
Abstract
Flu vaccination disparities persist among Black adults in the United States, highlighting the need for culturally tailored vaccination promotion strategies. A cross-sectional survey was administered to 159 members of a faith-based health alliance to examine flu vaccine uptake and related influences. Seventy-four percent reported receiving the flu vaccine. Vaccination was associated with older age, health insurance coverage, proactive health behaviors, and receiving recommendations from doctors and pastors. Flu vaccine uptake was substantially higher than national rates for Black adults, suggesting faith-based outreach and trusted messengers are effective strategies for reducing vaccination disparities.
Keywords
Introduction
Although adult influenza rates have improved in recent years, significant disparities persist among racial and ethnic minority populations in the United States.1,2 During the 2023–2024 flu season, vaccination coverage among Black adults (42%) remained lower than White adults (49%). 1 The cause of this imbalance is multifaceted but has been linked to a lack of trust in health care systems and information sources.3–6 To address these concerns, Healthy Sustainable Communities’ National Minority Quality Forum (NMQF) has successfully collaborated with community faith leaders of inner-city churches to form the Faith Health Alliance (FHA).4,7 The FHA provides church congregants the knowledge, skills, and abilities to maintain a healthy lifestyle, which includes staying current with yearly flu vaccinations. This article presents the findings from a partnership between NMQF and FHA that explored factors influencing influenza vaccination compliance and information trust among a sample of FHA congregates, with the goal of guiding community-based strategies to reduce vaccination disparities among Black adults.
Methods
Survey
A survey was designed in SurveyMonkey™ by a team of NMQF staff and academic researchers to collect information from church congregants related to internal and external influences and motivators for getting a flu vaccine. After multiple iterations of the survey were developed and considered, a final draft was reviewed by content experts for face validity and then finally approved by FHA members for cultural appropriateness. Digital links and QR codes were shared with congregants during services and small-group meetings. Printed paper surveys were also provided to those who preferred or required nondigital participation. In several churches, iPads were provided on-site with the survey preloaded to allow immediate digital responses.
Data collection occurred over a period of 3 weeks, after which the deidentified data were entered into a secured and encrypted database and checked for accuracy and clarity. The survey protocol was reviewed by the WIRB-Coprenicus Group (WCG) Clinical Services Institutional Review Board and deemed exempt 45 CFR § 46.104(d)(2).
Statistical Analysis
Data were entered into IBM SPSS™ version 26 software for analysis. Frequencies and percentages were calculated using descriptive statistics to provide a summary of the demographic data, vaccination status, and survey responses. Cross-tabulations were conducted to explore how responses varied by respondent characteristics (such as age and vaccination status), and Chi-square tests were applied to assess statistical significance.
Results
Demographics and Flu Vaccination Status
Table 1 shows the demographics and vaccination status for the whole sample, with comparisons between vaxed and non-vaxed participants. Most respondents were aged 60 and above, female, and Black/African American. Most were covered by some form of health insurance (e.g., private, Medicaid), either retired or working full-time, and lived in a household with annual incomes between $20,000-$89,999. Approximately three-fourths of respondents were vaccinated for flu (n = 118, 74.2%) during the 2023/2024 flu season. When compared with flu vaccine groups (i.e., vaxed vs. non-vaxed), the non-vaxed group tended to be younger and less likely to have health insurance (both variables statistically significant).
Demographics and Flu Vaccine Status of Sample (N = 159)

Bold value signifies p < 0.01.
Chi-square compares proportion of flu-vaxed vs. non-flu-vaxed for each demographic category.
ns, non-significant.
Health Indicators and Flu Vaccination Status
Roughly 80% of the whole survey sample reported being in either good or excellent health (Table 2). Nearly all (94%) reported they engaged in four or more health-promoting activities such as seeing their doctor regularly (93%), taking medications as prescribed (81%), eating healthy foods, or getting vaccinated regularly (76% each). More than three-fourths of participants were diagnosed with high blood pressure. The most cited source of health information was public service announcements (PSAs). When compared by flu vaccine groups, those who were vaccinated were more likely to participate in healthy behaviors, including taking medications as prescribed, getting recommended vaccines, regular health screenings, and dentist visits.
Health Indicators and Flu Vaccination Status (N = 159)

Bold value signifies p < 0.01.
aRespondents could select more than one response.
Chi-square compares the proportion of flu-vaxed vs. non-flu-vaxed for each category.
ns, non-significant.
Vaccine Motivators, Influences, and Vaccine Status
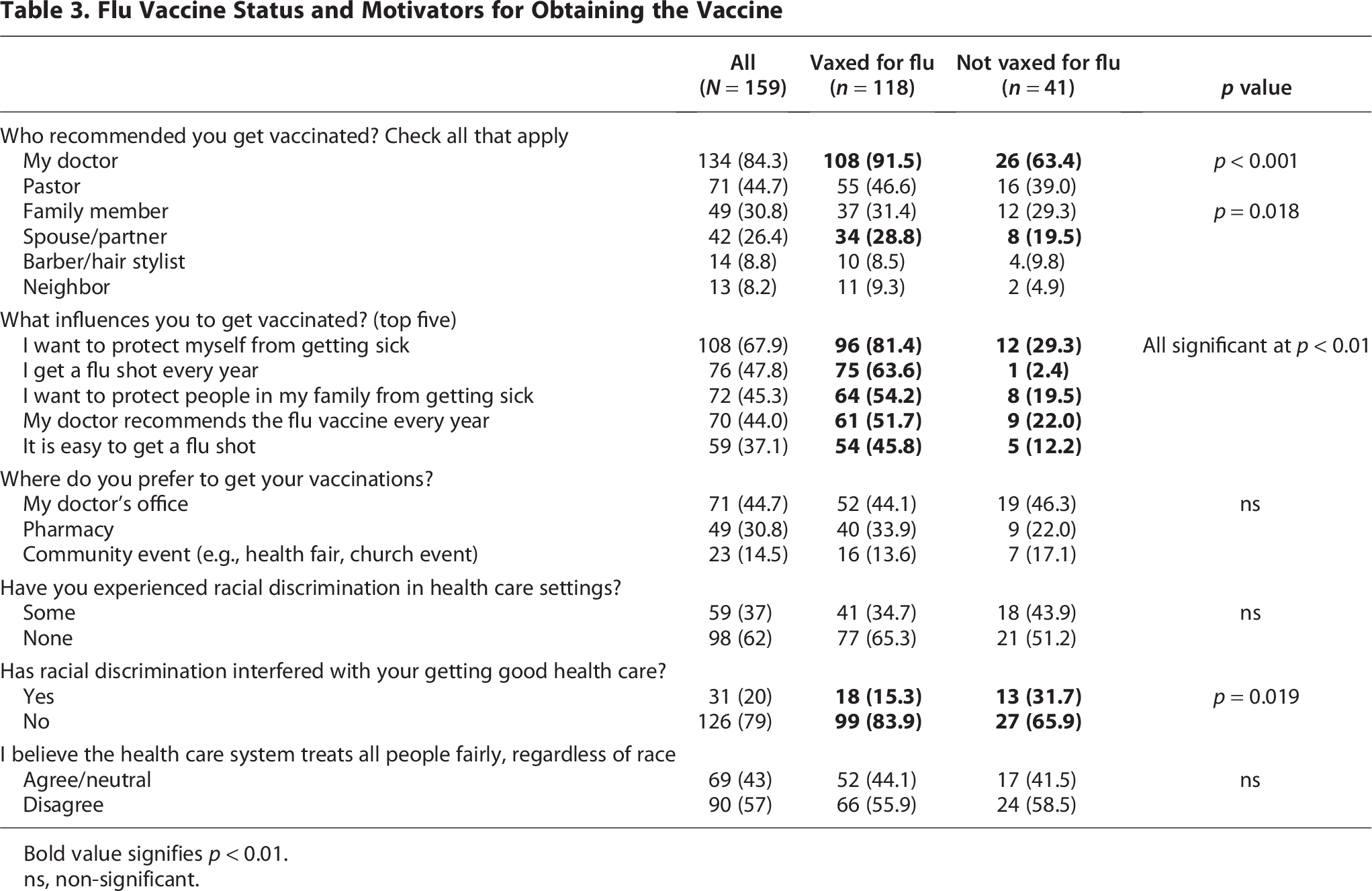
When asked who recommended getting the flu vaccine, a doctor/primary care physician was the most frequently cited, followed by a pastor and family member (Table 3). Most respondents were motivated by personal health reasons, being in the habit/routine of getting vaxed each flu season, and protecting family members. Nearly half said they preferred getting the flu vaccination at a doctor’s office, while others said they preferred obtaining it from a pharmacy or community event. Individuals who were vaccinated for flu were also more likely to be vaccinated for COVID-19 (72.9% vs. 29.3%), shingles (55.1% vs. 26.8%), pneumococcal (50.8% vs. 36.6%) and respiratory syncytial virus (63.1% vs. 40.5%) when compared to those who were not vaccinated for flu (all significant at p < 0.01).
Flu Vaccine Status and Motivators for Obtaining the Vaccine
Bold value signifies p < 0.01.
ns, non-significant.
Discussion
The flu vaccination rate among this sample of primarily older Black adults (74.2%) was notably higher than the national average for Black adults in the United States, which remains below 50% according to recent Centers for Disease Control and Prevention (CDC) data for the 2023–2024 flu season. 1 This elevated rate aligns with prior research demonstrating the success of faith-based outreach in improving vaccination uptake both in the United States and globally.8–10 These findings reinforce the potential of trusted community structures, particularly churches, in promoting preventive health among populations historically experiencing medical mistrust.
In this study, most respondents reported engagement in multiple health-promoting behaviors, including regular doctor visits, taking medications as prescribed, and obtaining recommended vaccinations. These behaviors are consistent with predictors of preventive health service utilization found in prior studies.11,12 The strong health orientation of this group may be partially attributed to their involvement in FHA programming, which appears to foster both individual agency and community norms around wellness.
In this sample, a critical structural factor was health insurance. Only 3% of the sample lacked coverage, and insurance status was significantly associated with vaccination, reflecting national data showing insured individuals are more likely to receive preventive services. 13 Ensuring broad insurance coverage remains essential for equitable access to preventive care.
We also observed vaccination clustering, where influenza-vaccinated individuals were more likely to receive other vaccines (e.g., COVID-19, shingles, pneumococcal, respiratory syncytial virus). While this finding could be reflective of individuals who are simply more health-conscious, it also suggests that health care providers have the opportunity to remind patients of the importance of getting vaccinated for multiple infectious diseases during clinic visits.
It is well known that a physician’s recommendation is a powerful influence among adults to get vaccinated for flu,6,14,15 and our results showed the same was true for this population. However, our participants also cited their pastor as a relevant influence in their decision process. This finding confirms other reports, which conclude that faith-based organizations (FBOs) can play an important role in vaccine uptake and highlights the impact FBOs can have on vaccine uptake among their congregants.9,16
Family members and spouses were also important motivators for getting vaccinated for flu among this sample. This finding is similar to that of Mantina et al., in which a recent focus group study showed that the influence of family was pronounced among African Americans and Hispanics/Latinos when compared to White adults. 17 Other studies have identified marital status or social support as correlates of vaccination uptake,11,12 but few have explicitly highlighted spouses as motivators. Our finding that spouses actively encouraged vaccination echoes broader social influence research, which notes that close ties, including partners, can shape adult vaccine decisions. This emphasizes the power of household-level support in public health campaigns and points to an under-recognized channel for boosting uptake.
Notably, more than half of the study sample reported relying on PSAs, especially those from the CDC or local government, as a primary health information source. Previous studies have shown that PSAs can be an effective way to increase public health guideline compliance in the U.S. adults, if the announcements are customized to individuals’ identities. 18 This reinforces the critical role of widely disseminated, trustworthy, and culturally attuned messaging. Ensuring that such PSAs are accessible and responsive to community concerns is essential for maintaining public confidence and combatting misinformation, particularly in disenfranchised communities.
Limitations
This study has limitations. First, participants were drawn from Faith Health Alliance churches, which may already be more health-conscious or engaged due to previous public health initiatives, limiting generalizability. Second, the cross-sectional design prevents causal inference. Third, self-reported data may be subject to recall or social desirability bias. Finally, while the sample size is appropriate for exploratory analysis, larger and more diverse samples are needed to confirm these results and explore subgroup differences in more detail.
Conclusions
This study highlights the effectiveness of faith-based strategies in increasing flu vaccination rates among older African American adults. Trusted influences such as physicians, pastors, and family members, particularly spouses, played a key role in vaccine decision-making, reinforcing the value of multi-level support systems.
Access to health insurance and engagement in health-promoting behaviors were also strongly associated with vaccine uptake, reflecting the broader importance of structural and individual factors. The observed clustering of multiple adult vaccinations suggests opportunities for health care providers to promote comprehensive preventive care during patient encounters.
Public service announcements from trusted sources like the CDC also proved influential, underscoring the need for culturally tailored and widely disseminated health messaging. These findings support the expansion of faith- and family-centered public health initiatives to reduce vaccine disparities and promote equitable access to preventive services in historically underserved communities.
Authors’ Contributions
All the authors contributed to the study conception and design. Material preparation, data collection, and analysis were performed by H.N., L.P.-D., C.U., and L.L.H. The first draft of the article was written by H.N., and all the authors commented on previous versions of the article. All the authors read and approved the final article.
Footnotes
Acknowledgments
The authors wish to thank the Churches, barbershops, and hair salons that participated in the Faith Health Alliance and HAIR Wellness Warrior initiatives, both for their help in designing and fielding the survey and for all the work they do to reduce health disparities in their communities.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by the CDC, award number