
Abstract
Purpose:
This work reports unusual peripheral vascular anomalies on ultra-widefield angiography in a case of idiopathic macular telangiectasia (IMT) type 1.
Methods:
A case report is discussed.
Results:
A 51-year-old woman with a 6-year history of IMT type 1 presented with ongoing vision symptoms from persistent macular edema despite extended antivascular endothelial growth factor therapy. Examination and macular imaging findings were consistent with a diagnosis of IMT type 1, and ultra-widefield angiography additionally demonstrated nonperfusion, terminal vascular loops, and arteriovenous anastomosis without exudation or telangiectasis. The patient’s condition remained stable after she elected observation.
Conclusion:
While extrafoveal vascular anomalies are a known feature of IMT type 1, they commonly consist of peripheral telangiectasias and exudation. Describing new peripheral vascular abnormalities in IMT adds to our knowledge of this condition and could be of value for diagnosis, management, and further study.
Introduction
The advent of ultra-widefield (UWF) retinal imaging, which allows for recording up to 220°of the retina, provides opportunities to better characterize peripheral findings in retinal pathologies. 1 Recent studies using UWF angiography (UWFA) have observed that peripheral retinal abnormalities—such as microaneurysms, right-angled vessels, and terminal networks—are noted even in healthy eyes. 2 The cause of peripheral vascular changes in retinal diseases is not fully understood, but the perfusion status of the retina is believed to be associated.
Idiopathic macular telangiectasia (IMT) type 1, also termed aneurysmal telangiectasia, is characterized by unilateral, easily visible macular telangiectasis that occurs predominantly in middle-aged men. Subsequently, macular edema (ME) can result in vison impairment. Approximately one-third of the IMT cases are associated with focal telangiectasias with or without exudation in extramacular locations. 3 However, there are limited reports of peripheral retinal vascular abnormalities on UWF imaging and UWFA in IMT type 1. Herein we present a unique case of IMT type 1 with intriguing peripheral UWFA findings, including retinal nonperfusion, arteriovenous anastomosis, and terminal vascular loops.
Methods
Case
A 51-year-old White female was referred for decreased vision in her left eye due to persistent ME secondary to IMT type 1 that was diagnosed 6 years prior. Her ME had failed to resolve after a prolonged course of ranibizumab therapy (20 monthly injections), focal laser, and a subsequent trial of aflibercept (monthly for 4 months). Her ocular history was significant for a left-eye superotemporal retinal hole secondary to posterior vitreous detachment, which had been treated with laser retinopexy. There was no history of diabetes, ocular trauma, retinal vein occlusion, prematurity, low birth weight, or high myopia.
Results
On assessment, her best-corrected visual acuity was 6/4.5 –1 in the right eye and 6/18 +2 in the left eye. Intraocular pressures and anterior segment examination were unremarkable. The right macula and peripheral retina were normal. Telangiectasia with exudation in the superior parafoveal area was appreciated in the left eye. Peripheral retinal examination revealed pigmented laser scarring and a temporal area suspicious for nonperfusion.
In the left eye, optical coherence tomography showed ME, exudates, and degenerative cystic cavitations in the fovea. Vascular complex telangiectasias were appreciated on optical coherence tomography angiography (Figure 1). Left-eye UWFA showed macular telangiectasias with late leakage (Figure 2) and temporal peripheral nonperfusion with abnormal vasculature, including terminal vascular loops and arteriovenous anastomosis (Figure 3). No peripheral telangiectasias or exudate were noted. Multimodal imaging of the right macula and peripheral retina was normal.
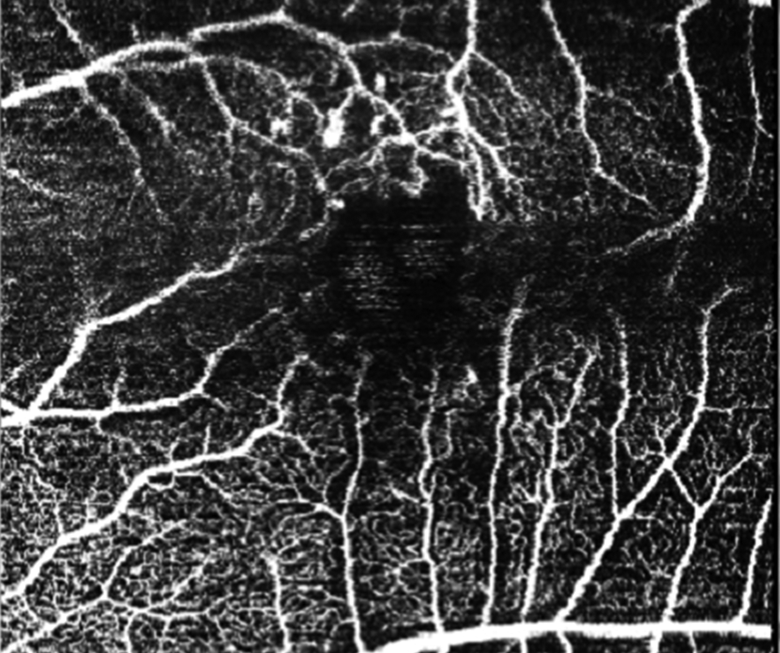
Left-eye optical coherence tomography angiography (Heidelberg Spectralis, Heidelberg Engineering) of the superficial capillary plexus demonstrates superior parafoveal capillary telangiectasias. Image artifacts precluded the assessment of the foveal avascular zone.
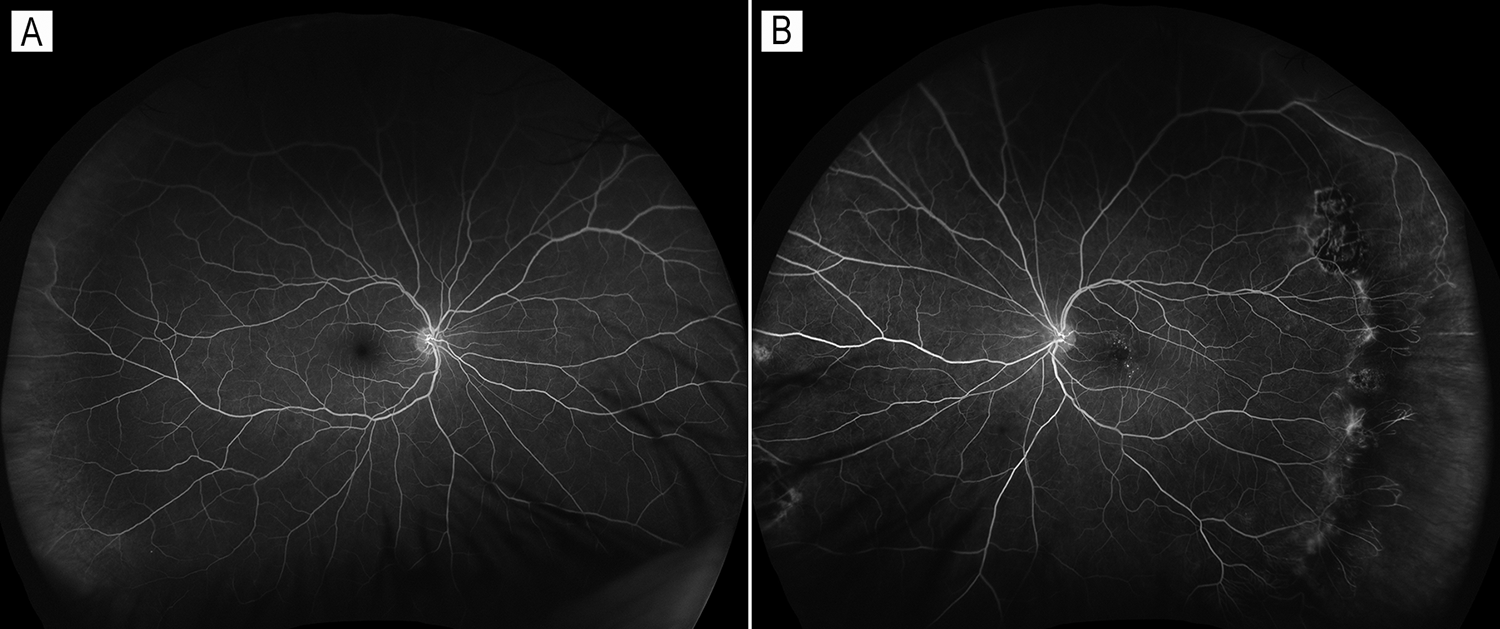
Optos ultra-widefield fluorescein angiography in the late venous phase of each eye. (A) Unaffected right eye. (B) In the affected left eye, perifoveal capillary telangiectasis is noted. Ultra-widefield fluorescein angiography shows peripheral laser scars at 2 o’clock and temporal peripheral vasculature abnormalities (see expanded Figure 3). Vascular changes in the peripheral inferonasal area were also noted. However, assessment of this area was limited by image artifacts.

Enlarged view of the peripheral left retina in the late venous phase. Marked peripheral nonperfusion, arteriovenous anastomosis (arrowheads), and terminal vascular loops (arrows) are noted.
The patient underwent systemic investigations to rule out other etiologies of peripheral retinal nonperfusion. Erythrocyte sedimentation rate, rheumatoid factor, glycated hemoglobin A1c level, liver function test results, electrolyte panel, and serum creatinine level were all normal. Complete blood count showed mild normocytic anemia. Serum protein electrophoresis did not suggest a monoclonal pattern, and the hemoglobin electrophoresis pattern was normal. Syphilis immunoglobulin G antibody testing was nonreactive. Therefore, other causes of retinal nonperfusion, including diabetic retinopathy, myopic degeneration, hyperviscosity syndromes, branch retinal vein occlusion, retinopathy of prematurity, hemoglobinopathies, and inflammatory diseases, were ruled out based on history, examination, and testing.
Therapeutic options were discussed with the patient, including observation, intravitreal triamcinolone, antivascular endothelial growth factor (anti-VEGF) therapy, focal laser, and peripheral photocoagulation. She opted for observation, and her vision and ME remained stable on subsequent follow-up 8 months later.
Discussion
In 1982 Gass and Oyakawa first proposed the entity of idiopathic juxtafoveolar telangiectasis, 4 which has been most recently reclassified by Yannuzzi et al as IMT type 1 (aneurysmal telangiectasia) and IMT type 2 (parafoveal telangiectasia). 3 IMT type 1 is believed to be of developmental origin and is characterized by dilation of the juxtafoveal retinal capillaries in the superficial and deep capillary plexuses. Over time, abnormal capillaries allow leakage of lipid and serous exudate. IMT type 1 is regarded to be an entity within the spectrum of Coats disease. 5,6 Coats disease is an idiopathic retinal vascular disorder characterized by telangiectasia associated with intraretinal and/or subretinal exudation and frequent exudative retinal detachment. 7 Unlike IMT type 1, Coats disease most often presents in childhood and telangiectasias within the macular region is observed in only 1% of cases.
UWF imaging systems have led to the identification of peripheral retinal abnormalities in healthy eyes 8 and in a wide range of retinal diseases including uveitis, 9 diabetic retinopathy, 10 pathologic myopia, 11 inherited retinal diseases, 12 and retinal vein occlusion. 13 Detecting peripheral nonperfusion has been shown to be important in managing eyes with retinal vascular diseases, 14 and the extent of nonperfusion has been associated with ME severity and treatment response. 15,16
UWF imaging findings in Coats disease that have been described to date include exudates, telangiectasis, intraretinal hemorrhages, and vascular sheathing. 17 Abnormal vascular channels and peripheral nonperfusion have also been identified with fluorescein angiography in Coats disease. 7,17 However, very few descriptions of peripheral retinal findings in IMT type 1 exist in the published literature. Midperipheral and anterior fundus abnormalities, including lipid exudates and extramacular aneurysms, 3,18 have been observed in a small subset of patients. The current literature is limited in regard to retinal evaluation using UWFA in IMT type 1. To date, only Bohórquez et al have described a patient with microaneurysmal dilations in the midperiphery on UWFA. 19 In the present case, UWFA identified novel peripheral retinal vascular changes including nonperfusion, terminal vascular loops, and arteriovenous anastomosis in the absence of exudation or telangiectasis.
Distinctive peripheral vascular patterns have been reported in healthy individuals, including looping and branching patterns. 2 The loop vascular pattern, wherein the most-peripheral vessels run circumferentially, is also observed in hypoxic conditions such as retinopathy of prematurity and sickle cell retinopathy. 20 However, the reasons why the peripheral angiographic patterns occur remain unknown.
To explain these curious vascular changes, authors have proposed that the peripheral oxygenation status may account for peripheral vascular patterns and microvascular abnormalities. 2 If local hypoxia at the peripheral retina occurs because of immature vasculogenesis at birth, increased VEGF secretion could promote endothelial cell growth, which could contribute to development of the farthest vessel. However, in the far-peripheral retina, the retina is thin enough to derive oxygen supply from choroidal circulation. 21 The sufficient oxygen supply from the choroidal circulation could decrease hypoxic-induced retinal angiogenesis. This may reduce the need for angiogenesis at that area and eventually lead to the loop peripheral angiographic pattern at the edge of far-peripheral retina. 2,20,22 After the loop pattern is developed, the relative hypoxia due to further growth and thickening of peripheral retina or VEGF originating from a neighboring peripheral avascular area may cause subsequent microvascular abnormalities.
Conclusions
Using UWFA, we report a case of IMT type 1 presenting with peripheral vascular findings including marked nonperfusion and vascular loops. Similar vascular changes have been observed in other hypoxic retinal diseases but have not previously been reported in IMT type 1. Identification and further characterization of these vascular abnormalities could be of value for diagnosis, staging, and management of IMT type 1. In particular, peripheral vascular morphology and angiographic findings in IMT may provide further insights into the retinal oxygen supply and peripheral perfusion status, which may be an important direction for future studies.
Footnotes
Ethical Approval
This case report was conducted in accordance with the Declaration of Helsinki. The collection and evaluation of all protected patient health information was performed in a Health Insurance Portability and Accountability Act (HIPAA)–compliant manner.
Statement of Informed Consent
This report does not contain any personal identifying information and therefore written consent was not required.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.