
Abstract
Introduction:
Maternal morbidity and mortality are urgent public health crises, disproportionately affecting Black and Latina women. In response to the rising rates of preventable maternal deaths and structural barriers faced by Black and Brown birthing people in Central Texas, we came together as perinatal providers and birth workers in Central Texas to form the Maternal Health Equity Collaborative (MHEC) in 2020.
Methods:
In this article, we describe the MHEC, an innovative approach to understanding and expanding reproductive services and support that improve perinatal health. The MHEC includes five birth and parenting organizations (Black Mamas ATX, Healing Hands Community Birthing Project, Mama Sana Vibrant Woman, Partners in Parenting, and Giving Austin Labor Support) and community members to support and uplift Black and Brown birthing communities. The MHEC is grounded in evidence-based, person-centered care services and utilizes the Perinatal Safe Spot and Reproductive Justice frameworks to address social and structural determinants of health. These frameworks emphasize bodily autonomy, dignity, and community-driven care to guide the MHEC’s program design, collaborative structure, and culturally congruent perinatal support.
Discussion:
This article reviews the historical and social context that necessitates collaborative perinatal care, highlights the strengths of establishing a regional collaborative, and details the major achievements and ongoing projects by the MHEC. Through strategic funding, cross-organizational data sharing, and a deep commitment to reproductive justice, the MHEC advances perinatal health equity in Central Texas to offer a transformational model. We provide a scalable model that can empower reproductive justice and birth organizations in the south and nationwide.
Introduction
Maternal morbidity and mortality remain critical public health concerns in the United States. While pregnancy-related deaths are largely preventable, national data underscores persistent racial, ethnic, and socioeconomic inequities, particularly for non-Hisp3anic Black women. The most recent data shows that non-Hispanic Black women had an average maternal mortality rate (MMR) of 50.3 per 100,000 births, which is 2.8 times greater than their white counterparts. 1 Black women also have a 1.9 times higher risk of severe maternal morbidity (SMM) compared with their White counterparts, including sepsis, shock, hysterectomy, and pulmonary edema.2,3 In addition, Black mothers face disproportionately high rates of preterm birth and low birth weight infants as well as higher infant mortality rates when compared with the national average and their non-Hispanic White counterparts.4,5 These disparities are compounded by broader systemic issues including social determinants of health and structural racism. 6
While the MMR for Hispanic women is similar to that of non-Hispanic White women, it doubled between 2018 and 2021, suggesting that COVID-19 was a particular stressor on maternal health.1,7 Hispanic women also have a higher risk of SMM compared with their White counterparts. 2 For example, nationally representative data from 2022 found that Hispanic women had a 22% higher risk for SMM compared with White women. 3 Hispanic women also experience a nexus of other structural barriers related to punitive immigration policies, limited health insurance options, and a lack of linguistically appropriate care.8,9 However, there is still a general lack of culturally congruent and accessible community-based reproductive health care. 10
Texas context
Texas ranks as one of the lowest performing states in maternal health based on outcomes like maternal mortality, morbidity, infant mortality, and preterm birth.3,11 The Texas Maternal Morbidity and Mortality Review Committee (MMMRC) was established in 2013 to understand and address high rates of preventable pregnancy-related deaths and SMM and has released several reports. The 2020 MMMRC report includes data from 2013 to 2018 and indicates a major racial disparity in SMM, with Black women experiencing 299.4 hospitalizations per 100,000 births compared with 150 hospitalizations per 100,000 non-Hispanic White births. 12 Moreover, the 2024 report highlighted that non-Hispanic Black women in Texas had a MMR 2.3 times greater than their White counterparts in 2020 (39.0 deaths per 100,000 compared with 16.1 deaths per 100,000, respectively). 13 While the rate of SMM decreased by 2021, non-Hispanic Black women still faced an increased risk of 134.4 cases per 10,000 hospitalizations, nearly double the rate of White women. 14 Maternal health disparities also exist for Latina women in Texas. The MMMRC report found Hispanic women had an increased MMR in 2020 (22.2 per 100,000 births) compared with White women, as well as a 30% higher risk for SMM hospitalization. 14
Texas also has one of the highest rates of uninsured individuals in the country, a considerable barrier for accessing necessary prenatal and postpartum care.15–17 46.5% of counties in Texas are defined as medically underserved or maternity care deserts as compared with the national average of 32.6%. In rural areas across Texas, this disparity is exacerbated as 28.4% of women live over 30 min away from a birthing hospital compared with 3.8% of women living in urban areas. 18 Recent policy shifts also influence perinatal health outcomes. While the full impact of abortion restrictions following the reversal of Roe v. Wade is not fully observable in maternal health statistics, early reports suggest worsening access to obstetric care, which would likely exacerbate the existing burden of maternity care deserts. 19
The MMMRC’s 2024 report recommended strengthening TexasAIM quality improvement initiatives, expanding on public awareness campaigns such as “Hear Her Texas,” increasing provider education on urgent warning signs, and improving access to preconception and perinatal care for high-risk individuals. 13 These findings and recommendations reinforce the need for community-based, culturally aligned models of care like the Maternal Health Equity Collaborative (MHEC) in Central Texas. Maternal mortality and morbidity contributing factors are complex and occur over the life course. Preconception health awareness and early entry into prenatal care can reduce maternal mortality and morbidity risk factors like chronic disease. While the MMMRC provides critical statewide data and recommendations, its scope is broad and policy-focused. Community-based collaboratives like the MHEC can complement this work by addressing gaps at the local level and building culturally congruent, person-centered care networks.
Structural determinants of maternal health
The social and structural determinants of maternal health are key drivers of racial and ethnic disparities. 6 Lack of health insurance or transportation as well as housing and financial insecurity are some of the primary barriers to accessing timely and high-quality maternal health care that make parts of Central Texas materno-toxic environments for many Black and Hispanic birthing people. In addition, social risk factors such as stress, interpersonal violence, food insecurity, and lack of social support are associated with maternal morbidity and mortality.20–22 These social factors disproportionately impact Black and Latina women, largely due to a fractured health care system, racism, and poverty, and are associated with late or no prenatal care, lower rates of postpartum visit follow-up, and perinatal mental health.23–25 Therefore, these determinants form the underlying rationale for the necessity of the MHEC. Equity-centered perinatal interventions need to go beyond individual-level solutions by infusing health equity concepts such as intersectionality, reproductive justice, cultural competence, and dignity, within the community-based support available to birthing individuals and infants. 26
Theoretical frameworks
To fully address the structural determinants of maternal health within Central Texas, the formation of the MHEC was guided by two primary frameworks: the Perinatal Safe Spot (PSS) model and Reproductive Justice. These frameworks offer philosophical and practical foundations for building community-led collaboratives like the MHEC. Furthermore, these frameworks were intentionally selected because they directly address the gaps identified in Texas’s maternal health landscape by addressing the need for culturally congruent, community-based care. The following section describes how these frameworks shape the design, delivery, and evaluation of the MHEC programs.
Perinatal safe spot
The National Perinatal Task Force (NPTF) developed the PSS, which is defined as “physical or virtual spaces where women and families can safely connect and find support.” PSS was conceptualized to reduce the number of “materno-toxic areas,” a term coined by the NPTF to describe areas where it is unsafe to be pregnant, parenting, or breastfeeding, particularly for Black, Latina, and other women of color. This toxicity refers to implicit and explicit biases, classism, sexism, racism, or other discriminatory factors. 27 Previous research has found patient-defined “safety” is rooted in three components: acknowledgment that the dominant culture has an impact, that care is provided in the community, and that providers respect patient choices and cultural knowledge. 28
The development of PSS is also rooted in the JJ Way Model of Maternity Care, a comprehensive model of maternal care created by midwife Jennie Joseph and her team. As per the “JJ Way”: access, connections, knowledge, and empowerment are principles vital to the success of a PSS. The goals of this model of care include a reduction in preterm births and low birth weights, increased bonding between parents, their families, and their newborns, and better rates of human milk feeding. 27
PSS are coming together to form Perinatal Safe Zones (PSZs) in Central Texas. A PSZ is defined as an area in which community-based organizations come together and share a vision and commitment to pool resources and services to create a “Safe Zone” where birthing people of color can safely and securely receive community support and resources with respect and dignity. The work of the NPTF inspired the involvement of St. David’s Foundation in bridging maternal health gaps throughout Central Texas.
The PSS framework directly informed the design and evolution of the MHEC. Each member organization operates as a PSS, creating culturally affirming spaces where birthing people can receive support without discrimination or fear. The rationale for forming a collaborative came from the understanding that individual Safe Spots are strengthened when coordinated.
Reproductive justice framework
Rooted in the work of SisterSong and empowerment of birthing people, this framework emphasizes the right to bodily autonomy, the right to have or not have children, and the right to parent children in safe and sustainable communities. This framework is rooted in equity and justice for birthing people and marginalized communities and emphasizes analyzing power systems, addressing intersecting oppressions, centering the most marginalized communities, and joining together across issues and identities. 29
Together, these frameworks shaped the creation of the MHEC. The limitations in Texas’s maternal health infrastructure, coupled with the community’s need for culturally aligned and community-controlled care options, led five organizations to formalize a collaboration grounded in these principles.
The maternal health equity collaborative
Background
The mission of the MHEC is to make birth safer for Black and Brown families by building community and using collective power to create lasting change rooted in birth justice and equity. The vision of the collaborative is for these communities to enter a space where birth is a safe, healthy, and joyful experience. 30 This mission is achieved through shared infrastructure, culturally congruent services, and cross-organizational collaboration.
The MHEC was developed out of necessity during the pandemic and began with a local advocacy effort to ensure birth worker support remained in hospitals during lockdown COVID-19 procedures. In 2020, hospitals changed their protocols to limit birthing persons to one support person. This forced birthing persons to choose between having a partner or birth worker present. However, we advocated for birthing people to maintain access to a birth worker, arguing that an individual should not have to choose. Therefore, five maternal health organizations across Central Texas came together to advocate for a new hospital policy that centered the needs of birthing people. After solidifying doulas as members of necessary health care teams, the MHEC wrote an internal needs assessment to understand gaps in the region. These initiatives set the stage for formally establishing a collaborative.
Structure
Our collaborative centers Black women and women of color from leadership to providers. We are comprised of five organizations that provide direct services and support services to underserved communities including doula care, lactation support, mental health support, childbirth education, and postpartum support: Black Mamas ATX (BMATX), Giving Austin Labor Support (GALS), Healing Hands Community Birthing Project (HHCBP), Mama Sana Vibrant Woman (MSVW), and Partners in Parenting (PIP). We then came together to establish a board, steering committee, and 10 working groups or circles. Refer to Figures 1 and 2 for more details.
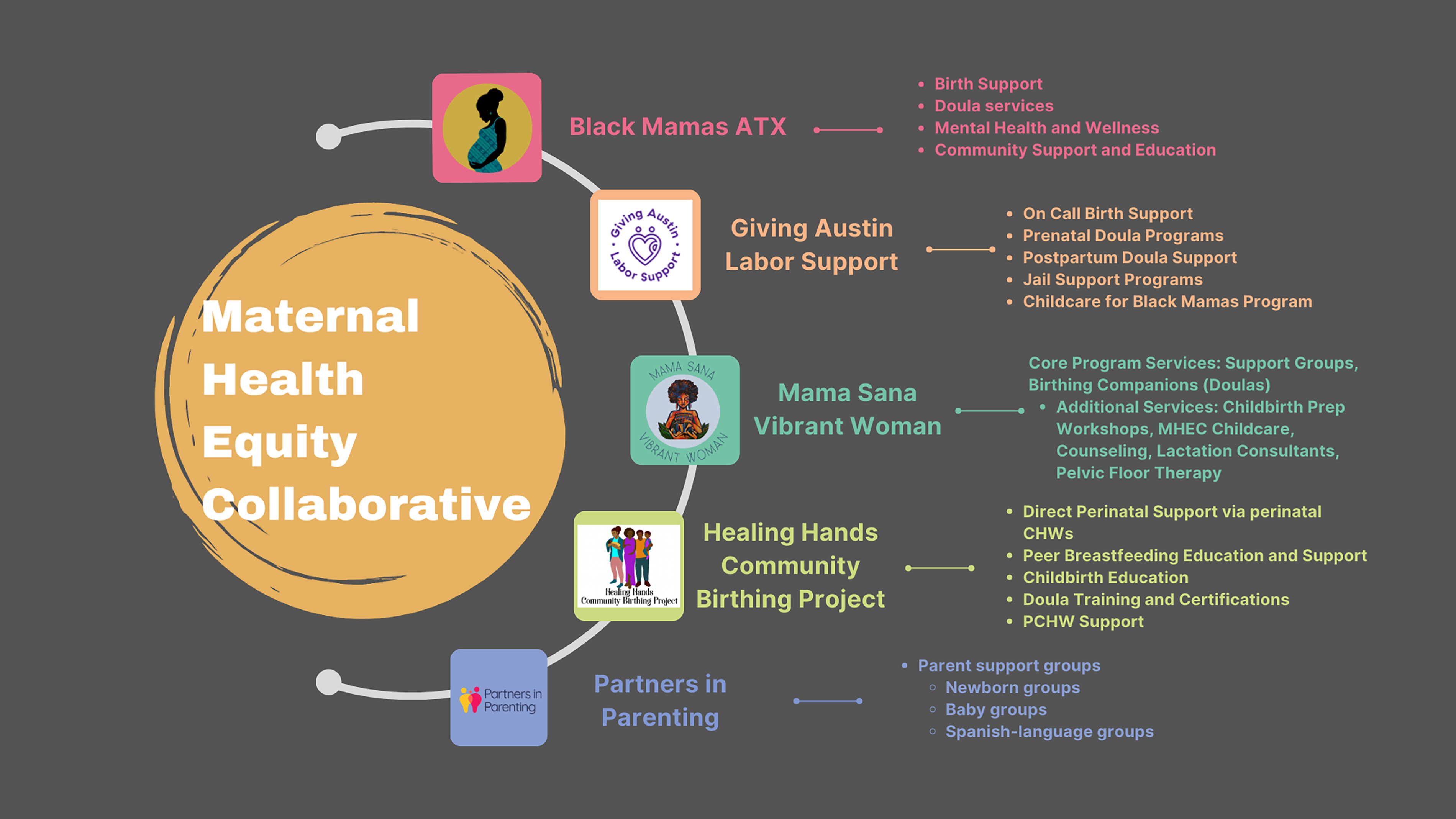
MHEC organizations. MHEC, Maternal Health Equity Collaborative.

MHEC organizational structure and leadership committees.
Equitable perinatal health care delivery
Over 90% of pregnancy-related deaths are preventable. 31 When women receive care aligned with their cultural values, personal preferences, and dignity, they are more likely to engage with health systems, clinician recommendations, and experience improved birth outcomes. Our work at the MHEC is grounded in respectful and patient-centered care. We intentionally train and hire Black and Latina women from the community, often previous clients, to provide services by and for the community.
As birth workers in Central Texas, we have dedicated our lives to addressing systemic barriers and improving health outcomes for Black and Brown women and families. A large portion of Central Texas, including Caldwell and Bastrop County, is considered maternity care deserts. 32 We see this in our day-to-day work, where rural individuals and families are isolated and struggle to access necessary reproductive care.
Considering the limited access for Black and Latina women seeking community-based perinatal services, the MHEC was established with the goal of making birth a safer practice for Black and Brown families across Austin and Central Texas. Through our innovative model of care, we incorporate key components of respectful maternity care including efficient and effective care and continuity of care. Not only does each of our organizations foster collaboration among perinatal care providers, but we also engage in collaboration across organizations. Each participating organization focuses on different social supports such as food access, housing, or mental health, and we share these resources and programs with other MHEC organizations via referrals and coordinated care. This model of care emphasizes shared responsibility, open communication, patient autonomy, and respect across birth workers and organizations.
Black Mamas ATX
BMATX has been serving Black mothers in Central Texas since 2018. The organization’s goal is to reduce and ultimately eliminate the alarmingly high rates of maternal mortality and morbidity among Black women.
Healing Hands Community Birthing Project
HHCBP is a nonprofit organization formally established in 2018 with the mission to eliminate birth outcome disparities that exist between Black and Brown mothers to lower maternal mortality in the Greater Austin and Houston areas. HHCBP provides pregnancy education, birthing doula support, and postpartum doula services. HHCBP prioritizes training and employment of equitable and diverse maternal health workforces to provide culturally congruent care to their clients.
Mama Sana Vibrant Woman
MSVW was formed in 2012 to improve pregnancy and birth outcomes for communities of color in Central Texas specifically through education and support. MSVW focuses on training caregivers of color to provide culturally sensitive and congruent care using the midwifery model.
This organization provides free wraparound care.
Partners in Parenting
PIP was founded in 2014 by two young mothers with the goal of bridging maternal health gaps in the city of Austin. PIP brings new parents together through facilitated support groups to create a space for community and connection. They also offer groups based on shared identities to ensure that every family has the support they need during early parenthood.
Giving Austin Labor Support
GALS started as a grassroots organization in 2008 with the goal of providing wraparound perinatal support to underresourced, unsupported, and incarcerated families in Central Texas.
MHEC achievements and projects
At the end of 2020, we published a report with support from St. David’s Foundation to shine a light on the gaps and inequities in maternal care throughout Central Texas. In addition, we published a report in April 2021 entitled The Spirit of Possibility. The report details the inequities in maternal health and provides evidence-based recommendations to the St. David’s Foundation for future funding endeavors. We recommended the extension of Medicaid coverage for postpartum individuals to 12 months, doula funding and reimbursement, antiracism training across health care ecosystems, safe spaces for Black, Indigenous, and other women of color, and the implementation of community-informed funding models. 33 These reports were disseminated to St. David’s Foundation program officers, local policymakers, and health system leaders.
In 2021, St. David’s Foundation created a PSZ funding opportunity. They awarded $1.8 million to 12 programs including BMATX, HHCBP, and MSVW to reduce maternal mortality, improve mental health, facilitate insurance coverage, advance access to family planning and reproductive care, and initiate breastfeeding programs. This funding was designed to transform the region into a PSZ. In addition, we received local foundation funding such as the Safer Childbirth Cities grant from Merck for Mothers. This initiative supports community-based organizations in cities with a high burden of maternal mortality and morbidity. With these funds, the MHEC advances culturally sensitive and comprehensive perinatal childcare services to complement doula support and ensure that Black mothers and families can access holistic, whole-person care.
In addition to receiving local funding through foundations, we also engage in local- and state-level advocacy by organizing advocacy days at city council or the state legislature regarding legislation on childcare funding, Medicaid benefits through 12 months postpartum and doula reimbursement through Medicaid. While we are engaging in this work as individuals and not organizations, this is a great way to build trust among staff, clients, and community members and act as a community.
Financial stability of the MHEC
MHEC provides financial stability to all birth worker organizations within the collaborative by streamlining administrative tasks and sharing federal and state funding when applicable. Individual organizations receive funding from various sources including local foundations, corporate or private foundations, city, state, and federal grants. These grants may fund operations overall or various programs (e.g., a childcare program or a mental health program). MHEC organizations often collaborate on larger state or federal grants and allocate a small portion of these grants to go directly toward the MHEC. For example, the Health Resources and Services Administration’s (HRSA) Healthy Start grant set aside funds to cover the cost of the data management system, Well Family System (WFS). MHEC may also write grants for the entire collaborative, to fund activities or efforts that benefit all member organizations. In the 5 years since the establishment of MHEC, we have cemented ourselves in the birthing community. We have applied for 15 grants between 2024 and 2025, receiving three and securing $1,746,800 since inception.
Limitations in reimbursement for doulas and midwives at the state and national level put financial pressure on nonprofits, and financial sharing within MHEC provides more sustainability. In 2025, we received 501(c)(3) status to further develop and support collaborative infrastructure. While there are no requirements or rules for MHEC organizations to include a percentage or portion of grant budget toward the collaborative, member organizations have organically written the MHEC into grant proposals. At the MHEC, we are considering it an expectation as part of our strategic planning for member organizations to write us into future grant proposals, but it has not been officially operationalized yet. While there is currently one full-time administrator, future planning includes more staffing so we can continue to grow and support the community.
Healthy Start funding for Healthy Start Central Texas (HSCT) has enabled participatory organizations such as BMATX and HHCBP to engage in mixed-method evaluations of individual data, which has benefitted the data infrastructure and sharing of the entire collaborative. Furthermore, every Healthy Start program has a Community Consortium, which has built on the collaborative nature of the MHEC. This consortium has brought people together to reach a shared goal: creating an environment that supports maternal, infant, and family health and well-being.
Data infrastructure and sharing
Data infrastructure costs are often high and can be restrictive, particularly for small, nonprofit organizations. Sharing federal and state funds that invest in streamlined data collection and sharing processes can maximize funds. Healthy Start funding has facilitated data sharing across MHEC organizations through a data management system called WFS. WFS is a comprehensive client data intake forum, which has enabled participatory organizations in the MHEC to generate benchmark data for the HRSA and keep track of relevant data and client outcomes. This information can be used to communicate with participatory organizations and arrange necessary referrals for clients, ultimately improving health outcomes through collaborative modes of care. The lead organizations on the Healthy Start grant, BMATX and HHCBP, have both fully transitioned to WFS and are documenting all of their organizational data here, for both HS participants and clients who are not enrolled in HS. The additional three organizations have been trained to document HS data in WFS, but they are currently documenting data in outside systems as well.
Barriers and lessons learned
Since its inception, the MHEC has faced several challenges including limited reimbursement for perinatal community health workers and doulas, variability in organizational capacity, delays associated with adopting new data systems, and threats to funding. Through these struggles, the MHEC has adopted consistent communication between and within organizations, prioritized community hiring, and attempted to diversify funding streams to strengthen sustainability. We have also maintained strong working relationships with the City of Austin and local foundations to maintain financial sustainability across member organizations.
Ongoing collaborations
One strength of MHEC’s approach is the pooling of grant funds and/or social services across MHEC organizations. We have highlighted below several ongoing collaborations that have been successful in expanding access to social services across MHEC organizations and clients. Refer to Figure 3 for more details.

MHEC services.
Black solidarity model and HSCT
In April of 2024, BMATX was awarded $1,008,033 from HRSA to develop a continuum of perinatal services called the Black Solidarity Perinatal Model and serve approximately 700 participants annually. These services meet the requirements of the Healthy Start initiative as they promote health and education, preventative screening, referrals and linkage to community services, navigation support across the clinical care continuum, and robust networks of referral partnerships. HSCT collaboratively provides direct services through several MHEC organizations, including BMATX, HHCBP, and PIP, to make these goals a reality.
Our goal is for HSCT to improve Black maternal and infant outcomes in Central Texas based on the prespecified Healthy Start benchmarks: access to prenatal and postpartum health care, breastfeeding initiation and continuation, depression screening and mental health service referrals, health behaviors during the perinatal period, infant care, and infant health care access. As previously mentioned, HSCT has enabled the MHEC to engage in data infrastructure and sharing, development of a Community Consortium, and supported mixed-method analyses to advance client health outcomes. We hope that this grant will enable MHEC organizations to monitor and align on primary maternal and infant health outcomes for streamlined tracking of community outcomes and to support future grant writing.
Culturally congruent mental health services
Culturally congruent models of care typically refer to diverse providers, culturally relevant mental health treatments, offering care in the client’s preferred language, and recognizing structural and historical trauma. Each organization provides direct mental health services or referrals to culturally sensitive providers. BMATX also sponsors confidential psychotherapy and counseling with Black providers for all their clients and for Black clients of other MHEC organizations under HSCT.
Childcare program
The MHEC childcare program began at the collaborative’s inception in 2021 to reduce the number of children who were put under supervision or care of Child Protective Services during perinatal emergencies due to the lack of adults present to provide care. This program was supported by the St. David’s Foundation, and the MHEC successfully developed a community-oriented approach to “free, short-term, culturally congruent, high-quality in-home childcare for birthing communities in Central Texas during the perinatal period.” 34 Each MHEC organization has access to these direct services, with some organizations supervising specific initiatives. GALS provides on-call childcare specialists to MHEC clients. While each individual organization facilitates appointment-based care and postpartum respite, childcare, and support. 34
Food access program
Tackling barriers to food access improves public health and health outcomes, supports economic stability, strengthens communities, and promotes equity. 35 Increased access to healthy food also lowers the rate of chronic disease prevalence including diabetes, obesity, and cardiovascular complications. MHEC collaboration with WIC empowers birthing and pregnant clients to access the services available such as free lactation consultations from peer and board-certified lactation consultants. 36
Free community baby showers
For the past 5 years, GALS and PIP have collaborated to organize biannual Community Baby Showers for their clients and other pregnant individuals in the Central Texas area. In addition to providing parents with essential supplies, community baby showers increase awareness of the MHEC and the wide range of services its partner organizations offer, fostering stronger connections between families and the resources available to support them throughout the perinatal period.
Conclusion
The MHEC was formed to address the social, economic, and racial inequities in Central Texas that are impacting clients within each MHEC organization and across the broader community. The work of the MHEC can be best understood through the interconnected components highlighted throughout this descriptive article: the unification of five community-based organizations, shared infrastructure and funding, coordinated care, and the application of evidence-based frameworks to deliver culturally congruent perinatal services. Taken together, these pillars demonstrate how the MHEC functions as a cohesive, community-rooted maternal health system.
This innovative model of care demonstrates how building a collaborative can expand access to respectful maternal health care and enhance community impact by aligning services and reducing social and health burdens faced by Black and Brown populations throughout Central Texas. The MHEC offers a scalable strategy rooted in collaboration and community enterprise to improve maternal health outcomes and advance equity beyond its current geographical scope.
Authors’ Contributions
K.B.: Conceptualization, writing—original draft, supervision, resources, and project administration. D.T.: Writing—reviewing and editing, resources, and project administration. J.R.: Writing—reviewing and editing and project administration. C.V.: Writing—reviewing and editing and project administration. R.M.: Writing—reviewing and editing and project administration. M.M.: Writing—reviewing and editing and project administration. R.K.: Investigation, writing—original draft, and visualization. L.P.: Conceptualization, visualization, writing—original draft, and supervision. All authors reviewed and approved the final article.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.