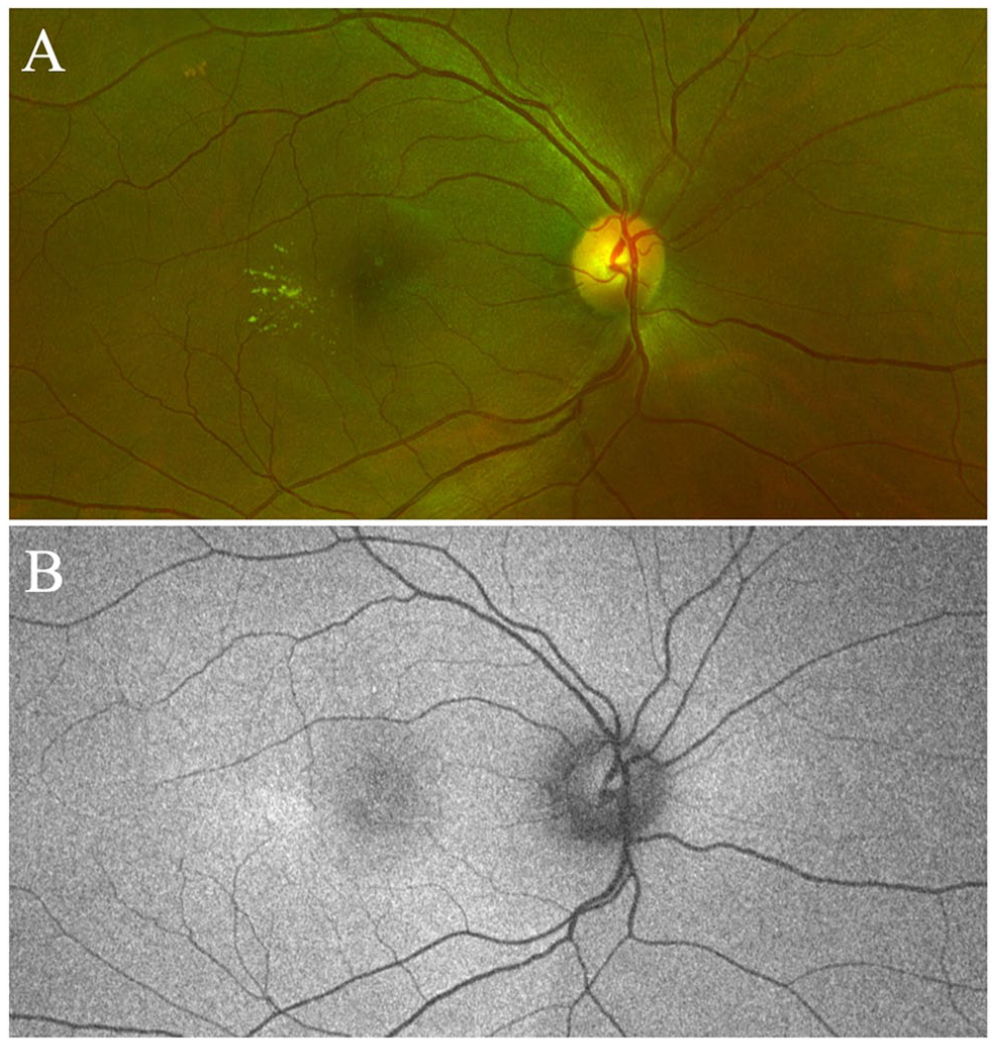
(A) One-year postlaser follow-up. Color fundus photograph shows significant resolution of the exudation and edema discovered at initial presentation. (B) Fundus autofluorescence taken 1 year after the patient’s initial visit and 6 months after focal laser treatment shows the disappearance of the hypoautofluorescent spot with residual exudate temporal to the macula.
Conclusions
We describe a patient presenting with clinical and morphologic features of a retinal arterial macroaneurysm that was found in exceptionally close proximity to the center of the fovea and which was initially mistaken for CME secondary to a BRVO.
CME associated with exudation may represent chronic edema secondary to retinal venous or arterial occlusion, retinal arterial macroaneurysm or, less commonly, neuroretinitis secondary to infectious and inflammatory etiologies. Various clinical characteristics may aid in determining the potential underlying causes of CME. For example, patients with BRVO typically have arteriovenous nicking and dilated tortuous veins in addition to cotton-wool spots, hard exudates, and sectorial retinal hemorrhages that usually do not cross the horizontal raphe. The risk profile is similar to that of patients with retinal arterial macroaneurysm, although BRVO may also be present in hypercoagulable states 8 and delayed filling of the occluded retinal vein in addition to capillary nonperfusion would be seen on FA. CME arising from neuroretinitis is uncommon and typically occurs in younger patients. On initial examination, swelling and flame hemorrhages may be seen surrounding the optic disc. Peripapillary and macular exudates in a star-shaped pattern with cells in the vitreous may also be observed. In addition, SRF and IRF may be noted in the peripapillary region. Patients with neuroretinitis may have a history of recent animal exposure, systemic symptoms, or flu-like prodrome as well as risk factors for Lyme disease, sexually transmitted infections, or tuberculosis. 9
Unlike most retinal arterial macroaneurysms, which are found in the first 3 orders of arterial bifurcations (50% superotemporal and 45% inferotemporal), 6 the location of the retinal arterial macroaneurysm in this case indicates an origin in the terminal arteriolar retinal network. To our knowledge, only 1 other case of retinal arterial macroaneurysm originating in terminal arterioles and located close to the FAZ has been reported. In this case, Menezes et al 10 discovered an acquired juxtafoveal retinal arterial macroaneurysm 400 µm nasal to the foveal center in a 52-year-old man with type 2 diabetes and hypertension. Multimodal imaging demonstrated the hallmark features of a saccular arterial macroaneurysm approximately 250 µm in diameter. Given the proximity of the retinal arterial macroaneurysm to the fovea, the authors avoided direct laser treatment and instead administered 6 monthly IVT injections of ranibizumab. Good anatomic outcomes were achieved, with limited improvement in VA due to the longstanding nature of ME and presumed outer retinal cell loss.
In their case report, Menezes et al 10 hypothesized that a juxtafoveal retinal arterial macroaneurysm is almost always exudative and chronic in nature, even in the absence of hypertension, because of the lower pressure system found in the smaller branches of the retinal arterial vasculature. Our patient also had normal blood pressure and a small paracentral scotoma in the right eye several years previously.
The use of antivascular endothelial growth factor (anti-VEGF) treatment has shown promise in treating exudative retinal arterial macroaneurysms and has been effective in previous reported cases.10,11 Focal embolic damage to arterial walls, potentially leading to localized ischemia, can result from retinal arterial macroaneurysms. In response, VEGF upregulation is activated, in turn stimulating endothelial production of nitric oxide and causing retinal artery dilation and increased permeability.11,12 Anti-VEGF agents decrease leakage and central retinal thickness, consequently improving VA in various neovascular and exudative ocular diseases. Moreover, VEGF inhibition could disrupt the balance between coagulation and fibrinolytic processes, enabling the clearance of hemorrhage in different retinal layers.11,12 These mechanisms are believed to help manage hemorrhagic or exudative complications in retinal arterial macroaneurysms with foveal involvement.
However, not all causes of ME associated with retinal arterial macroaneurysms are solely VEGF-driven. Other molecular pathways, such as inflammatory cytokines, oxidative stress, and other growth factors, may play a more prominent role. Mechanical disruption of the blood–retinal barrier surrounding the aneurysm and the accumulation of blood, exudates, and inflammatory mediators also likely contributes to ME. In such cases, anti-VEGF treatment alone may be insufficient.
The extent, location, and size of intraretinal exudates may also impact visual prognosis. Those especially proximal to the fovea can pose a higher risk to visual function. In addition, larger exudates can lead to widespread disorganization of retinal layers, impeding the natural restoration of anatomic layers, even after resolution of the primary pathology. The presence of extensive exudates can also suggest more widespread inflammation and vascular permeability and may confer a poor anatomic and functional prognosis. In our patient, extensive subretinal and intraretinal exudates were present, leading to a worse visual prognosis resulting from the irreversible photoreceptor damage and morphologic changes in the macula. 3 In addition, there was no anatomic or visual improvement after the first 2 IVT doses of aflibercept; thus, the decision was made to perform low-power focal laser photocoagulation. Laser therapy, has previously been used successfully in the management of ME, alone or combined with anti-VEGF therapy.13,14
Given the multifactorial origin of ME secondary to retinal arterial macroaneurysms, it is plausible that the success with laser therapy in this case was assisted by the background suppression of VEGF through previous IVT injections. These modalities work synergistically to reduce vascular permeability while directly addressing the vascular anomaly. Ongoing injections after laser therapy may also help maintain visual and anatomic gains.13,15
When using laser therapy to treat retinal arterial macroaneurysms, the selection of modality and settings is critical. In our case, the proximity of the retinal arterial macroaneurysm to the fovea required targeted precision to limit collateral damage. Tailoring the 532 nm green laser achieved a faint gray burn without affecting the surrounding tissue. Despite our alterations, the broader discussion of how best to manage retinal arterial macroaneurysms remains diverse. 14 Conventional direct photocoagulation using the argon 532 nm green laser or the 577 nm yellow diode consistently yields positive results in sealing aneurysmal sacs and mitigating exudative symptoms. This approach typically uses large spots (500 µm) with extended exposure (500 ms) to achieve direct lesion burns. 14 However, these settings confer a higher risk for hemorrhage or branch retinal artery occlusion because of the thin walls of the macroaneurysm. The indirect treatment method serves as an alternative, targeting the compromised retinal capillaries around the retinal arterial macroaneurysm and encircling the lesion with laser burns to contain potential hemorrhages.
The introduction of the newer subthreshold micropulse laser has also emerged as a potential solution. Although its exact mechanism is not yet fully understood, prevailing theories attribute its benefits to sublethal retinal hyperthermia, potentiated by heat shock proteins. Studies indicate that the efficacy of subthreshold lasers matches that of their threshold counterparts in retinal arterial macroaneurysm treatments but may offer a reduced risk profile. 16
The use of ancillary imaging in our patient confirmed the proper diagnosis and supported the use of low-power laser photocoagulation, resulting in a significant improvement in BCVA and resolution of the ME. At present, there are no standardized treatment guidelines for symptomatic retinal arterial macroaneurysm. Management decisions, such as observation, anti-VEGF therapies, or laser photocoagulation, should be made on a case-by-case basis, supported by multimodal imaging and in accordance with the patient’s clinical characteristics and goals as well as the physician’s abilities and experience.
This case highlights the valuable role of multimodal imaging, including OCTA and FA, in distinguishing less common presentations of retinal arterial macroaneurysms from ME secondary to other etiologies.
Footnotes
Acknowledgements
We thank the patient for his participation in this study and for providing informed consent for the publication of this case.
Authors’ Note
All authors attest that they meet the current International Committee of Medical Journal Editors criteria for authorship.
Ethical Approval
This case report was conducted in accordance with the Declaration of Helsinki. The collection and evaluation of all protected patient health information were performed in a US Health Insurance Portability and Accountability Act–compliant manner.
Statement of Informed Consent
The patient consented to publication of the clinical history, findings, and images. The patient understands that his name and initials will not be published and that due efforts will be made to conceal his identity but that anonymity cannot be guaranteed.
Declaration of Conflicting Interests
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.