
Abstract
Background:
The proportion of the U.S. population identifying with multiple races and ethnicities has increased in the last decade, but we have limited knowledge of how these individuals self-identity.
Methods:
We conducted a secondary analysis of data on how participants reported their racial/ethnic identities in Giving Voices to Mothers (GVtM), a community-based participatory research study (2016–2017) capturing the perspectives of childbearing people from communities of color and those who planned births at home or birth centers in the United States. Survey items were codeveloped by service users and community health workers. We used descriptive and bivariate statistics to explore how respondents reported racial/ethnic identity, how multiracial identity was related to personal characteristics, and how people used the “other” category.
Results:
Of 2700 survey participants, 2522 (93%) responded to the race/ethnicity questions. Respondents who expressed multiracial identity (n = 339) most often marked more than one racial/ethnic category (78%) or marked the category “biracial” (22%). Multiracial respondents were more likely to be 29 years or younger, to live in the Southern or Western regions of the United States, and to be of low socioeconomic status. In contrast, individuals identifying with the specific term “biracial” were more likely to live in the Midwest or Northeast and to have a higher socioeconomic status.
Conclusion:
The GVtM model for sociodemographic data collection demonstrates how community members can inform the design of racial/ethnic categories that better reflect their lived experience and preferences for self-identification. This can, in turn, enhance participation in and value of findings on health inequities.
Introduction
The U.S. population has experienced a dramatic increase in racial/ethnic diversity, including an increase of 276% in people with multiethnoracial identities between the 2010 and 2020 census. 1 A Federal Interagency Technical Working Group on Race and Ethnicity Standards revising federal standards for reporting race and ethnicity, Statistical Policy Directive No. 15 (SPD-15) identified the increase in multiracial/ethnic identity as one of the drivers for a need to revise standard categories and analytic approaches in order to better capture and understand the experience of people identifying as multiethnoracial.2,3 Yet we have limited knowledge of how people identifying as multi-ethnoracial conceptualize their own identity, and what terms they identify with.
Well-designed measures of race and ethnicity have the potential to elucidate health and health care inequities.4,5
Researchers have begun to seek different ways of categorization that are better aligned with self-identification and provide greater nuance to understanding the experience of Black, Indigenous, Latin, and other racialized individuals. We follow in the footsteps of scholars such as Saperstein, Gómes, and Martinez in ascribing to the concept of race and ethnicity as social constructs that are dynamic both over time and social context.6–8 We also ground this work in social research, feminist action research, and research justice frameworks,9–12 in particular, the belief that decolonizing research requires involving sharing power with marginalized communities and involving them in every stage of the research process, including the construction of ethnoracial categories.
If multiracial identity, broadly, and the label of “biracial,” more specifically, follow the patterns of self-identity for the term “Latino/a/e,” 14 they might most readily be assumed by respondents from demographics aligned as progressive, i.e., individuals with greater education and higher income, privately insured, and younger. Multiracial identity might be anticipated in regions of the country with larger proportions of first-generation immigrants (the South and the West). Given different ethnoracial paradigms across countries, multiracial identity might be more readily adopted among individuals born in the United States than those born in other countries.
To date, no one has examined these assumptions from the lived experience perspective. In addition, this study was conducted in the United States, a country where Black, Latin, and Asian populations represent a very complex set of multiracial and diverse ethnic identities and collectively constitute nearly 40% of the national population. 15 Thus, we aimed to examine how people from both unique and overlapping underrepresented groups self-identify. The Giving Voice to Mothers (GVtM) study was a community-based participatory research study that examined perinatal experiences among 2700 women in the United States. In this secondary analysis, we detail an innovative and community-responsive methodology for designing an instrument that supports self-identification of sociodemographic data on race and ethnicity and explores the characteristics of individuals expressing multiracial or biracial identity.
While the Giving Voice to Mothers study used gendered language that is mirrored in this analysis, we acknowledge that pregnancy and birth are not limited to those who self-identify as “women,” “mothers,” or “female.”
We also recognize the limitations of and lack of clarity around terms like Latina and Hispanic. We have sought to define our use of the term Latin as inclusive of individuals who are Spanish speaking as well as those with family origins from non-Spanish speaking parts of Latin America.
Adapted with permission from the Giving Voice to Mothers report. 13
Methods
We examined sociodemographic data from the GVtM study, a community-based participatory research study about experiences of pregnancy and childbirth care in the United States. Service users provided input into the most accurate and respectful ways to capture sociodemographic identities. We conducted a secondary analysis of GVtM data to explore: (1) how people with multiracial identity chose to express that identity; (2) if multiracial identification is related to age, geographic region, or time in the United States; (3) demographic factors associated with differences among people adopting the specific identity of “biracial” versus those who did not; and (4) contexts related to the selection of the “other” option.
Our secondary data analysis protocol was reviewed by the University of California San Francisco Institutional Review Board (approval # 22-36248). The University of British Columbia Institutional Review Board approved the original study protocol (H15-01524).
Survey instrument development
GVtM was a community-based participatory research study that sought to describe birthing experiences of two populations that have been historically underrepresented in the U.S. patient experience literature: childbearing people from communities of color and those who planned community births (birth in homes or birth centers). A multistakeholder Community Steering Council (CSC) including service users, clinicians, community health workers, health equity and perinatal researchers with lived experiences of being minoritized, decided on the topics of study, and participated in item selection, content validation, recruitment, and interpretation of results. 13 Methods for survey development in the parent study have previously been described in greater depth.13,16
Recruitment and sample of the parent study
The GVtM study used intentional sampling, relying on evidence-based methods to reach childbearing women of color, including networking through trusted community leaders, venue-based sampling by community partners, and distribution through community-based organizations. Data collection protocols intentionally oversampled communities of color and women who sought a community birth experience. The online 218-item survey was available in English and Spanish. Several community-based partners provided internet access or “data doulas” to support participation for those with limited digital access or literacy. No financial incentives were provided for participation. Robust engagement resulted in a sample of respondents (2700) that was representative of the socioeconomic and racial/ethnic distribution reported by the U.S. census at the time.
Study measures relevant to current secondary analysis
As directed by the CSC, the original research team prioritized item selection of validated and respectfully phrased sociodemographic items, including race and ethnicity.16,17 The CSC strongly preferred self-identified versus perceived race, and they opted for an ethnoracial approach in which ethnicity was listed alongside racial categories and respondents could select all categories that applied. 18
All items were assessed by the CSC for importance, relevance, and clarity, and they were vetted by 55 representative pilot testers. Multiple consensus-seeking discussions and feedback informed the decision to go beyond the usual U.S. Census-driven categories of race and ethnicity and to perform literature reviews and environmental scans to inform the phrasing of self-identification items. The CSC and pilot testers recommended rephrasing to enhance inclusiveness. 13
The final instrument presented a combined race/ethnicity question with 14 categories, in which respondents could select all that applied. Selection of racial and ethnic categories would open branching logic such that respondents would be able to provide additional detail (e.g., respondents selecting “Black” would then be able to select from African American, Black Asian, Black Caribbean, etc.). Multiracial identity could be selected by choosing “biracial” and/or by selecting multiple categories of race/ethnicity (see Fig. 1). Open-ended text responses were available if respondents marked “biracial” and “other” categories. 19
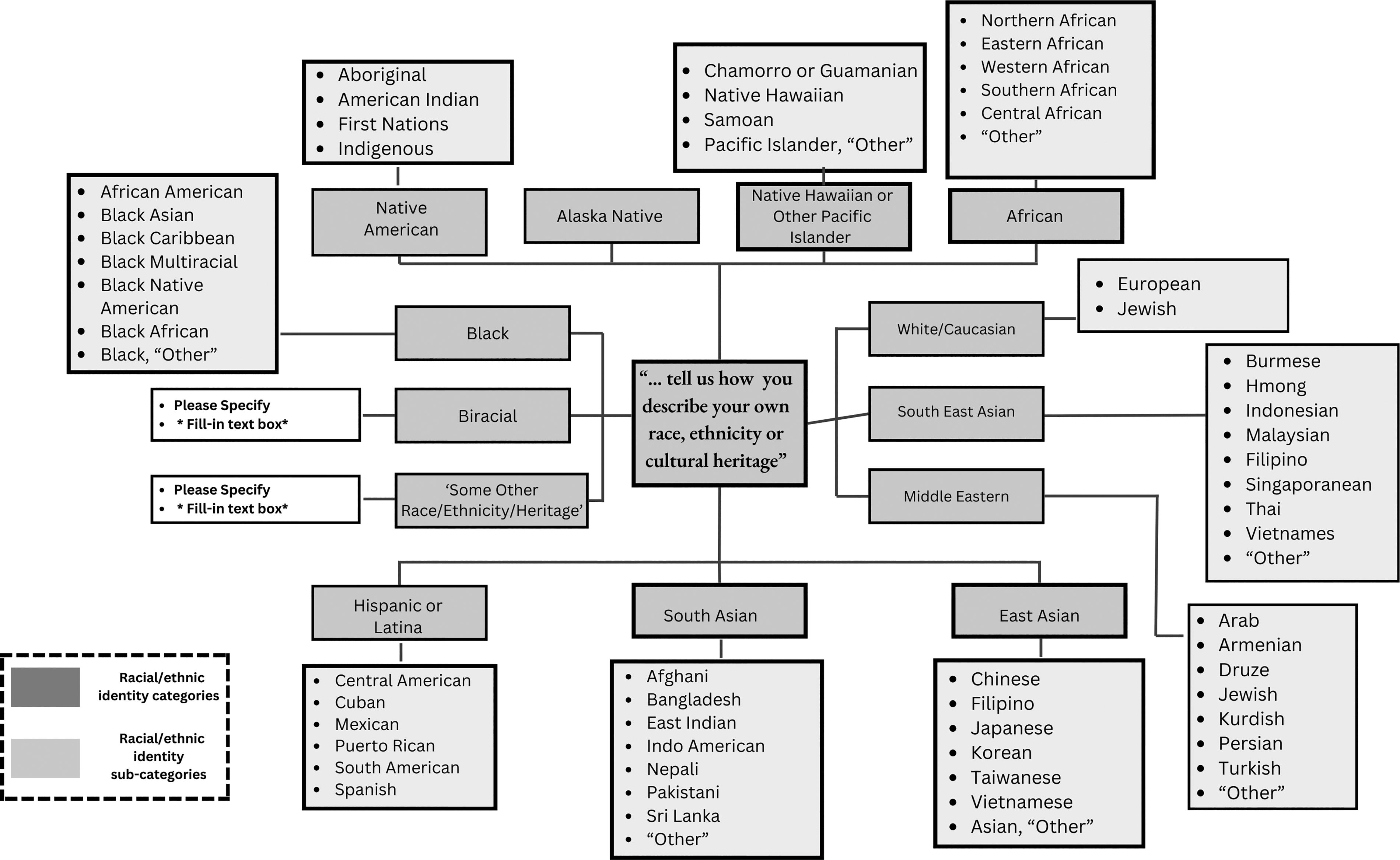
Structure of questions and sub-questions capturing self-identification of race and ethnicity in the Giving Voices to Mothers survey.
Data analysis
We used descriptive statistics such as frequencies and summary statistics to characterize the sample. We defined “multiracial” identity as being expressed through one of three mechanisms: (1) marking more than one racial/ethnic category; (2) marking the category “biracial;” or (3) providing a text response indicating multiracial identity for the “other” category. Consistent with other research, we considered individuals reporting both Latin ethnicity and another race to be multiracial. 20 We conducted bivariate testing to describe how multiracial identity broadly, and the label of “biracial” specifically, were associated with variables such as geographic region, age, education, and socio-economic status. We used descriptive statistics to describe how people selecting Latin identity responded to other racial categories and to examine the use of the “other” category as an alternative to or supplemental information about other ethnoracial categories.
Results
More than 2700 individuals from all 50 states responded to the GVtM cross-sectional survey on the experience of perinatal services in the United States. Of these individuals, 2522 respondents (93%) answered the racial/ethnic identity question.
Survey respondents were almost all between 20 and 50 years of age, with 68% between the ages of 30 and 39 at the time of the study (Table 1). Almost all had at least a high school degree, 71% had completed a 4-year college degree program, and 33% a graduate or professional degree. A quarter reported low income or having experienced social needs such as food insecurity. Private insurance covered the costs of pregnancy and birth care for more than half of respondents (57%), 21% were self-pay, and 15% were reimbursed by Medicaid. In terms of race and ethnicity, 72% reported identifying as White, 14% as Black, and 11% as Latin, with smaller proportions identifying as Native American (4%), East Asian (2%), or South Asian (1%).
Characteristics of Participants (n = 2522)
aRespondents could select more than one category, so percentages may add up to more than 100%.
“Multiracial” identity was expressed by 13.4% (n = 339) of respondents in one of several ways. The most common method was through the selection of multiple racial/ethnic categories (78%), followed by marking the category “biracial” (23%), or describing multiracial identity in an open-ended text entry (22%). People reporting multiracial identities in any of these ways were more likely than other respondents to be 29 years or younger, to live in the Southern or Western regions of the United States, to be publicly insured, and to be economically disadvantaged. They were also more likely to be born outside the United States (Table 2).
Proportion of Respondents Identifying as Multiracial, by Demographic Group (n = 339)
Socioeconomic status is a combination of variables measuring income and measures of social need, such as food insecurity, debt, and having heat or electricity cutoff.
p < 0.05.
We compared multiracial individuals who identified with the category “biracial” versus those who did not. Individuals from the Midwest or Northeast, holding vocational or bachelor’s degrees, and publicly insured were more likely to identify as “biracial” when compared with peers to expressed multiracial identity in other ways (Table 3). Most respondents (64%) who indicated Latin ethnicity did not select other racial categories (Table 4). Among those who did, the most common racial categories were White (61%), Black (25%), Native American (12%), and Biracial (12%).
Proportion of Multiracial Individuals Ascribing to the Identity of “Biracial” Versus Those Not Identifying as “Biracial,” by Demographic Group (n = 339)
p < 0.05.
p < 0.10.
Self-Identification by People Reporting Latin Identity (n = 282)
A term more commonly used in Latin American and the Caribbean to refer to Native American ancestry, “Indigenous,” was used in a follow-up question that was displayed if participants selected “Native American,” but it was not part of the response option for the primary ethnoracial identity question.
Sixty-five people selected “other” in response to the question about racial/ethnic identity. We compared open-text responses with the pre-defined option variables to assess whether the open-text responses were provided as supplemental information (indicated by marking the corresponding category and also providing a text response) or as an alternative (not selecting the category but instead providing a text response). More than half of respondents (60%) appeared to provide text responses as an alternative to existing categories, with some of the most common responses corresponding to European, Jewish, Multiracial, or West Indian ancestry or identity (data not shown).
Discussion
Results from the GVtM study reflect changing trends in ethnoracial identity in the United States and mirror national data reflecting an increase in people identifying as multiracial. We found that, compared with individuals who did not identify as multiracial, individuals identifying as multiracial tended to be younger, have lower income, be publicly insured, hold a vocational or bachelor’s degree, and be born in another country. In contrast, the term “biracial” was more often adopted in the Northeast or Midwest by individuals with higher socioeconomic status (SES). We observed that across ethnoracial categories, many people selecting the “Other” category did not simultaneously ascribe to another pre-described category, suggesting that some respondents did not feel that their identity was adequately captured by existing categories.
Our survey suggests that offering people multiple ways to express their racial identity and engaging communities in the design of ethnoracial categories may facilitate a nuanced understanding of personal characteristics that most associated with experiences of racism and mistreatment. Of note, while the most common method of expressing multiracial identity was to select multiple categories, using that method alone would have missed 22% of respondents who expressed multiracial identity through the “biracial” category or through an open-ended response. During development, the GVtM research team intentionally designed and adapted sociodemographic variables to enable respectful, inclusive, and trauma-informed data collection of personal identities and circumstances. While consistent variables are important when collecting data to enhance generalizability and comparisons in population-based research, without specificity in identity variables, it will be difficult to understand and elucidate the systemic disadvantages and risks incurred by specific marginalized groups. This is especially salient as ethnicity is highly context-specific as a potential predictor of risk for health outcomes and access to care.
Our finding that women identifying as multiracial are more likely to be younger than other respondents mirrors an increase in people identifying as multiracial. From 2010 to 2020, there was a 276% increase in people classified by the U.S. Census as multiracial, 1 underscoring the importance of capturing and analyzing identity in a way that reflects people’s lived experiences.
In accordance with demographic patterns seen for self-identification as “Latin,” we found that many individuals identifying as multiracial were college educated, 14 and as anticipated, many were from the Southern and Western regions of the country. These individuals were more likely to have lower income and be publicly insured. In addition, individuals born in other countries were more likely to endorse multiracial identity. Within the group of multiracial respondents, individuals ascribing to the specific term “biracial” were more likely to be from the Midwest or Northeast and to be publicly insured, and they were less likely to be low SES. The differences between identification as multiracial broadly and use of the term “biracial” specifically reflect the dynamic and contextual nature of ethnoracial identification that has received increasing attention by scholars.6,7,14
Our findings around Latin self-identification corroborate a large body of work, including a 2015 PEW report observing that 67% of respondents identifying as Latin did not mark another racial identity. 20 Of note, while 25% of Latin respondents to the National Longitudinal Survey espouse Indigenous racial identities, 20 only 12% of Latin respondents to the GVtM survey espoused this identity, suggesting that the category for the primary ethnoracial question (“Native American”) may not have resonated with their identity. Our analysis confirms the complexity and multiethnic nature of the Latin population and the fact that Latin or Hispanic are used as umbrella terms that mask such variation, diversity, and the need for more disaggregated data that unpack such complexity, as suggested by other authors.21,22
An alternative school of thought, espoused by the “Latino is not a race” movement, raises concerns about combining race and ethnicity questions. For example, advocates of the movement argue that a combined question could effectively reclassify many Afro Latinos as multiracial rather than Black, and they argue that this would effectively erase this group and belie important shared experiences with others identifying as Black. Advocates have proposed alternatives ranging from maintaining separate race and ethnicity questions to Dr. Nancy Lopez’s proposal to ask about “street race-gender,” in which respondents describe how others see them, which is often closely related to treatment by others. Zaire Dinzey-Flores alternatively proposed creating an Afro-Latin category within standard race/ethnicity questions. Of note, the GVtM study included a category for Afro-Latin.
Implications for research
Notably, SPD-15 was amended only once in the decades that preceded, a minor revision in 1997 that, among other actions, changed the race question to “select all that apply.” However, health researchers using the Census categories found that using that approach results in large multiracial cohorts that complicate the study of links between racialization and disparities in health outcomes and experiences. In 2023, the U.S. Census Bureau conducted a series of consultations regarding how best to categorize race and ethnicity. Our observations informed the Office of Management and Budget's update to SPD-15 in 2024. Our team provided insights during a series of consultations for the task force charged with updating the standard, based on insights from the community-informed instrument from GVtM. In 2024, SPD-15 was revised to combine race and ethnicity into a single question, add subcategories, and amend recommendations for reporting that better recognize multiracial identities.
Several specific recommendations for design of ethnoracial survey questions stemming from the GVtM study include: (1) engage service users in the design of survey questions; (2) provide multiple methods for people with multiracial identity to express that identity (e.g., selection of multiple categories, inclusion of a “multiracial” category, open-response items); (3) include examples in core ethnoracial survey questions that resonate with common demographics (e.g., the addition of examples such as “Maya” or “Quiche” as examples for “Native American,” to include Indigenous identities more relatable to Latin populations); and (4) include “other” categories to allow self-identification when existing categories do not capture self-identity.
This study was guided by social research, feminist action research, and research justice frameworks.9–12 During the development phase of the GVtM study, the Steering Council members and pilot testers prioritized self-identification racially and ethnically in ways that were meaningful to them. Some participants in the survey expressed that seeing their racial and ethnic groups represented contributed to a willingness to participate. Moreover, feminist action research seeks to empower marginalized populations and align knowledge with action. The GVtM study demonstrated disproportionate mistreatment of Black, Indigenous, and people of color during perinatal care, and those findings have been a catalyst for policy change.11,16,23 The GVtM study also resulted in the validation of several new survey instruments measuring respectful care and autonomy in decision making that have contributed to improved research and practice.16,24,25 We suggest that their novel approach to self-identification of race/ethnicity could inform future survey design.
Strengths and limitations
By using community-based participatory research methods for survey development, we were able to cocreate resonant group-specific descriptions of race and ethnicity, while also collecting population-level data in a way that can impact policy. The network-based convenience sampling strategy used was successful at reaching target audiences for the primary study and includes representation from across the United States, but additional research is needed to determine the extent to which findings can be generalized to the U.S. population. Of note, similar findings were apparent in a large similar national study in Canada. 26 The field and terms around ethnoracial identities have evolved significantly since the GVtM study was launched in 2017. The GVtM survey instrument informed the development of a large national participatory study in Canada, and the multistep process for self-identification was adopted by a Community Steering Council in Birth Includes Us, a separate community-based participatory research study focusing on the perinatal experiences of families with sexual and gender-minoritized identities.17,19
Despite our robust development process, the final instrument did not encompass all identities, underscoring the complexity of racial and ethnic self-identification. Contemporary scholars have begun to describe distinctions between self-identification, identity shared with others in different contexts, and ethnoracial identity as perceived by others.27,28 Noting this important factor and the potential for impact on experiences of health care, our subsequent national study included an item on ethnoracial identity as perceived by others. The GVtM study on the experience of perinatal services was not designed to explore other important questions such as the impact of skin tone, language, colonial histories, or immigration may impact ethnoracial identity.7,21,29
Conclusion
The GVtM model for sociodemographic data collection demonstrates how community members can inform the design of racial/ethnic categories that better reflect the lived experience and preferences for self-identification among historically underrepresented populations. In particular, instruments that allow research respondents to self-identify race and ethnicity will lead to reliable, culturally resonant datasets, and ultimately could enhance trust in findings from research on health inequities. Development of research methodologies and variables that allow for disaggregation of data in meaningful ways is critical to guide programs and policies that counteract the impact of racialized oppression.
Footnotes
Acknowledgments
The Giving Voice to Mothers study would not have been possible without the long-term commitment and participation of these members of the GVtM US Steering Council: Shafia Monroe, Paula Rojas, Marinah Farrell, Jacqueline Left Hand Bull, Roberta Eaglehorse, Claudia Booker, Vanessa Calderi, Michelle Goodwin, Zsakeba Henderson, and Jennie Joseph. Flor de Abril Cameron provided valuable input on the construction of Latin designations for this article.
Community organizations involved in study design, recruitment, and knowledge translation include: Choices in Childbirth, Every Mother Counts, the International Center for Traditional Childbearing, Mamas of Color Rising, Oregon Intertribal Breastfeeding Coalition, Phoenix Midwife, Mama Sana/Vibrant Woman, Mountain Midwifery Center, and Easy Access Women’s Health Clinic (Commonsense Childbirth).
Authors’ Contributions
M.O.R.: Conceptualization and writing—original draft. S.V.: Conceptualization, methodology, writing—review and editing, supervision, and funding acquisition. A.T.: Methodology, data curation, and writing—review and editing. M.D.: Methodology, project administration, and writing—review and editing. R.W.G.: Conceptualization and writing—review and editing. C.S.B.: Review and editing.
Author Disclosure Statement
The authors have no relevant financial or nonfinancial interests to disclose.
Funding Information
Giving Voice to Mothers was funded by the New Hampshire Charitable Foundation Transforming Birth Fund (Grant numbers 100156 and 105661).