
Abstract
Introduction:
Diversity in the physician workforce is associated with improved patient outcomes, yet individuals from lower socioeconomic status (SES) backgrounds remain underrepresented in medicine. Doctors of Tomorrow (DoT) is a pathway program at the University of Michigan Medical School that provides mentorship and interactive learning experiences to expand health care career access for students from resource-limited backgrounds. DoT recruits students from two Detroit high schools that require entrance exams, raising concerns that the program may disproportionately enroll students from higher SES households with greater social capital. This study aims to evaluate the SES of DoT participants to assess whether the pathway program is reaching students from resource-limited backgrounds and those who are underrepresented in medicine.
Methods:
A cross-sectional, web-based survey was conducted among 122 parents of DoT students to assess socioeconomic markers. Findings were compared with Detroit population data from the American Community Survey and with national medical school applicant and matriculant data from the AAMC.
Results:
The survey response rate was 62%. Only 7% of DoT parents reported working in health care. Compared with Detroit census data, DoT households reported higher parental college education and home ownership, while household income was similar. Racial composition was predominantly Black in both the DoT cohort and Detroit overall. Compared with national medical school applicants and matriculants, DoT parents were less likely to have a college degree and had a distinct racial distribution.
Conclusion:
DoT recruits students without pre-existing access to health care mentors, with household income comparable to Detroit overall, but who significantly differ from national medical school applicants. Ensuring socioeconomic diversity in pathway programs to medical school is essential for diversification of the physician workforce and better outcomes for historically marginalized patients.
Introduction
A diverse physician workforce strengthens the quality, equity, and cultural responsiveness of health care. Physicians from racially, ethnically, and socioeconomically diverse backgrounds bring a breadth of perspectives and community connections that enhance patient communication, trust, and outcomes.1,2 Also, greater representation among physicians promotes innovation, more equitable health policy, and a workforce better equipped to meet the needs of an increasingly diverse US population. By 2045, individuals identifying as racial and ethnic minorities are projected to comprise most of the US population. Yet, Black (5%), Latin (5.8%), and Native American (0.3%) people represent only 11% of the physician workforce.3–5
Persistent disparities in access to medical education contribute to the lack of representation. Inequitable education resources, limited exposure to health care careers, and reduced access to mentorship are some of the barriers encountered by students from historically marginalized and socioeconomically disadvantaged backgrounds. 6 Efforts to diversify medicine, racially and economically, require investment in the development of social capital and opportunities that support student aspirations.
Pathway programs are a promising mechanism for fostering opportunities. By providing early exposure to health care careers and academic preparation, pathway programs cultivate interest, confidence, and a sense of belonging in medicine.7–10 Doctors of Tomorrow (DoT) is a pathway program at the University of Michigan Medical School (UMMS) that was designed to support students from high schools in Detroit who are interested in medicine but have limited access to professional networks or financial resources. Considering the racial disparity in medical training, a key focus of DoT is additionally training future physicians who reflect Detroit’s predominantly Black population. 11 Grounded in Bourdieu’s concept of social capital, defined as the resources and advantages gained through social networks, DoT provides mentorship and experiences that expand the social and cultural capital available to participants.12–14
Currently, the high schools with which DoT partners require entrance exams for admission. These schools were selected due to their primarily Black student body, administrative feasibility, and the schools’ demonstrated capacity to support and sustain external programming to establish a framework for successfully diversifying medical education, which could then be applied to other Detroit schools. 15 The entrance exam was not a selection criterion for our partnership, but there is concern that DoT may disproportionately recruit students from higher socioeconomic status (SES) households because of this entrance barrier. To date, DoT has a limited understanding of its SES-related recruitment efforts. This study aims to evaluate the SES of DoT participants to assess whether the pathway program is reaching students from resource-limited backgrounds and those who are underrepresented in medicine.
Methods
Program Description
DoT is a longitudinal pathway program founded in 2012 as a partnership between UMMS and Cass Technical High School (CTHS) in Detroit, Michigan, USA. 16 In 2020, DoT expanded its reach to a broader student population by partnering with a second Detroit high school, The School at Marygrove (TSM). 17
CTHS and TSM are two of Detroit’s public examination high schools and enroll academically motivated students reflective of the city’s racial and socioeconomic diversity. TSM was chosen as an expansion target for DoT due to its established partnership with the University of Michigan Marsal Family School of Education, which includes a three-year residency program for new teachers. 18 More than 80% of the CTHS student body identifies as members of racial and ethnic minoritized groups (73.37% African American, 14.2% Hispanic), and 62.3% are considered economically disadvantaged. Similarly, at TSM, 98.5% of students identify as African American, and 68.3% are considered economically disadvantaged. 15
DoT provides a structured sequence of programming to foster and sustain early interest and engagement in medicine. DoT Foundations engages 9th- and 10th-grade students through monthly health care experiences, medical student mentorship, professional skills instruction, and hands-on anatomy and simulation activities. Each student also completes a longitudinal capstone research project that focuses on a community health initiative. DoT Rising programming builds on DoT Foundations and occurs from 11th through 12th grade, providing additional resources for navigating undergraduate admissions. Finally, DoT Succeed extends into undergraduate education at the University of Michigan and includes test preparation, mentorship, and medical school application guidance.
Study Population and Design
For the 2024–2025 DoT cohort, 182 applications were received—155 from CTHS and 27 from TSM. The application contains five essay prompts (see Supplementary Data S1) designed to assess applicants’ interest in medicine and community health and their motivations for participating in the program. Applications were reviewed by the DoT leadership team, and participants were selected based on the quality of their responses and curiosity about medicine. 122 high school students were accepted into the program (105 from CTHS and 18 from TSM). All accepted students completed authorization forms, which identified a primary parent, guardian, or caregiver (hereafter, termed “parent”) and their contact information. This information was used to disseminate surveys.
A cross-sectional, web-based survey study was conducted among parents of DoT participants. A self-administered survey was developed following recommendations from the International Association for Health Professions Education Guide no. 87. 19 A literature review was conducted to describe the problem and identify relevant literature and existing surveys. DoT students and leadership collaborated to delineate outcomes of interest. These discussions occurred during a series of regularly scheduled program meetings and feedback sessions, with extensive student input. Survey questions were developed in consultation with an evaluation expert. The final online survey consisted of 22 items covering household demographics, parent education and occupation, employment in the health care field, and living situation. The survey was piloted with DoT alumni and UMMS students. After piloting the survey, revisions were made to ensure alignment with respondent understanding (See Supplementary Data S2).
Data Collection
The survey was administered online using Qualtrics software (Qualtrics, Provo, UT). It was emailed as an open-link survey to each DoT student’s primary parent between April 6 and May 7, 2025. Parents received weekly reminders to complete the survey. To enhance responses, printed surveys were distributed at in-person DoT events. Responses from paper surveys were manually entered and merged with data gathered online. Participation was voluntary with no incentives, and responses were confidential. Responses were collated to characterize the cohort’s SES and connection to the medical field.
Data Curation
From the full survey data, the race, ethnicity, parent employment, job title, parent education, parent health care occupation, household income, car ownership, and home ownership were extracted and deidentified. One duplicate entry was removed after verification with the respondents. Three duplicates were merged based on the responses (from both parents). For employment, the “Looking for work,” “unable to work,” “unemployed,” and “laid off” answers were consolidated to “not employed.” The job titles were categorized into the 11 major occupation groups from the Census Bureau’s Current Population Survey. Generative AI assistance (University of Michigan U-M GPT, based on GPT-4o) was used to support occupation categorization and was reviewed by study investigators for accuracy. Summary tables and figures were generated using RStudio Table 1 and ggplot2 packages, respectively.
Doctors of Tomorrow Parental Demographic Information a

Missing refers to no reported second parent or incomplete data.
Actual response from participant.
Comparison Data Sets
Using the 2023 American Community Survey (ACS), DoT student data were compared with census data from the city of Detroit, which surrounds CTHS and TSM. Data were obtained from Census Reporter, an open-source project that collates and visualizes census data. 11
Applicant and matriculant data from MD-granting institutions were obtained from the American Association of Medical Colleges (AAMC) Faculty and Applicants: Comprehensive Tabulations on Students (FACTS) table. 20 Parental education data were obtained from the 2024 Table A-24, which contains data from the 2018–2025 application years. This dataset reports on EO1/2 and EO3/4/5, which are internal AAMC categories. The EO1/2 categories contained applicant and matriculant parents with less than a Bachelor’s degree or working a service, clerical, skilled, or unskilled occupation. The EO3/4/5 categories contained parents with Bachelor’s, Master’s, or Doctoral degrees with an executive, managerial, or professional occupation. These AAMC categories do not describe education data alone, so we compared DoT parents with less than a Bachelor’s degree with the EO1/2 and DoT parents with a Bachelor’s degree or more with the EO3/4/5 categories. These categories were not used for any direct comparisons.
We obtained the 2019 parental incomes from Nguyen et al.’s article, which obtained the data from the AAMC. Because the DoT household income levels do not perfectly match up with the AAMC data, we categorized DoT levels into the closest categories. The only DoT income level that we could not place into an AAMC category was the 100,000–150,000 category. This was handled by dividing the number of households (7) by 2 and adding half into the 75,000–125,000 (3.5) and half into the 125,000–200,000 (3.5) category. 21
Race and ethnicity data were obtained from the 2024 AAMC FACTS Table A-12, which contained data from the 2021–2025 application years. 22 The data for applicants and matriculants were summed and compared to the DoT racial distribution.
Statistical Testing
Descriptive statistics were used to characterize the DoT cohort. Inferential statistics were used to compare DoT participants with local census data, between partner schools, and with national medical school data. Categorical variables were compared using Fisher’s exact or chi-squared tests as appropriate, and continuous variables were compared using Welch’s t-test. Odds ratios were calculated when applicable. Detailed statistical procedures, including figure-specific analyses and handling of comparison datasets, are provided in Supplementary Data S3. All analyses were conducted using RStudio.
Institutional Review Board Approval
Ethics approval for this study was provided by the University of Michigan Institutional Review Board.
Results
A total of 76 parents (66 from CTHS and 10 from TSM) completed the survey, with a response rate of 62%. Descriptive household demographics for the 2024–2025 DoT cohort are displayed in Table 1. Most DoT students identify as Black or African American (69.7%), and 11.8% identify as Hispanic or Latino or Spanish. Roughly half of all parents work full-time (69.6%). Among the 115 parents who reported employment, 8 work as health care professionals, with 1 physician, 4 nurses, 2 nurse practitioners, and 1 physician’s assistant. 8 parents self-reported working in other health care occupations, including medical assistant, direct care, home health care, social work, dental coordinator, sterilizing technician, claims lead, and oncology administrative assistant.
Socioeconomic Markers of DoT Compared to Detroit
Demographic information of the DoT cohort was compared to that of the city of Detroit, Michigan, using categorical data from the 2023 ACS. The spread of educational attainment between DoT and Detroit households slightly differs; 29.3% of DoT households have completed at least a college-level degree compared to 18.6% of Detroit residents (Fig. 1A, p = 0.011). Using the ACS categories, DoT respondents have a distinct household income, with 65.5% earning over $50,000 compared to 39% of all Detroit households (Fig. 1B, p = 0.00019). To better represent both low- and middle-income families in Michigan, households with incomes of $100,000 or less were combined and compared; this showed no significant difference between DoT and Detroit households (see Supplementary Data S4, p = 0.1915). More DoT parents are homeowners (70.3%) than Detroit families (53.8%) (Fig. 1C, p = 0.009). The racial distribution for DoT is comparable to Detroit with a majority Black population, but the DoT sample reports Pacific Islander and more Asian, and Detroit reports Native American and Other identities (Fig. 1D, p = 3.3e-11).

Comparison between DoT families and the Detroit area (ACS 2023 data for the city of Detroit).
Characterizing DoT Households from CTHS and TSM
Households for students from CTHS and TSM were compared to better characterize the students participating in DoT from each partner school in Detroit. At both CTHS and TSM, most parents work full-time and do not work as health care professionals (Fig. 2A, p = 0.095; Fig. 2B, p = 0.3857). Figure 2C shows there is a wide range of household incomes with no significant difference between schools (p = 0.679). When comparing homes, Figure 2D and E reveals that most CTHS and half of TSM families own their homes (p = 0.223), and the average household size is 4.04 at CTHS and 3.75 at TSM, with no significant difference between schools (p = 0.599). The identified race of participating DoT students is majority Black or African American at both schools (Fig. 2F, p = 0.603).
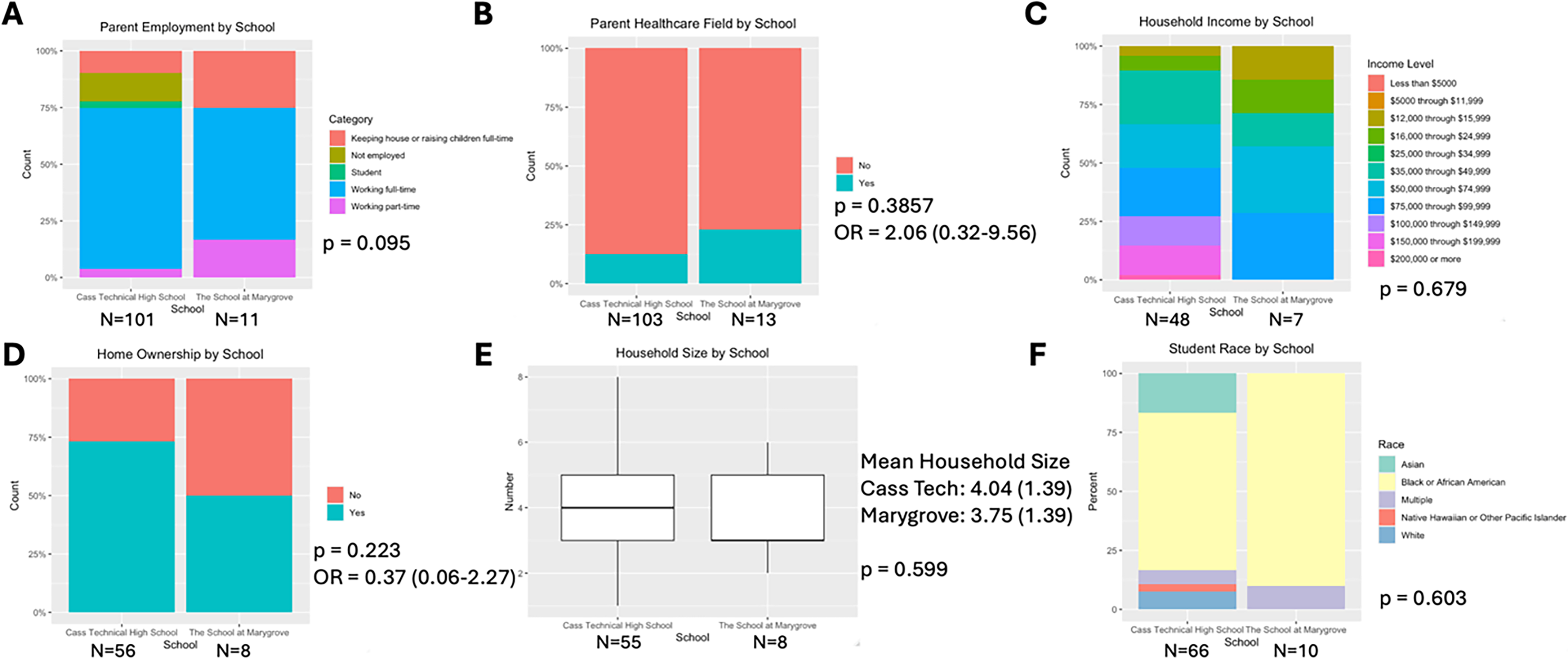
Comparison between DoT families at CTHS (N = 66) and families at TSM (N = 10).
Overall Comparison of DoT Cohort to US Medical Students
The cohort of DoT parents was compared to applicants and matriculants to MD-granting institutions in the United States using AAMC data. This reveals differences in the students participating in DoT and the typical medical school applicant or matriculant. Most DoT households do not have a parent who completed a college education, but most applicants and matriculants to MD schools from 2018 to 2025 did have a parent with at least a bachelor’s degree (Fig. 3A, p < 2.2e-16). We do not see a significant difference in the parental income among DoT students compared to MD applicants and matriculants using accessible data from 2019 (Fig. 3B). Finally, the majority of DoT students identify as Black, which significantly differs from the MD applicants and matriculants who identify primarily as White, followed by Asian (Fig. 3C, p < 2.2e-16). DoT students also significantly differ from applicants and matriculants to DO-granting institutions, following the same pattern as above (see Supplementary Data S5, p < 2.2e-16).
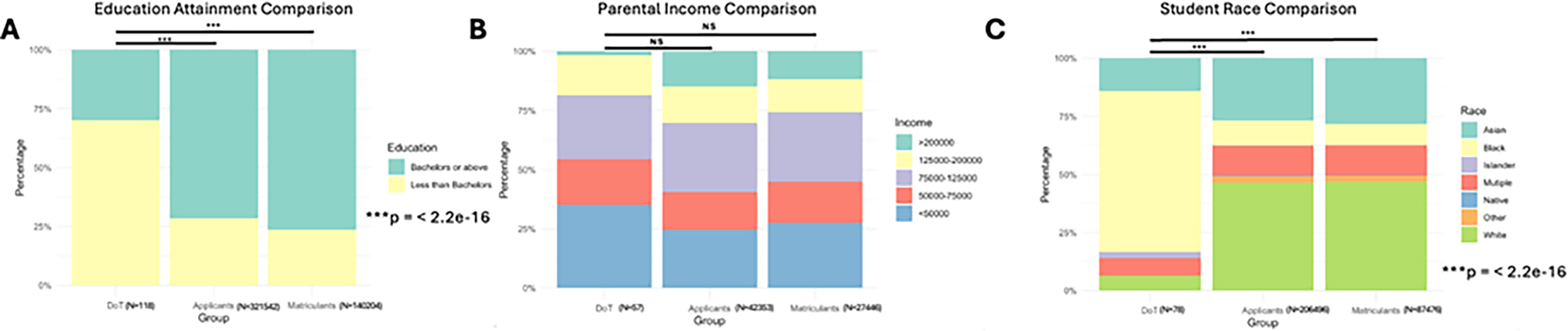
Comparison between DoT families and all applicants and matriculants to MD-granting schools.
Discussion
This study characterizes the households of 9th- through 12th-grade students participating in the DoT program. Through analyses of parent-completed demographic surveys, we examined the socioeconomic composition of our cohort and reflected on the program’s approach to recruiting students who have limited opportunities to explore health care careers. Most DoT households do not have a parent who works in health care. The socioeconomic markers of DoT households differ from the city of Detroit. There were no significant socioeconomic differences between students from CTHS and TSM. Compared to applicants and matriculants to US allopathic medical schools, DoT students came from households with lower parental education levels and greater racial diversity. The majority of DoT students were Black, which differs significantly from the primarily White and Asian applicants and matriculants to US medical schools, demonstrating DoT’s mission of serving a predominantly Black population reflective of Detroit.
Establishing middle or high school pathway programs is an established strategy for building skills and knowledge among underrepresented students with an interest in health science. 23 Since DoT was designed to engage students from underrepresented and/or resource-limited backgrounds, this review of the recruitment process is essential to ensure the program reaches its intended goals and population and furthers our understanding of pathway program demographics as a whole. Previous DoT data (2013–2019) showed that the majority of applicants and accepted DoT students identified as Black women, and were representative of their applicant pools. 24 While DoT reaches racial and ethnic minoritized students, our findings point to the intersecting influence of socioeconomic factors, including parent occupation and education, on access and opportunities. Students with parents in the health care field may benefit from the social capital that facilitates access to mentors and opportunities. 14 Additionally, social capital assists with navigating the higher education admissions process and networking for professional careers. By contrast, most DoT parents do not work in health care, suggesting the program is identifying students without preexisting mentors and networks in the field. Thus, DoT recruitment and opportunities provide important connections and exposure.
Although DoT households reported higher proportion of college education, income >$50,000, and home ownership than the Detroit population, the adjusted comparison of low- and middle-income households (household income <$100,000) showed no statistically significant difference. Having college-educated parents has been shown to influence students’ involvement in advanced high school coursework and achievement in math and reading.25,26 These factors may partially explain why DoT students from families with greater educational attainment attend public examination schools like CTHS and TSM and demonstrate interest in careers in medicine. This highlights a tension in pathway programs between reaching resource-limited students and having sufficient programmatic resources. 27 Students with greater social capital may be better positioned to take advantage of the offering of pathway programs, but additional outreach strategies, like partnering with non-exam schools or seeking additional administrative support, may be necessary to engage students from lower socioeconomic backgrounds.
In 2020, DoT programming expanded to include TSM. Although fewer students from TSM participate in DoT when compared to CTHS, there was proportional representation after adjusting for total school size (8% of TSM students and 6% of CTHS students applied to DoT, with nearly equal acceptance rates).15,28 The lack of a significant socioeconomic difference between CTHS and TSM suggests that DoT was successful in expanding its reach to an additional public examination high school in Detroit. Notably, DoT’s partnership with TSM during the COVID-19 pandemic required virtual implementation, likely contributing to its early engagement. This is similar to a pathway program at the University of Chicago which reported that virtual recruitment and the reduced need for transport during the 2020–2021 program may have strengthened partnerships. 9 Future pathway programs may benefit from the implementation of virtual outreach and programming to foster broader partnerships with schools. Beyond virtual outreach, adapting partnerships between medical schools and high school teacher liaisons would facilitate a foundation for longitudinal growth of new programs. DoT’s existing planning resources and consultations will be made freely available for peer institutions wishing to employ similar partnerships. Programs are encouraged to adapt existing models for their specific settings, including resource availability, mentorship access, and geography.
Limited racial and ethnic diversity among physicians continues to contribute to inequities in patient care. 29 Increasing physician diversity begins with early exposure to health professions, like pathway programs with high schools. A prior study reports that underrepresented students encounter multiple barriers to medical schools, including parent education, financial constraints, and limited mentorship. 30 The DoT cohort’s lower parental college completion rates, lower SES, and underrepresented racial backgrounds in comparison to medical school applicants and matriculants suggest that DoT is reaching students traditionally absent from medical careers. Therefore, partnering with examination schools may not be a limitation of our implementation, but may be a strategy to engage motivated students who are underrepresented in medicine. Longitudinal tracking of DoT alumni will be necessary for ongoing program evaluation and to examine the relationship between participation in the pathway program and matriculation to a health profession.
This study has several limitations. First, we do not possess demographic data on applicants to the 2024–2025 cohort, so we cannot determine that our accepted students are representative of the applicant pool; inferences were drawn from a prior program analysis of applicants. 24 Second, the small sample size from TSM may have limited statistical comparisons between the two schools. Third, there may be bias in self-reported data (i.e., parental socioeconomic data), as well as in nonresponses (i.e., nonrespondents may differ in SES or employment).
Conclusion
Lack of diversity in the health care workforce undermines equitable patient care. While the socioeconomic profile of DoT households appears to be distinct from broader Detroit households, few DoT parents work in health care or have college degrees compared to parents of applicants and matriculants to MD-granting institutions in the United States. Our findings suggest DoT is effectively reaching racially diverse high school students who are underrepresented in medicine and lack parents with connections to the health care field. These findings indicate opportunities for the role of pathway programs with high schools. Ensuring socioeconomic diversity in pathway programs to medical school is essential for diversification of the physician workforce and better outcomes for historically marginalized patients.
Authors’ Contributions
M.S.G.: Conceptualization (equal); methodology (lead); investigation (equal); writing—original draft (lead); visualization (equal). B.L.: Formal analysis (lead); data curation (lead); writing—review and editing (equal); visualization (equal). A.Y.: Conceptualization (equal); methodology (supporting); writing—review and editing (equal); visualization (equal). J.F.F.: Supervision (supporting); writing—review and editing (equal). G.S.: Conceptualization (equal); methodology (supporting); resources, writing—review and editing (equal); supervision (lead).
Footnotes
Acknowledgments
The authors acknowledge Anuoluwapo Abioye, Jaelynn Maldonado, and Isabel Taboada for their contributions to discussing the study topic and its relevancy.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
B.L. is funded by the University of Michigan Medical Scientist Training Program, NIH T32GM156550.