
Abstract
Keywords
Introduction
Ocular trauma associated with an intraocular foreign body (IOFB) is a significant cause of morbidity, especially in young men of working age. 1 The posterior location and retinal involvement of the IOFB as well as size larger than 3 mm1,2 are important predictors of poor visual outcomes in these types of patients.
An IOFB associated with a posterior perforation presents unique surgical challenges. External suture closure of a posterior defect can be complicated by difficult exposure, particularly in a hypotonus eye. Care must be taken to avoid damage to the macula and optic nerve. Small posterior defects can often be observed only and left to self-seal.3,4 However, larger defects may have to be surgically repaired to maintain adequate intraocular pressure and reduce the risk for hypotony and phthisis. 5 If silicone oil tamponade is indicated, closure of a large posterior wound would likely be necessary to prevent leakage of silicone into the orbit.
Previous approaches for closure of posterior penetrating or perforating injuries include autologous Tenon packing5,6 and ab interno suturing. 7 Posterior radial scleral buckles have also been used in cases of posterior perforating eye injuries to support the wound sites and reduce the rates of retinal detachment. 8 We describe a novel technique for addressing posterior perforating injuries using a 3-layer plug consisting of donor sclera, human amniotic membrane, and fibrin glue.
Case Report
A 21-year-old man presented to our center with bilateral, large, metallic IOFBs that were sustained while hammering a metal railway pin with a maul (Figure 1, A-C). The presenting visual acuity (VA) was 20/400 OS and light perception UD. After informed consent was obtained, the patient was taken to surgery under general anesthesia. For the right eye, suture repair of the laceration in the sclerocorneal junction was performed, after which pars plana vitrectomy, placement of a scleral buckle, removal of the IOFB, endolaser photocoagulation of a peripheral retinal break, fluid–air exchange, and silicone oil tamponade was carried out. The metallic IOFB measured 15 mm × 5 mm × 1 mm and was noted to be protruding slightly from the anterior penetration site near the limbus. It was removed directly with the aid of a 0.3 mm toothed Castroviejo forceps.
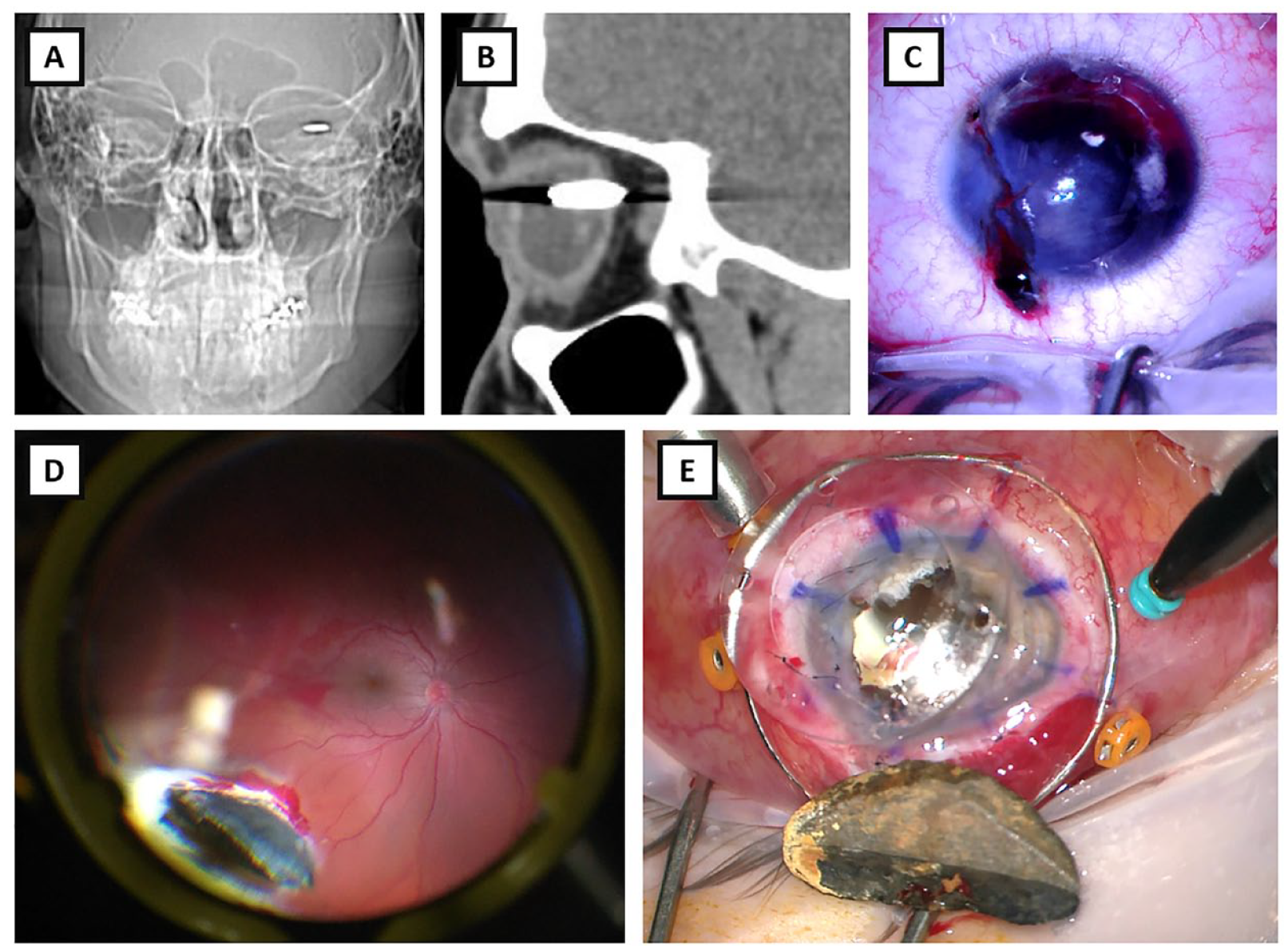
A 21-year-old man presented with a bilateral ocular injury sustained while hammering a railway pin with a maul. X-ray of the skull revealed bilateral orbital foreign bodies (A), and a sagittal section of the orbital computed tomography of the left eye suggested a full-thickness posterior perforating injury (B). Anterior examination revealed a corneal entry wound (C). Intraoperatively, a large metallic foreign body was seen imbedded in the eye wall (D). The 15 mm × 7 mm foreign body was removed through a temporary keratoprosthesis (E).
In the left eye, the posterior segment could not be adequately visualized due to the severity of the corneal trauma, so a penetrating keratoplasty was performed to place an 8.2 mm Landers temporary keratoprosthesis. A 15 mm × 7 mm × 3 mm foreign body was observed to be embedded in the midperipheral posterior eye wall (Figure 1D). This IOFB was lodged in a posterior perforation site, with part of the IOFB inside the globe and part of it protruding through the sclera into the orbit.
Grasping the IOFB proved challenging due to its size and the fact that it was wedged in the scleral perforation. A micro alligator forceps was used to grasp and mobilize the IOFB, an approach that has been previously described for large IOFBs. 9 The IOFB was removed through an open-sky approach after removing the temporary keratoprosthesis (Figure 1E). The keratoprosthesis was thereafter resutured into place.
Upon internal inspection following removal of the IOFB, a full-thickness defect in the posterior eye wall was noted. This was temporal to the macula and measured approximately 6 mm × 2 mm (Figure 2A). There was a surrounding localized retinal detachment. A limited retinectomy was performed to remove incarcerated tissue and necrotic retina bordering the defect. It was felt that silicone oil tamponade would be required to optimize the chances for retinal reattachment. However, there was concern that the silicone oil would simply migrate through the posterior defect and into the orbit.
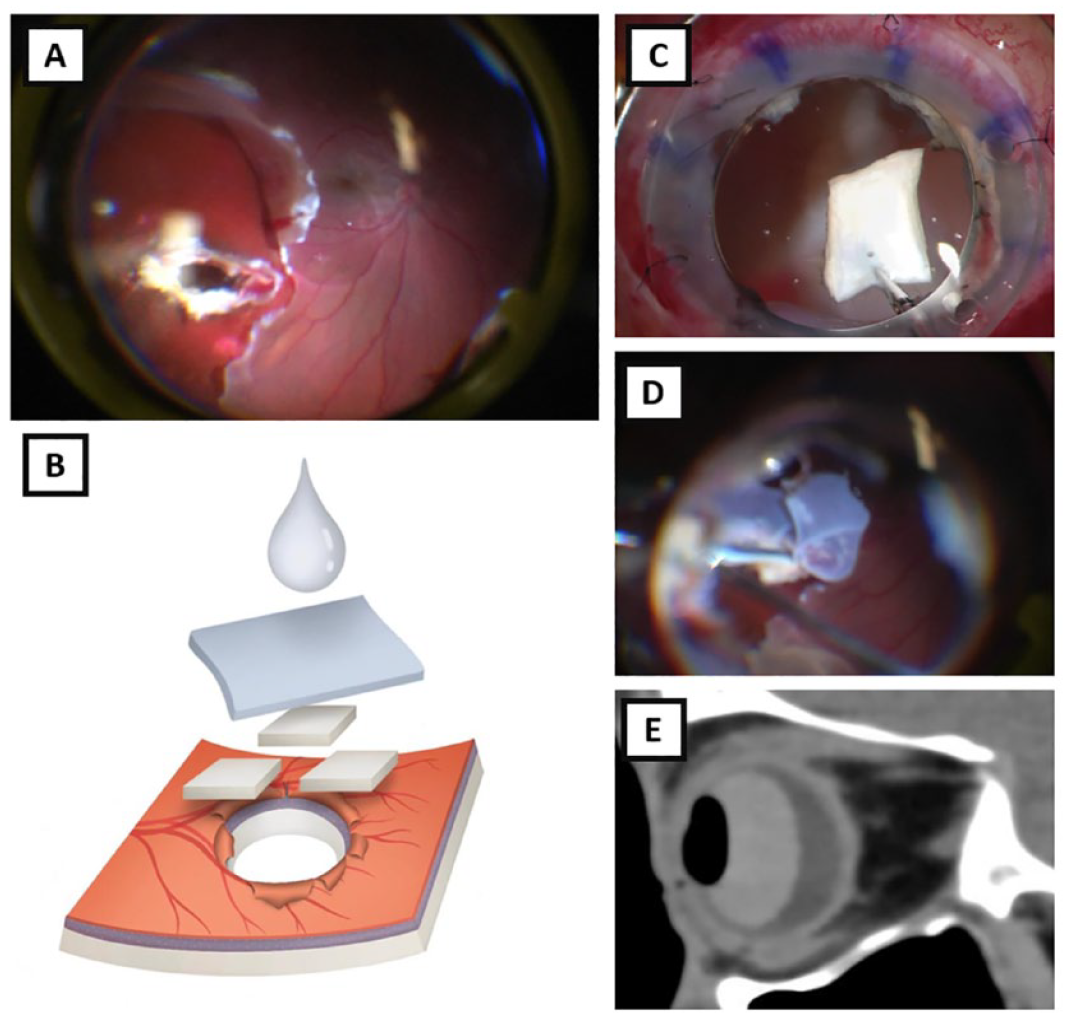
After removal of the foreign body, an approximate 6 mm × 2 mm defect was found in the posterior eye wall (A). The defect was filled with a 3-layer plug (B) consisting of donor sclera (C), amniotic membrane (D), and fibrin glue. Following silicone oil tamponade, the postoperative examination revealed an 85% silicone oil fill and computed tomography confirmed the presence of intraocular oil with no oil in the orbit (E).
To fill the defect, a section of donor sclera measuring approximately 2 mm × 2 mm was first introduced into the eye via the edge of the keratoprosthesis and packed into the wound (Figure 2C). This was repeated with four 2 mm × 2 mm pieces of donor sclera until the internal volume of the defect was adequately filled. Next, a sheet of human amniotic membrane (AmnioGraft, BioTissue Inc) measuring 6 mm × 4 mm was tucked into the opening to fill any gaps (Figure 2D). Finally, following fluid–air exchange, fibrin glue (Artiss Fibrin Sealant, Baxter International) was administered to the defect to secure the donor sclera and amniotic membrane layers (Figure 2B). After the surrounding retinal breaks were treated with endolaser, the eye was filled with silicone oil (5000 centistoke), and the temporary keratoprosthesis was replaced with a donor corneal button.
On postoperative day 1, computed tomography imaging confirmed that there was no oil migration into the orbit (Figure 2E). Unfortunately, the final VA in the left eye was limited due to proliferative vitreoretinopathy (PVR) and recurrent retinal detachment.
Conclusions
Traumatic IOFBs complicated by posterior perforating injuries can lead to significant vision loss, and surgical repair is often challenging.
A full-thickness posterior defect can serve as a point of egress for intraocular vitreous substitutes. Ab interno suture closure of a posterior penetrating injury has been described to address this issue. Schmidt et al 7 presented a case of a 3 mm posterior pole scleral perforation caused by a metallic splinter, which was closed using 10-0 nylon suture introduced via a sclerotomy into the vitreous cavity and tied with an intraocular forceps. This technique is technically complex and may induce bleeding from the needle entry points. Furthermore, suture closure of a large defect may require significant traction to approximate the wound edges and could distort the surrounding tissue.
Ma et al 5 used autologous Tenon capsule to plug a posterior defect from a perforating metallic foreign body. They noted that the initial Tenon graft was too soft to patch the hole and was washed into the orbit by the flow of fluid. The 3-layer plug using donor sclera, a sheet of human amniotic membrane, and fibrin glue described in the present study may provide a more robust plug.
PVR and retinal redetachment are common sequalae of intraocular bodies, especially in younger patients. 1 While it is possible that the introduction of the 3-layer plug in our case promoted PVR formation, human amniotic membrane has been used intraocularly in other instances, such as for macular hole repair, 10 retinal detachment, 11 optic disc pit maculopathy (ODPM), 12 and a choroidal patch. 13 Fibrin glue 14 and scleral patch graft15,16 have also been used in ODPM.
Hence, this 3-layer plug technique provides surgeons with a novel approach for repairing challenging traumatic posterior perforating injuries, particularly when silicone oil tamponade is indicated. The efficacy and safety of this method should be further validated in similar cases.
Footnotes
Authors’ Note
A video of this case was presented at the American Society of Retina Specialists Film Festival under the title “Heavy Metal: XL Edition.”
Ethical Approval
Institutional review board approval was not required.
Statement of Informed Consent
Written informed consent for publication of this paper was obtained from the patient.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.