
Abstract
Keywords
Introduction
A lamellar macular hole (LMH) is a retinal disorder with the following 3 diagnostic criteria: irregular foveal contour, a foveal cavity with undermined edges, and apparent foveal tissue loss. 1 Rarely, an LMH spontaneously progresses to a full-thickness macular hole (FTMH), defined as an opening through all layers of the retina at the fovea. 2 This progression may necessitate surgery; however, surgical closure of an FTMH arising from an LMH with pars plana vitrectomy (PPV), traditional internal limiting membrane (ILM) peeling, and gas tamponade reportedly has worse outcomes than similar closure of an idiopathic FTMH. 3 The inverted ILM flap technique might repair FTMHs that are large or refractory to traditional ILM peeling. 4 However, the outcomes of this technique have seldom been reported for FTMHs progressing from LMHs. 5
Here, we present 2 cases of an LMH spontaneously progressing to an FTMH that were treated with PPV, the inverted ILM flap technique, and gas tamponade with good visual outcomes. We also review the literature regarding surgical management of FTMHs arising from LMHs.
Methods
Case Reports
The charts of 2 patients in whom the inverted ILM flap technique was used to treat an LMH spontaneously progressing to an FTMH were retrospectively reviewed. Verbal informed consent was obtained from all subjects before the study.
Literature Search
A literature search of Ovid MEDLINE: Epub Ahead of Print, In-Process & Other Non-Indexed Citations; Ovid MEDLINE Daily; Ovid MEDLINE 1946-Present; and Embase Classic plus Embase was performed through June 5, 2022, without year restrictions. The search strategy was the following: “macular hole” and “lamellar” and “full thickness”. This yielded 329 results. After removal of duplicates, the remaining 198 results underwent title and abstract screening. Thirty-four results underwent full-text screening. Ultimately, 16 studies were included. English-language studies with documented spontaneous LMH progression to an FTMH and surgical management of the resultant FTMH were included. Studies with FTMH formation after surgical intervention for an LMH (ie, iatrogenic FTMH) were excluded.
Data, including age, sex, preoperative best-corrected visual acuity (BCVA), postoperative BCVA, and hole-closure rate, were collected for each included study using Excel software (Microsoft Corp). A chi-square test was used to compare the hole-closure rate between surgical techniques, with P < .05 indicating statistical significance. All mean values are ±SD.
Results
Case Reports
Case 1
A 76-year-old Asian man with a history of cataract was referred for an LMH with epiretinal proliferation in the right eye (Figure 1A). The baseline VA was 20/50. He was regularly followed (Figure 1B). After 1 year of follow-up, the patient presented with spontaneous progression of the LMH to an FTMH (Figure 2A). The VA at the time was 20/150. He had PPV, an inverted ILM flap procedure, and sulfur hexafluoride (SF6) gas tamponade. Intraoperatively, the ILM was peeled, hinged onto the temporal side of the FTMH, and draped over toward the nasal side with gentle tugging of the overlying ILM into the FTMH (Figure 2B). The VA gradually improved from 20/150 preoperatively to 20/70 by the 24-month follow-up visit. The FTMH remained closed (Figure 2C).
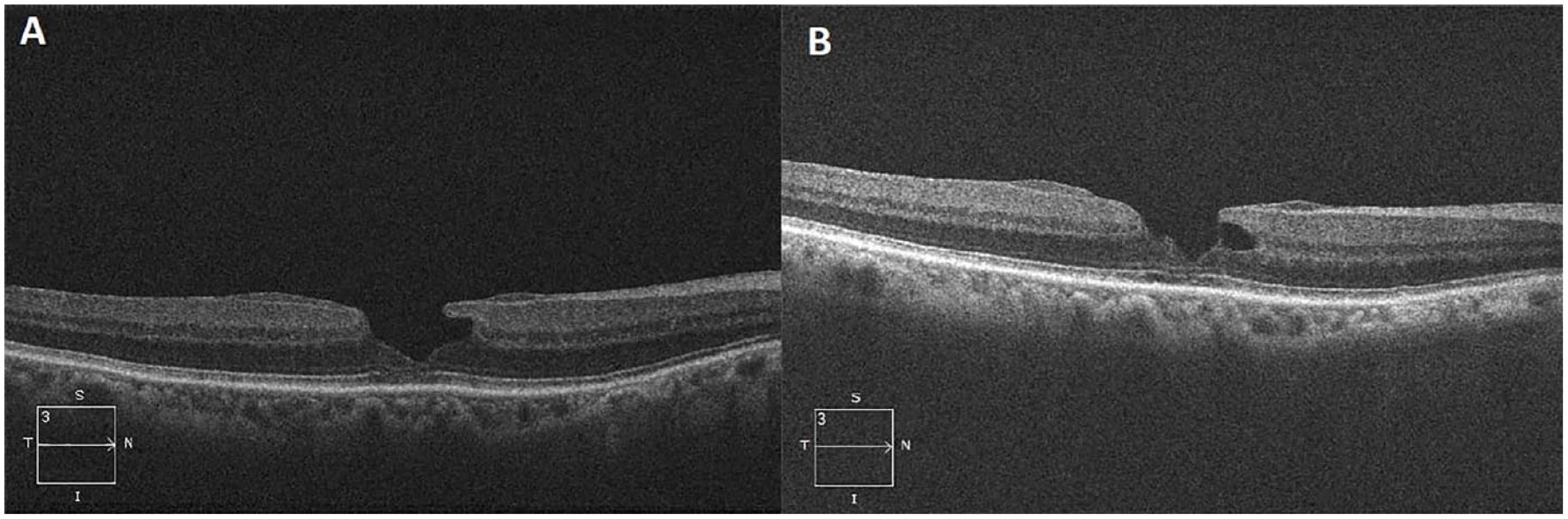
(A) Lamellar macular hole (LMH) with epiretinal proliferation at presentation. (B) LMH during follow-up. There is a subtle subfoveal stress line.
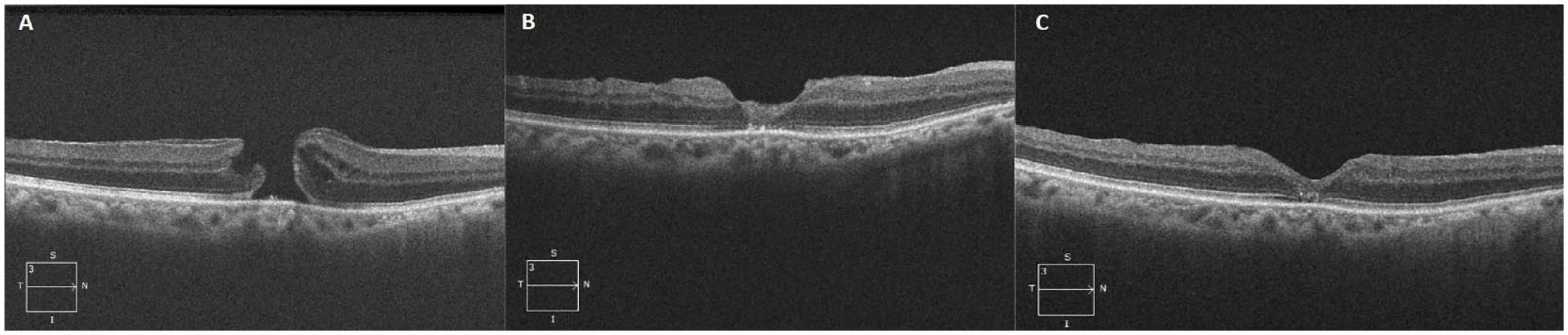
(A) Full-thickness macular hole (FTMH) at presentation. (B) One month postoperatively, a slightly hyperreflective internal limiting membrane is plugging the MH. (C) Two years postoperatively, the FTMH remained closed.
Case 2
A 46-year-old Asian woman with a history of laser in situ keratomileusis in both eyes in 2017 and laser retinopexy for retinal tears in both eyes in 2017 and 2019 presented with an abrupt VA decrease in the right eye. The baseline VA was 20/60. She was found to have a lamellar defect with an FTMH (Figure 3). She also had PPV, an inverted ILM flap procedure, and SF6 gas tamponade. The FTMH remained closed at the 1-month follow-up (Figure 4).
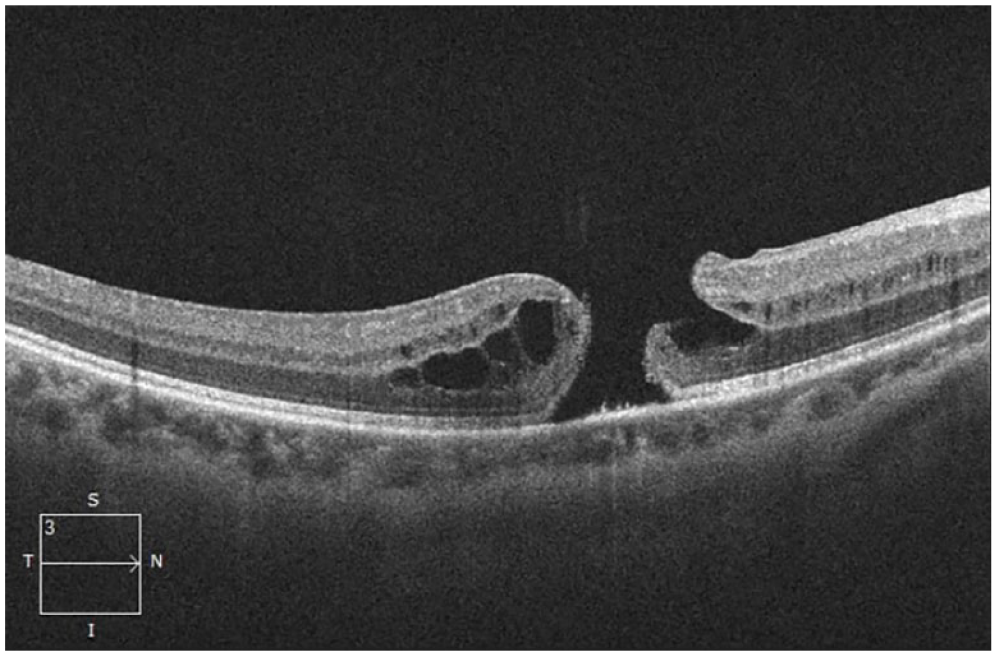
Lamellar defect with full-thickness macular hole at presentation.
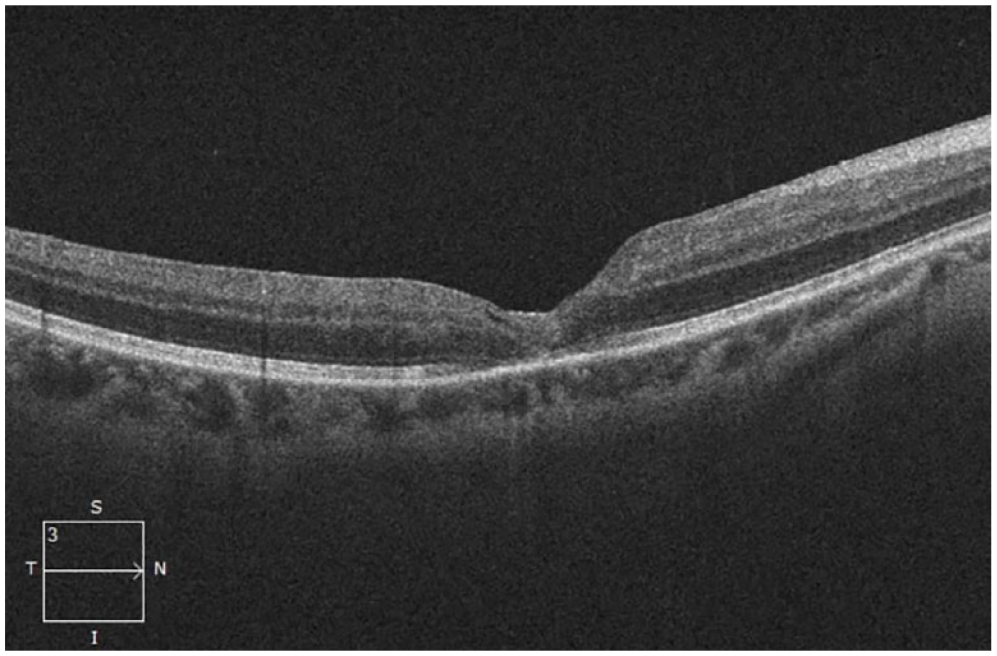
One month postoperatively, the full-thickness macular hole remained closed.
Literature Review: Overall
Sixteen studies2,3,5,6 –18 with a combined sample of 76 eyes (n = 76) were included (Table 1). Thirteen studies2,3,6 –12,14 –17 (n = 40) used ILM peeling, 1 study 5 (n = 32) used inverted ILM flap techniques, and 2 studies13,18 (n = 4) did not specify the surgical technique.
Summary of included studies.
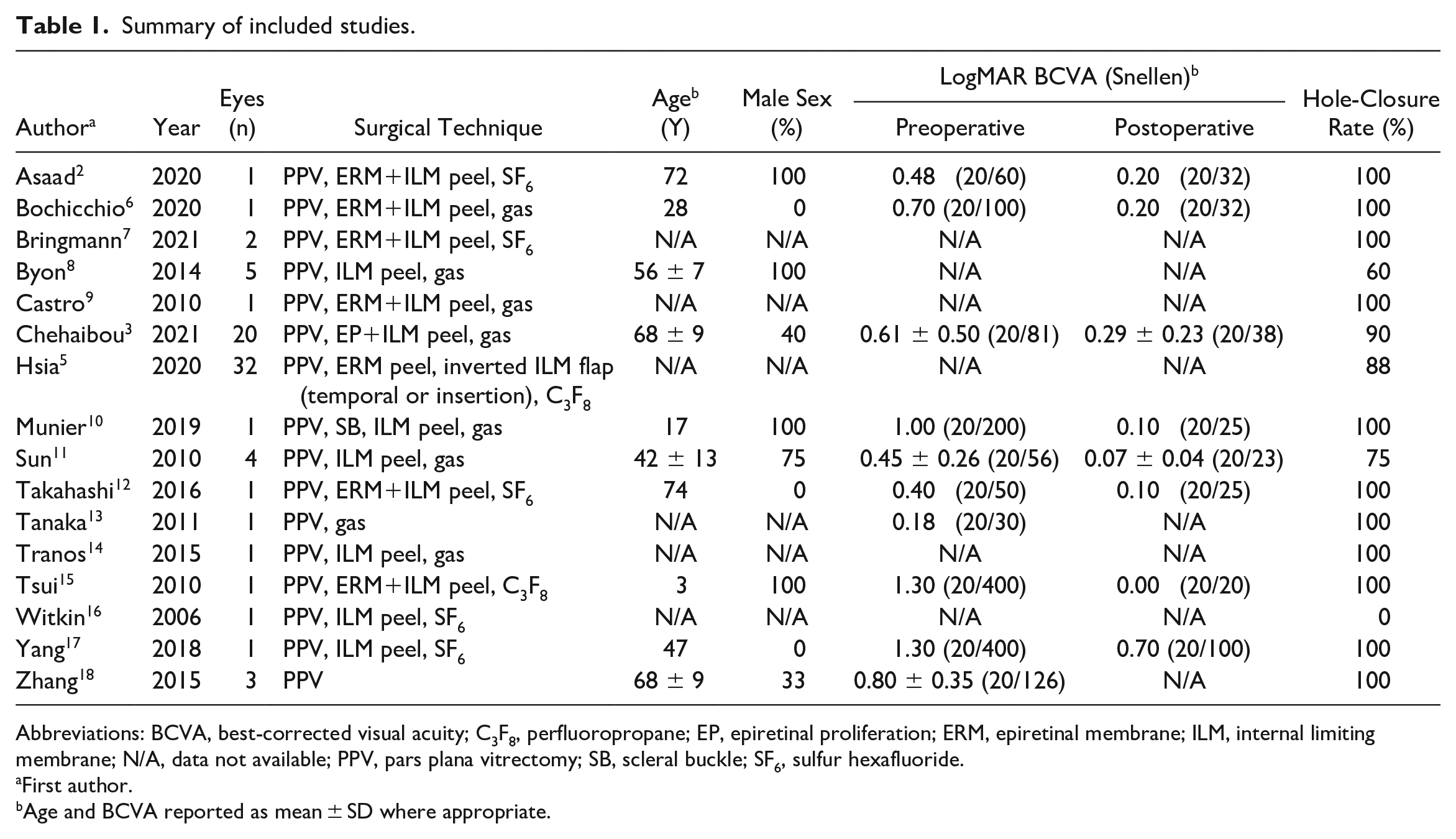
Abbreviations: BCVA, best-corrected visual acuity; C3F8, perfluoropropane; EP, epiretinal proliferation; ERM, epiretinal membrane; ILM, internal limiting membrane; N/A, data not available; PPV, pars plana vitrectomy; SB, scleral buckle; SF6, sulfur hexafluoride.
First author.
Age and BCVA reported as mean ± SD where appropriate.
Literature Review: Internal Limiting Membrane Peeling
Based on the 13 studies using ILM peeling, the hole-closure rate was 85% (34/40). Demographic data were available for 9 studies2,3,6,8,10 –12,15,17 (n = 35) with ILM peeling. These patients had a mean age of 58.5 ± 14.8 years, and 54.3% were men. The BCVA data were available for 8 studies2,3,6,10 –12,15,17 (n = 30) of ILM peeling. The mean BCVA improved from 0.64 ± 0.46 logMAR (Snellen 20/87) preoperatively to 0.25 ± 0.22 logMAR (Snellen 20/36) postoperatively.
Literature Review: Inverted Internal Limiting Membrane Flap
The hole-closure rate in the study using temporal inverted ILM flap or inverted ILM flap insertion techniques 5 was 88% (28/32); however, no specific data regarding age, sex, or BCVA were available. There was no significant difference in the hole-closure rate between ILM peeling and inverted ILM flap techniques (P = .761).
Conclusions
Although infrequent, an LMH may progress to an FTMH, requiring surgical intervention. The most commonly reported repair technique in the literature is ILM peeling with PPV and gas tamponade, which was used in all but 1 study 5 in our review. As stated, in the largest individual study using ILM peeling for 20 cases of FTMHs secondary to LMHs,3 these cases may have relatively poor outcomes, including a lower hole-closure rate (88%) and less BCVA improvement (0.32 logMAR) compared with the results in the literature on ILM peeling for idiopathic FTMHs. Our review supports these findings given the overall hole closure rate of 85% and BCVA improvement of 0.39 logMAR in studies using ILM peeling. However, these determinations are based on limited numbers from retrospective data. Thus, it is important for future prospective studies with large samples to further assess the outcomes of ILM peeling in FTMHs from LMHs.
The authors of the largest study using ILM peeling 3 hypothesized that the relatively poor outcomes may be a result of the loss of central Müller cell cone integrity in LMHs and the subsequent FTMHs. The inverted ILM flap technique may be beneficial in such cases because the flap may create a compartment that prevents fluid in the vitreous cavity from entering the hole, providing a helpful environment and a scaffold for Müller cell proliferation and recovery. In addition, the proteins within the ILM flap may promote Müller cell proliferation and migration, which can lead to expression of neurotrophic factors that contribute to FTMH closure and photoreceptor recovery. 4 This might lead to better vision outcomes via improved foveal tissue recovery. Hence, despite the small size of the FTMHs in our cases, rather than peeling, we draped the ILM flap over the FTMH to use it as a scaffold to simultaneously address the preexisting lamellar defect, which is not present in an idiopathic FTMH, and the resultant FTMH.
In our review, the lone study using inverted ILM flap techniques 5 did not provide data regarding baseline demographics or vision outcomes specifically for their cases of an FTMH arising from an LMH. However, our review found that this study had similar success in terms of the hole-closure rate compared with the studies that used traditional ILM peeling. Also, our illustrative case reports support that this technique can lead to good visual outcomes in addition to successful long-term hole closure, indicating that it may be reasonable to consider inverted ILM flap techniques as an alternative to traditional ILM peeling in cases of FTMHs secondary to LMHs.
Furthermore, the largest ILM peeling study 3 also observed that the resulting FTMH from the LMH had unusual features, such as flat edges and minimal retinal hydration. Characteristics, such as an open, flat formation on optical coherence tomography, are poor prognostic features of closure and may have also contributed to the poor surgical outcomes in that case series. The authors of that study did not postulate on the underlying mechanism resulting in reduced hydration in FTMHs derived from LMHs. This may occur due to the degenerative process of LMHs in which an initial injury disrupts the Müller cell cone at the foveola or fovea wall, resulting in cavitation, which is followed by slow, chronic degeneration of Henle fibers. This degeneration, coupled with an event such as choroidal ischemia, leads to degenerative changes of the outer retinal layers, causing central photoreceptor death along with retrograde degeneration of bipolar and horizontal cells with minimal opportunity for retinal hydration.
This is in comparison with tractional cases in which vitreomacular traction along with unequal epiretinal membrane (ERM) traction results in intraretinal splitting with Müller cell disruption, allowing the buildup of intraretinal fluid. Also, unlike ERMs, epiretinal proliferation exerts minimal traction because of the lack of myofibroblasts. This is supported by our first case, which had epiretinal proliferation indicative of a degenerative LMH, having less intraretinal fluid than our second case, which had traction from a nasal ERM. This is our speculation for the underlying mechanism leading to reduced hydration given that the issue of hole hydration is complex19,20 and the precise factors leading to progression of LMHs to FTMHs are not known.
Furthermore, given that significant vitreous traction is implicated in idiopathic FTMHs, 21 our cases had less hydration than idiopathic FTMHs. This further supports consideration of using the inverted ILM flap technique or possibly an inverted epiretinal proliferation flap technique, which has also shown good anatomic results in cases with epiretinal proliferation, as a potential alternative to traditional ILM peeling for FTMHs arising from LMHs. Prospective studies comparing these techniques in regard to the hole-closure rate and vision outcomes are needed to confirm or refute this hypothesis.
In conclusion, certain features of FTMHs progressing from LMHs, such as loss of foveal tissue, flat hole edges, and limited retinal hydration, may result in there being no major difference between inverted ILM flap techniques and the traditional ILM peeling technique for surgical repair. However, our findings are based on retrospective data with limited sample sizes. Therefore, future prospective studies are needed to elucidate the optimum surgical technique for an FTMH arising from an LMH.
Footnotes
Ethical Approval
Ethical approval was not required for this study.
Statement of Informed Consent
Verbal informed consent was obtained from all subjects before the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.