
Abstract
Purpose:
This work reports a rare case of spontaneous suprachoroidal hemorrhage (SSCH) and summarizes the literature on its treatment options and outcomes.
Methods:
A case report and comprehensive literature review are presented on the medical and surgical management of SSCH on PubMed from 1998 to 2021.
Results:
The literature search revealed 58 studies, 33 of which included 52 eyes of 47 patients. Surgical treatment typically consisted of choroidal drainage with posterior sclerotomies combined with pars plana vitrectomy and silicone oil placement. Medical therapy involved intraocular pressure control with laser peripheral iridotomy and topical, oral, and intravenous medication.
Conclusions:
In cases of SSCH, conservative management and a prompt workup should be initiated to identify the cause before proceeding with surgery. If the initial workup does not reveal a cause, medical and surgical treatments are both viable and the decision is at the discretion of the treating physician.
Keywords
Introduction
Suprachoroidal hemorrhage (SCH) is a rare but vision-threatening complication of intraocular surgery and trauma whereby extensive hemorrhaging in the potential space between the choroid and sclera mechanically brings the retina into near or complete apposition and in severe cases, extrudes intraocular contents through open wounds. 1 Suprachoroidal hemorrhage typically occurs secondarily to intraocular surgery, both intraoperatively and postoperatively, and in patients experiencing physical trauma. 1
Although rare, SCH has also been described to occur spontaneously but typically occurs in association with specific ocular or systemic risk factors.1,2 Commonly encountered systemic risk factors include old age, increased venous pressure during the Valsalva maneuver and coughing, hypertension, and the use of antiplatelets, anticoagulants, and thrombocytopenia. Intraocular risk factors include high myopia, acute hypotony, glaucoma, and choroidal lesions, such as hemangiomas and melanoma.2,3
Indications for drainage of an appositional SCH include central choroidal apposition, a flat anterior chamber, associated retinal detachment, uncontrolled elevated intraocular pressure (IOP), and severe pain. 4 In nonappositional cases, surgical and conservative approaches with frequent monitoring of hemorrhage absorption have been well described. 5
In this report and review of the literature, we describe a case of spontaneous suprachoroidal hemorrhage (SSCH) with near apposition of the retina in a patient with thrombocytopenia secondary to type 1 chronic myeloid leukemia and lymphoplasmacytic lymphoma that was successfully treated with conservative therapy and close monitoring. Our case illustrates the importance of a prompt systemic workup as well as a multidisciplinary approach to the management of SSCH before planning surgical intervention.
Methods
Case Report
An 84-year-old White man with sudden-onset right-sided eye pain and vision loss presented to the emergency department. On initial assessment, the IOP in the right eye was 70 mm Hg, which prompted a referral to the glaucoma service. Maximum medical therapy consisting of oral acetazolamide and topical brimonidine, dorzolamide, and timolol was promptly initiated, and a peripheral iridotomy in the superior iris was performed that resulted in normalization of IOP. Posterior segment examination by the glaucoma team revealed an elevated retinal lesion in the affected eye. Therefore, the patient was referred to the retina service for further management and follow-up.
The visual acuity (VA) at the time of presentation was light perception OD with an IOP of 21 mm Hg. Anterior segment examination of the right eye revealed conjunctival chemosis, 3+ corneal edema with pigment deposition on the corneal endothelium, and an iris at near iridocorneal apposition centrally at risk of touch. Fundoscopy of the affected eye revealed a dome-shaped elevation of the retina with near apposition. Anterior segment examination and fundoscopy of the fellow eye confirmed previous retinal detachment repair and a reattached retina. A B-scan ultrasound confirmed near appositional suprachoroidal hemorrhage in the right eye (Figure 1).
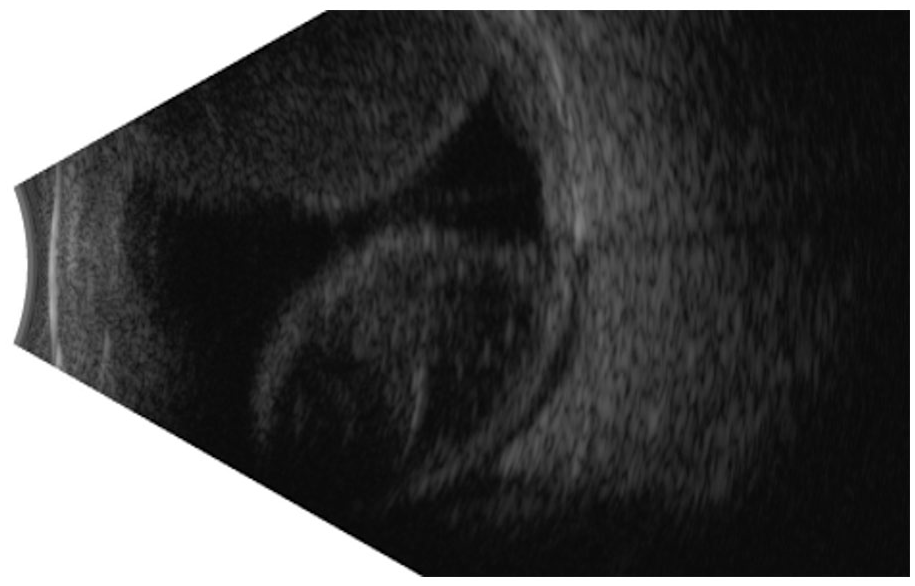
B-scan revealing a near appositional dome-shaped choroidal elevation in keeping with choroidal hemorrhage in the suprachoroidal space.
The patient was treated with a single 0.5 mL dose of sub-Tenon triamcinolone and was scheduled for urgent surgery. A prompt investigation was initiated given the spontaneous onset of the hemorrhagic choroidal detachment, which revealed thrombocytopenia with a platelet count of 75 × 109/L. A complete workup found a medical history significant for type 1 chronic myeloid leukemia and lymphoplasmacytic lymphoma in remission. Surgical management was deferred because of the risk of a further or new hemorrhage that could permanently compromise vision. Hematology and oncology were consulted to manage the thrombocytopenia.
One week after the initial presentation, the VA in the affected eye was hand motion and the IOP was 12 mm Hg with a reduced risk of apposition. Two weeks after the initial presentation, the VA was counting fingers, the IOP was within normal limits, and there was a further decrease in choroidal elevation (Supplemental Figure 1). At this point, the platelet count had increased from 75 × 109/L to 131 × 109/L. Four weeks after the initial presentation, the VA was 20/200, the choroidal elevation had substantially reduced (Supplemental Figure 2), and the posterior pole was visible. At this point, a collection of residual subfoveal fluid was still visible (Supplemental Figure 3). Six weeks after the initial presentation, the VA was 20/100 and the SSCH had completely resolved (Figure 2). The collection of subfoveal fluid had almost completely resolved (Supplemental Figure 4).

Complete resolution of suprachoroidal hemorrhage after 6 weeks of follow-up.
Search
A comprehensive search of PubMed from 1998 to 2021 using the keywords and MeSH terms “spontaneous” “hematoma” “hemorrhage” and “suprachoroidal” was performed. Case reports and case series of patients who developed SSCH with a history of intraocular surgery within the past 3 months except for laser iridotomy were excluded. Patient demographics, risk factors, presumed etiology, management, and visual outcomes were abstracted from the selected records (Table 1).
Basic Characteristics of Included Studies.
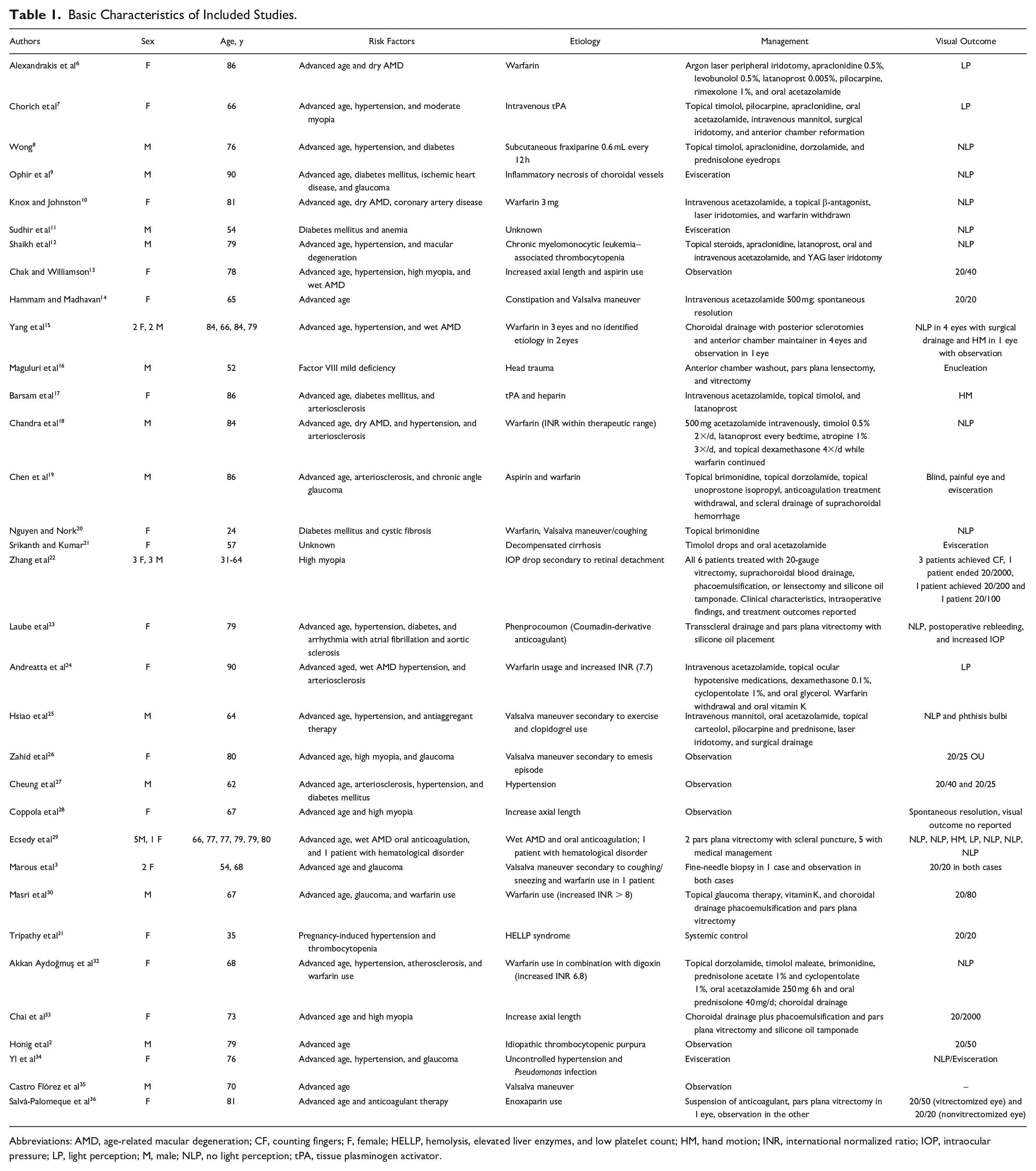
Abbreviations: AMD, age-related macular degeneration; CF, counting fingers; F, female; HELLP, hemolysis, elevated liver enzymes, and low platelet count; HM, hand motion; INR, international normalized ratio; IOP, intraocular pressure; LP, light perception; M, male; NLP, no light perception; tPA, tissue plasminogen activator.
Results
The literature search revealed 58 studies; after a careful review of the literature, all cases with a recent history of any ocular surgery or procedure were excluded. Of those 58 studies, 33 were included after the exclusion criteria were confirmed. These 33 studies, comprising 52 eyes of 47 patients, were included in the review (Table 1). All cases except 5 were unilateral. The most reported systemic risk factors for SSCH included advanced age followed by hypertension, diabetes mellitus, and arteriosclerosis. In terms of ocular risk factors, high myopia with an increased axial length and open-angle glaucoma were commonly reported. The use of anticoagulants, antiplatelets, and thrombolytic medication as well as performing the Valsalva maneuver were the most prevalent etiologies for SSCH.
The most common cause of SSCH in this review was warfarin use, even in patients with an international normalized ratio (INR) within therapeutic range and in patients with supratherapeutic INR values. These patients were typically treated through surgical choroidal drainage with posterior sclerotomies combined with pars plana vitrectomy with silicone oil placement tamponade. Medical therapy consisted of control of the IOP with topical, oral, and intravenous medication and neodymium:YAG laser peripheral iridotomy. In cases in which anticoagulant therapy was the etiology, medication discontinuation was the standard practice pattern. For patients with supratherapeutic INR, reversal therapy with vitamin K was applied.
Of the 52 eyes, 3 (5.8%) required immediate evisceration because of expulsive suprachoroidal hemorrhage. Of the remaining 49 eyes, the final visual outcomes were reported in all but 2 cases. Overall, 26 of 47 eyes received conservative treatment and 21 of 47 received surgical management. Two of 21 (9.5%) eyes in the surgical group and 1 of 26 (3.8%) in the medical group required a secondary evisceration/enucleation during treatment. Eyes in the surgical and medical group had a similar likelihood of achieving a final VA of no light perception (NLP), with a rate of 9 of 21 (43%) and 11 of 26 (42%) in the 2 groups, respectively. Patients in the medical group had a higher likelihood than those in the surgical group of achieving a final VA better than 20/80, with a rate of 11 of 26 (42%) and 2 of 21 (9.5%), respectively.
Conclusions
SSCH is a rare but devastating complication that is associated with poor visual outcomes. Hematological factors such as blood dyscrasias, anticoagulation, and antithrombotic therapy are serious risk factors that predispose patients to SSCH in many cases.2,21,30 The literature on the management and visual outcomes in patients with an SSCH is limited to individual case reports. Previously reported cases of SSCH in patients with chronic myelomonocytic leukemia have ended in an NLP visual outcome.12,29 To our knowledge, we are the first to describe SSCH in a patient with type 1 chronic myeloid leukemia and lymphoplasmacytic lymphoma who achieved a good visual outcome with conservative management.
In our review, a larger percentage of patients in the medical management group obtained a VA greater than 20/80 and a smaller percentage required secondary evisceration. Surgical management of SSCH is usually recommended in cases with choroidal apposition because of the high likelihood of complications such as acute angle-closure glaucoma. If a surgical intervention is pursued, performing the surgery 7 to 14 days after the initial presentation is preferred to allow adequate time for any blood clots to lyse before evacuation.23,37 During the period before surgery, the SCH can be closely observed using B-scan. Different surgical approaches, including radial sclerotomies, a transconjunctival approach with the use of trocar cannulas, and active drainage with a guarded needle, are commonly used by anterior and posterior segment surgeons. 37
Unfortunately, although surgical management of SSCH has shown good results in IOP control, the visual outcome is usually poor. 25 Several studies have reported poor visual outcomes after surgical drainage in cases of SSCH. Laube et al 23 reported a case with final vision of NLP after surgical drainage and vitrectomy in a patient with choroidal apposition secondary to SSCH. Despite the complete resolution of the SCH in this report, a pale optic nerve head secondary to an elevated IOP and chorioretinal fibrosis resulted in the poor outcome.
Our review of the literature suggests a strong association between anticoagulation and the risk of SSCH. Therefore, it is important to investigate the use of oral anticoagulation and the INR values in the assessment of patients presenting with SSCH. 38 The anatomic resolution of SSCH with surgical drainage is possible; however, rebleeding within 1 week or even 2 months of intervention has also been documented. To prevent rebleeding, it is important to correct the underlying cause, such as stopping anticoagulants or giving the patient a platelet transfusion. Yang et al 15 reported 2 cases of rebleeding after surgical drainage in a case series of 5 patients on warfarin.
In the present case, the decision was made to pursue a conservative approach to treat the SSCH because of the resolution of the angle-closure glaucoma and the patient’s history of a myeloproliferative disorder. With the help of the hematology team, we were able to normalize the patient’s thrombocytopenia to prevent rebleeding. In addition, we used corticosteroids in the periocular and sub-Tenon space to reduce the inflammation cascade following the hemorrhage. Steroids can also play a role in platelet activation to prevent rebleeding. 39
Majoor et al 40 found that after a course of 10 days with oral prednisone (0.5 mg/kg/day) treatment, there was an increase in von Willebrand factor (VWF) in healthy individuals. The increased VWF levels after steroid therapy might be beneficial in patients with SSCH because it can promote platelet adhesion and contribute to faster stoppage of active bleeding. Different pathways have described the effect of VWF on platelet adhesion. 41 Although steroids might certainly affect platelet adhesion, as Majoor et al’s work indicates, if a benefit exists, it is uncertain that enhancing platelet adhesion is the primary reason considering that ongoing bleeding is an uncommon issue by the time the patient presents for treatment. However, platelet activation after the initial bleeding might prevent rebleeding, promoting faster spontaneous resolution, as in our case, or preventing rebleeding in the intraoperative or postoperative period.
Our case report and the literature review demonstrate that in selected patients with SSCH and thrombocytopenia related to myeloproliferative disorders, conservative management with corticosteroids and close observation can achieve an excellent final visual outcome. To our knowledge, the present paper is the first in the literature to provide a hypothesis regarding the potential therapeutic mechanism of localized steroids in the management of SSCH. Moreover, the evidence provided by our review emphasizes the importance of a systemic workup in patients with an SSCH to identify and reverse the cause of bleeding. Evaluating a possible steroid benefit effect related to platelet function and the benefit of reversal of oral anticoagulation in patients with an SSCH would require a prospective multicenter randomized trial to assess the likelihood of rebleeding after surgical drainage or secondary bleeding after reversal of anticoagulation and to confirm our proposed theory on the benefit of steroids in patients with an SSCH. A prospective multicenter randomized trial would elucidate a cause effect in terms of the therapeutic role of the steroids and would also provide insight regarding the more beneficial approach for this entity, either surgically or with medical therapy.
A systemic workup and investigation before surgery could provide the surgeon with clinical information that will ultimately protect the patient from the risk of rebleeding and protect the surgeon from devastating outcomes secondary to expulsive hemorrhage.
Supplemental Material
sj-docx-1-vrd-10.1177_24741264221074799 – Supplemental material for Massive Spontaneous Suprachoroidal Hemorrhage in a Patient With Type 1 Chronic Myeloid Leukemia and Lymphoplasmacytic Lymphoma: Case Report and Review of the Literature
Supplemental material, sj-docx-1-vrd-10.1177_24741264221074799 for Massive Spontaneous Suprachoroidal Hemorrhage in a Patient With Type 1 Chronic Myeloid Leukemia and Lymphoplasmacytic Lymphoma: Case Report and Review of the Literature by Miguel Cruz-Pimentel, Parsa Mehraban Far, Michael H. Brent and Peng Yan in Journal of VitreoRetinal Diseases
Footnotes
Ethical Approval
This report was conducted in accordance with the Declaration of Helsinki. The collection and evaluation of all protected patient health information was performed in a HIPAA (Health Insurance Portability and Accountability Act)–compliant manner.
Statement of Informed Consent
Informed consent was obtained before collection of images, including permission for publication of all photograph and images included herein.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material is available online with this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.