
Abstract
Objectives:
This study examined associations between maternal characteristics, mental health services use, and trajectories of postpartum depressive (PPD) symptoms.
Methods:
Secondary analysis of longitudinal data of mothers <8 months postpartum with PPD symptoms, collected as part of a larger randomized controlled trial. Mothers completed measures of demographic characteristics, parenting, and social support at baseline and monthly reports of Mental Health Services Use and Edinburgh Postnatal Depression Scale (EPDS) scores. Univariate and multivariable mixed-effects linear regression models assessed associations between maternal characteristics, psychosocial variables, and mental health services with changes in EPDS scores.
Results:
Most mothers were Black (72.5%), single (68.1%), and with a high school education or less (50.6%). Average EPDS scores were moderate at baseline, declined over 9 months, but were still high by study end. Univariate analysis showed parenting competence (β = −0.073, 95% confidence interval [95% CI] [−0.14, 0.00]) and perceived social support (β = −0.051, 95% CI [−0.09, 0.00]) were negatively associated with overall EPDS, while parenting stress was positively associated (β = 0.063, 95% CI [0.03, 0.10]). Psychosocial variables were not significantly associated with EPDS in the multivariate model. EPDS scores were higher at baseline among those who reported mental health treatment than those who did not, but score declines were similar in both groups.
Conclusions:
EPDS scores declined but remained elevated over the postpartum period among the cohort. Those who reported mental health treatment had higher but similar declines than those who did not. These findings support policy initiatives to provide 12 months of postpartum coverage for new mothers.
Introduction
Postpartum depressive (PPD) symptoms remain a challenge for new mothers during the postpartum period. PPD symptoms can consist of persistent sadness, anxiety, and a lack of interest in usual activities and affect an estimated 10–20% of mothers globally.1–4 This is significant because high levels of PPD symptoms can have a myriad of negative consequences, including poor infant health, delayed behavioral development, and dysfunctional infant-mother bonding.5–8
An established body of literature has studied the various patterns of PPD symptoms, which demonstrate that the symptoms tend to decrease over the course of a woman’s postpartum period.9,10 PPD symptoms additionally vary by common demographic factors. These common factors, such as low levels of education, low levels of marital satisfaction, and single status, are all found to be associated with greater PPD risk across the postpartum period.11–13
There is growing evidence that various dimensions of a mother’s parenting behavior and psychosocial characteristics have an impact on the severity and progression of PPD symptoms. In particular, some parental characteristics that have been of focus in the context of PPD symptoms include parenting stress, parenting sense of competency, and social support. Elevated parenting stress has been shown to increase the risk of PPD symptoms and may influence the timing of PPD symptom onset in mothers.14,15 Research has also highlighted the protective role of parenting competence, which is a parent’s perception of personal parenting capability and self-efficacy and their perceived social support. A similar study of inner-city mothers confirmed that lower levels of perceived social support and parenting competence are indicated as markers of likely depressive symptoms. 16 These findings vary by ethnicity, with this association reported by other studies to be significant among European American mothers but not among African American or Hispanic mothers. 17 Low or moderate levels of perceived support have been linked to increased likelihood of PPD, while stronger social support may buffer against depressive symptoms.18,19 While parenting stress, parenting competence, and social support have been linked to general depressive symptom burden, a gap exists in how these psychosocial factors impact overall depressive symptom scores over the postpartum period. Furthermore, prior analyses have not considered these psychosocial factors alongside mental health service use during the postpartum period.
The goal of this study was to further assess the association between parenting stress and competence and social support with overall depressive symptoms during the postpartum period and specifically how mental health services impacted PPD symptom trajectory. Understanding the underlying factors and patterns of PPD symptoms can better inform the design of support systems and policy for the postpartum period, especially given the disparities in diagnosis and treatment of PPD within marginalized racial and ethnic groups.20–22
Methods
Sample
Data for this study were collected as part of an ongoing randomized controlled trial of a social media-based parenting program for new mothers with PPD symptoms conducted at six primary care pediatric practices affiliated with a large children’s hospital from November 1, 2022, to April 30, 2025. Mothers with infants aged 1–8 months were screened for postpartum depressive symptoms at routine well-child visits using the Edinburgh Postnatal Depression Scale (EPDS), a validated 10-item screening tool for depressive symptoms. 23 Due to the fact that these routine primary care clinic EPDS screens were only conducted at 1-, 2-, 4-, and 6-month well-child visits, and families may be late for their appointments, 8 months were permitted as part of the enrollment criteria. To be eligible to participate in this study, participants must have been >18 years old, scored between 10 and 20 on the EPDS at their infant’s pediatric visit, be without suicidal ideation/behavior, have access to a smartphone, have an infant <8 months, and speak and read English proficiently. Following informed written consent, mothers were randomized to an online parenting program plus MoodGym, a cognitive behavioral therapy program or MoodGym alone. 24 The study was approved by the institutional review board at the Children’s Hospital of Philadelphia.
Measures
Participants completed demographic data (age, marital status, education level), EPDS, the Parenting Sense of Competency (PSOC) scale, Parenting Stress Index Short Form (PSI-SF), and Multidimensional Scale of Perceived Social Support (MSPSS) at baseline. The PSOC is a validated measure of perceived self-efficacy and satisfaction with parenting. 25 The PSOC evaluates parents’ self-reported parenting competence through 17 items and scores them on a scale ranging from 17 to 102. The PSI-SF is a 36-item screening tool used to evaluate parenting stress and includes the subscales Parental Distress, Parent–Child Dysfunctional Interaction, and Difficult Child. 26 The PSI-SF has a total score ranging from 36 to 180. The MSPSS is a validated instrument used to quantify an individual’s perceived sense of social support with three subscales: Family, Friends, and Significant Other. 27 The MSPSS has a total score range of 12 to 84. Additionally, mothers completed the EPDS and a single item from the National Comorbidity Survey (NCS) each month: “In the past month, did you go to see any of the professionals on the list for problems with your emotions, nerves, or your use of alcohol or drugs?” 28 These two items were scheduled to be completed monthly for 9 months.
Analysis
Simple summary statistics were obtained. The association between changes in EPDS scores and baseline demographic, PSOC, PSI-SF, and MSPSS scores was assessed using t-tests. p-Values < 0.05 were considered statistically significant. Univariate mixed-effects linear regression models were developed to assess the effects of demographic characteristics, parenting stress, parenting competence, social support, and mental health service use on EPDS scores over time. Following univariable models, a multivariable mixed-effects linear regression model was developed to assess the independent effects of these variables on changes in EPDS scores over time. In this analysis, demographic attributes including maternal education, marital status, and maternal age were included, and intervention status was controlled for in the regression model. Time was quantified as months from when baseline scores were recorded. The model included both linear and quadratic time variables to capture potential nonlinear trends in EPDS trajectories. We assessed interaction terms between the time-varying mental health service use and time variables to assess differential change in depressive symptoms over time between those engaged in treatment compared to those not in treatment. Race and ethnicity were omitted from the multivariate analysis since the majority of participants in the main study were African American, and we had no preconceived hypotheses concerning race and ethnicity. We generated predicted adjusted mean EPDS scores from the model for the postpartum period, holding each variable constant. In addition, predicted mean EPDS scores were estimated at planned data collection time points in order to assess differential changes in depression with treatment engagement. All analyses were performed in STATA 18 SE.
Results
Sample Characteristics
In total, 95 mother–infant dyads enrolled in the main study; four mothers were excluded from the current analysis for the following reasons: one was found to be ineligible after study completion and three withdrew. This left 91 mother-child dyads who completed the study. Of these 91 dyads, all 91 (100%) completed the final study visit at 9 months postenrollment.
Table 1 describes the demographic characteristics of the cohort (n = 91). Mothers were predominantly African American (72.5%) with a mean age of 29.9 years (SD = 6.3) and an average of 2.3 children in their household (SD = 1.5). Moreover, the cohort primarily consists of never-married/separated mothers (68.1%). Approximately half of the sample had a high school education or less (50.6%). The mean PSOC score was 67.9 (SD = 10.2), with a range of 45–98. The mean PSI-SF score was 82.2 (SD = 18.1), with a range of 39–139. The mean MSPSS score was 54.4 (SD = 15.9), with a range of 12–84. Of the sample, 36 unique mothers sought mental health treatment at any point in the study, with the average being 4 months of treatment (SD = 3.2).
Baseline Descriptive Characteristics of the Sample

aPWD intervention refers to the Parenting with Depression intervention. This study is a secondary data analysis in which the intervention condition was included as a covariate to adjust for its potential effect on depressive symptoms.
bThis refers to the 36 unique participants who indicated seeking professional mental health support at any point in the study.
Outcomes
In the univariate regression models results (Table 2), all psychosocial variables were statistically significant in their respective models. There were negative associations seen with maternal social variables, like parenting competence (β = −0.073, 95% confidence interval [95% CI] [−0.14, 0.00]) and perceived social support (β = −0.051, 95% CI [−0.09, 0.00]), with overall PPD symptom scores. Parenting stress was positively associated with overall EPDS scores (β = 0.063, 95% CI [0.03, 0.10]). Within the demographic variables model, baseline maternal age was positively associated with EPDS scores (β = 0.16, 95% CI [0.04, 0.28]), as was being Hispanic compared to African American (β = 3.17, 95% CI [0.89, 5.45]).
Univariate Correlates of Overall Depressive Scores

CI, confidence interval.
In the multivariate regression model results (Table 3), greater maternal age was associated with higher EPDS scores (β = 0.12, 95% CI [0.00, 0.23]). Greater maternal education was associated with lower EPDS scores (β = −2.10, 95% CI [−3.92, −0.29]). Similar to univariate models, parenting competence (β = −0.05, 95% CI [−0.15, 0.03]) and perceived social support (β = −0.022, 95% CI [−0.06, 0.02]) had negative associations with overall PPD symptom scores. Parenting stress was also positively associated with overall PPD scores (β = 0.033, 95% CI [−0.02, 0.08]). In addition, Mental Health Services Use was associated with higher EPDS scores (β = 0.94, 95% CI [−0.57, 2.45]).
Adjusted Multivariate Correlates of Overall Depressive Scores, by Baseline Characteristics

aMental Health Services Use was modeled as a time-varying covariate, including interactions with both linear and quadratic time to examine differences in depression trajectories between groups.
Predicted changes in EPDS scores covering a 9-month period were generated using adjusted model-based estimates (Fig. 1). Overall, the predicted model demonstrated a statistically significant decline over time, suggesting a general trend of recovery from PPD symptoms as time progresses. However, throughout the entire period, the cohort was observed to have elevated EPDS scores, with EPDS declining to only roughly 9 on the 30 scale in the later months.

Predicted adjusteda changes in depressive symptoms (EPDS), in months since baseline. aAdjusted refers to the demographic attributes controlled for, including maternal education, marital status, maternal age, and intervention status
Predicted EPDS scores were also analyzed in relation to whether the mother received any therapy or medication, based on the NCS data. Figure 2 stratifies the predicted EPDS scores by the presence of Mental Health Services Use over the course of 13 months, while Table 4 highlights the differentiated predicted EPDS scores at four separate timepoints. Mean predicted EPDS scores were observed to be higher across all months in the mothers who reportedly sought additional treatment than those who didn’t. The interaction terms between NCS assessments and time were not statistically significant, suggesting that there was no statistically significant difference in the rate of decline in EPDS scores between the two groups.
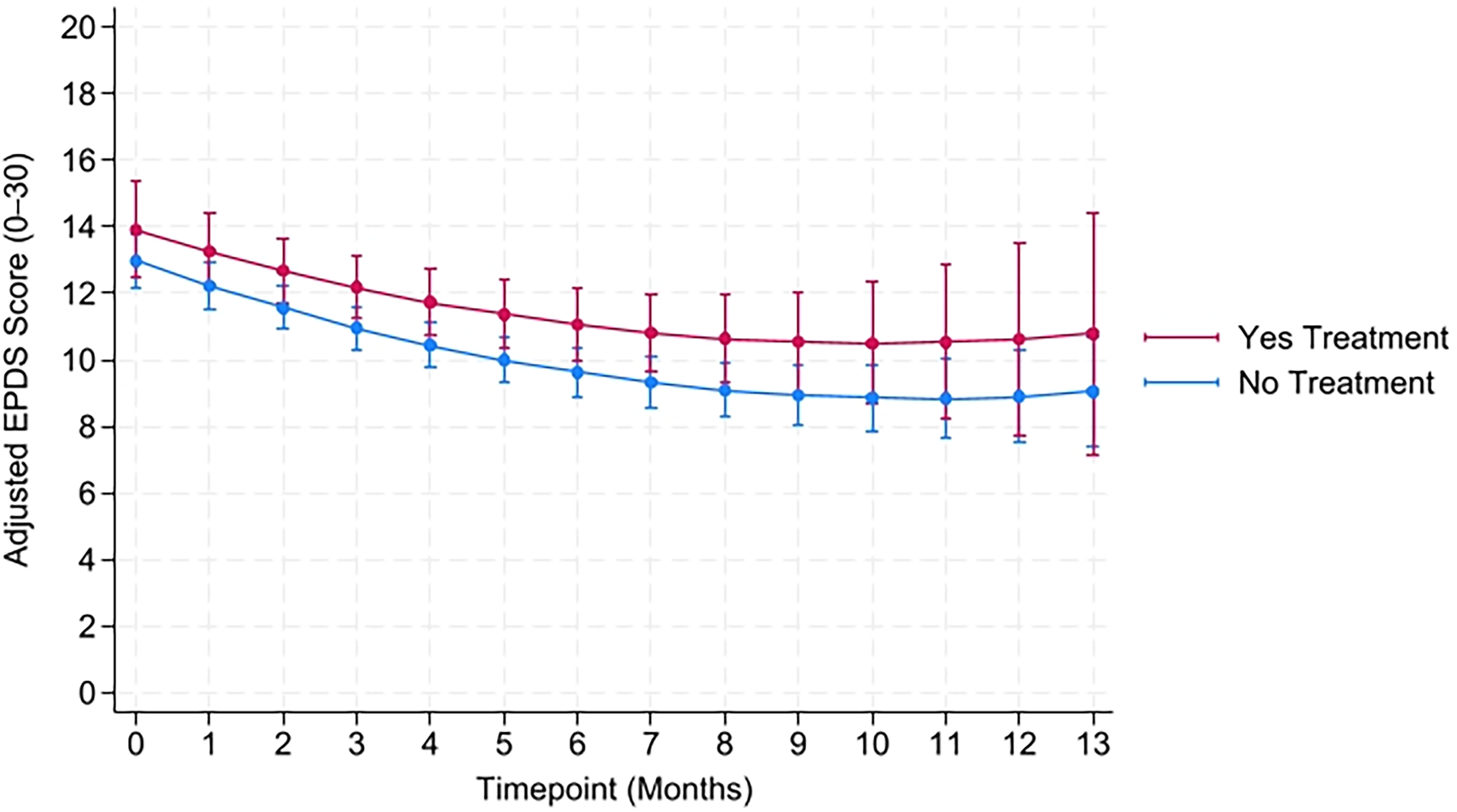
Predicted adjusteda depressive symptom (EPDS) scores by the presence of mental health services treatment, over time. aAdjusted refers to the demographic attributes controlled for, including maternal education, marital status, maternal age, and intervention status
Predicted Adjusted Depressive Symptoms Scores at Selected Timepoints by Presence of Treatment

Discussion
The findings from this study indicated a decline in PPD symptoms over a 9-month period among a sample of urban, predominantly African American women during the postpartum period. A steeper decline in EPDS scores was observed earlier on, while scores began to level off near the 8-month timepoint at approximately 9–10 on the EPDS scale. This temporal trend aligns with prior research suggesting a natural course of decline during the postpartum period.9,10 However, even late into the postpartum period, relatively elevated PPD symptoms were observed, highlighting the issues of persistent depressive symptoms for mothers. Previous studies examining the trajectory of PPD symptoms in the postpartum period have found similar severity occurrences in various populations. A clinical study of Norwegian women revealed that 2.2% of their sample had a “postpartum only” trajectory similar to our study, where their model placed mothers at an estimated mean of roughly 14 on the EPDS scale in the immediate postpartum months before declining. 29 This was similar in a US-based study, where 12.6% of their sample identified with the “moderate-decreasing” trajectory. 30
Higher maternal age at baseline was associated with increased EPDS scores. This finding is consistent with the literature indicating that maternal age is positively associated with PPD symptoms, suggesting that older-aged mothers may have higher stress reactivity, support needs, or health-related vulnerabilities during the postpartum period. 31 Conversely, mothers who had completed college or had postcollege degrees had lower adjusted EPDS scores at baseline compared to those in the reference group. This is also consistent with prior literature and suggests that higher education may confer access to resources that mitigate PPD symptoms.12,13
Although no statistically significant associations were identified for parenting sense of competency, parenting stress, or perceived social support within the adjusted multivariate model, the separate univariate models indicated that each psychosocial variable may still play a role, similar to prior research.13–19 A mother’s emotional state and perceptions can still impact the severity of their depressive symptoms in the postpartum period. It is possible that other unmeasured confounders or specific inter-variable mediating effects may have affected the observable impact in this analysis. Further research is needed to evaluate the effects of these factors on PPD symptom severity and trajectory, and perhaps on the psychosocial variables as well.
Across all timepoints, those who engaged in additional mental health treatment, like medication and therapy, had higher mean EPDS scores. This suggests that those with higher EPDS scores may have been more likely to seek mental health treatment. Findings from prior studies in this population indicate that the majority of mothers with PPD symptoms do not engage in professional mental health care.32–34 However, with nearly 40% of the cohort seeking mental health care at some point in the study, this could indicate higher access to mental health resources through telehealth or perhaps a more favorable perception of seeking help. 35
This secondary analysis uniquely examined the psychosocial variables and their impact on overall PPD symptoms in the postpartum period, and in the context of mental health services use. This longitudinal study also centered on a primarily historically underserved racial population in the United States.20,22
Implications
These findings support the continued development and implementation of policies aimed at enhancing equitable mental health service access for women in the postpartum period. While we observed a general decrease in PPD symptoms in our sample, the persistent depressive symptoms highlight the continued necessity for sustained mental health support and targeted interventions throughout the postpartum period. Our results suggest mothers who may already be disproportionately impacted by unfavorable social conditions (i.e., high stress environments, perceived lack of social network and support systems) may have worsened symptoms in the postpartum period and will need additional support.
The 2021 American Rescue Plan Act permits states to extend postpartum Medicaid coverage to 12 months. 36 As of January 2025, the expansion of 12-month Medicaid coverage for postpartum care was available in 49 U.S. states, which represents a critical opportunity to integrate depression screening, counseling, and care coordination with routine maternal health services during the postpartum period. 37 Our results suggest that limiting postpartum coverage could disproportionately affect mothers with the greatest mental health needs, reinforcing existing disparities that are compounded by existing racial disparities in African American communities.20–22 Those seeking care are not necessarily the ones who may need it the most, as they likely have more severe symptoms, based on our findings. Furthermore, policy and practice frameworks should also prioritize older mothers and those with lower educational attainment, who appear to be at greater risk for more severe PPD symptoms.
Limitations
There are several limitations in the study. First, predicted EPDS scores for infant months 10, 11, 12, and 13 carried a wide 95% CI because of a reduced number of data points at those timepoints. Although data collection was scheduled monthly for 9 months, some participants completed the surveys late, which shifted their time variable ahead and resulted in a small number of observations beyond month 9. Second, the relatively small sample size may have also lowered our ability to evaluate associations between maternal variables, parenting characteristics, and social support with changes in PPD symptoms. Finally, our study findings may not be generalizable to all new mothers with PPD symptoms. Our sample consisted of an urban, predominantly African American population of primarily single women with moderate PPD symptoms and lower educational attainment. We also made the conscious decision to omit race and ethnicity from the multivariate model, given the homogeneity of the cohort and how it may skew results.
Conclusion
We conclude that PPD symptoms declined during the postpartum period but still remained clinically high on average in this sample of new mothers. We found subgroup differences, with older mothers exhibiting more severe depressive symptoms and mothers with greater education exhibiting less severe symptoms. PPD symptoms decreased similarly among mothers who reported receiving mental health services and those who did not. However, mothers who received mental health services had higher depressive symptoms over time. Parenting sense of competency and perceived social support were both negatively associated with overall PPD symptom scores, while parenting stress was found to be positively associated with overall PPD symptom scores. However, the current study was potentially underpowered, and future research is needed to confirm these results. These findings underscore the importance of targeted screening and sustained support services for women based on sociodemographic risk factors. Addressing PPD requires a sustained approach that prioritizes early identification, available access to care, and long-term support during the entire postpartum period.
Authors’ Contributions
A.L.: Conceptualization, software, writing—original draft, writing—review and editing, and visualization. K.H.M.: Methodology, software, validation, and writing—review and editing. M.R.: Conceptualization, data curation, supervision, and writing—review and editing. O.Q.: Conceptualization, data curation, and writing—review and editing. E.M.: Conceptualization, data curation, and supervision. R.C.B.: Methodology, validation, and writing—review and editing. J.P.G.: Conceptualization, methodology, writing—review and editing, project administration, and funding acquisition.
Footnotes
Acknowledgments
The authors are grateful for all the study participants who made this research possible and for the Children’s Hospital of Philadelphia PolicyLab for supporting this work. The authors would also like to thank Joanne Levy from the Leonard Davis Institute of Health Economics for her support of Mr. Lu during his Summer Undergraduate Mentored Research program.
Author Disclosure Statement
The authors declare that they have no competing interests.
Funding Information
This study was funded by a grant from the National Institute of Mental Health R33MH118405 and the Leonard Davis Institute of Health Economics at the University of Pennsylvania.