
Abstract
Maternal and infant morbidity and mortality in the United States, particularly in Alabama, are unacceptably high and disproportionately affect Black and other marginalized communities. Community health workers (CHWs) are a promising solution to address these disparities by bridging the gap between health care systems and underserved communities. This article describes an ongoing Perinatal CHW Program conducted by ConnectionHealth in Jefferson County, Alabama, that provides wrap-around perinatal care to economically marginalized communities. The ConnectionHealth CHW program is a promising model for addressing maternal/infant health disparities. This article outlines our experience with a Perinatal CHW Program, including a training, mentorship structure, and ongoing assessment strategies that can serve as a model for others aiming to bridge the gap in their own communities.
Introduction
Maternal and infant mortality rates (MMR and IMR) remain alarmingly high in the United States (U.S.). Recent statistics reveal that the MMR in the United States was 32.9 deaths per 100,000 live births in 2021, and IMR was 5.4 deaths per 1000 live births, which rank among the highest in the industrialized world.1,2 Furthermore, for every maternal death, there are estimated to be 100 “near-miss” cases that the Centers for Disease Control and Prevention (CDC) captures in a severe maternal morbidity (SMM) composite of 21 outcomes that have profound short and long-term ramifications for both the mother and newborn.3,4 Social and structural determinants of health (SDoH) such as structural racism, neighborhood environment, education access, insurance coverage, and income disparities underpin the starkly poorer health outcomes experienced by Black and other pregnant women from historically marginalized backgrounds.5–8 Structural racism encompasses systemic conditions, for example, residential segregation, and institutional policies that systematically disadvantage individuals based on race or ethnicity, which further intersect with identities such as gender, socioeconomic status, disability, and other factors. 9 In the context of maternal and infant health, structural racism manifests through disparities in access to quality care, discriminatory practices within health care systems, and other SDoH that disproportionately affect marginalized communities. 10
Alabama’s MMR and IMR are among the highest in the United States with racial disparities across both measures: the MMR was 36.4 per 100,000 live births in 2020 (third highest in the nation) and infant mortality, while decreasing, was 6.7 deaths per 1000 live births in 2022, significantly higher than the U.S. average. 11 Quantitative data for Alabama suggest that poor maternal and infant health outcomes, including access to and use of services, are related to socioeconomic deprivation, living in medically underserved areas, Medicaid insurance coverage, and race (as a proxy for racism).8,12–16 Pregnant women in Alabama experience multiple barriers to getting perinatal care, including lack of transportation and childcare and logistical and administrative hassles, which are exacerbated by people’s lived experience of health care discrimination based on race, income level, and insurance status.17,18 There are, however growing statewide efforts to address this unjust and excessive burden of death. The Alabama Maternal Mortality Review Committee (MMRC) has provided analysis and interpretation of maternal deaths in the state since 2016, the latest of which (2018–2019) identified infection, cardiovascular conditions, and hemorrhage as the leading causes of pregnancy-related death, with most of those deaths (75%) occurring after childbirth. 9 In response to the MMRC and other data, the Alabama Maternal Health Task Force, a coalition of government agencies, and private, nonprofit, and community-based organizations, developed a strategy in 2023 to promote healthy outcomes for Alabama mothers and families. Key priority areas include strengthening the maternal health workforce and identifying and promoting programs that improve maternal health and improve people’s access to high-quality care. 9
Community health workers (CHWs) have been shown to increase access to services and improve the quality of culturally competent care, and thus, there is an urgent need and emerging strategic opportunity in Alabama to explore and test CHW programs that bridge the gap between women and evidence-based perinatal health care services. 19 Literature over the last decade on CHW programs impact on perinatal health outcomes in the United States is increasingly robust. Several large-scale, state-based programs have documented substantial improvements in birth outcomes through CHW-led interventions. The Arizona Health Start Program demonstrated significant reductions in adverse birth outcomes, including a 38% reduction in low birth weight (LBW) among American Indian mothers and a 36% reduction in very low birth weight among Latina mothers. 20 Michigan’s Maternal Infant Health Program (MIHP) documented powerful outcomes for Black women and infants who enrolled by the second trimester, with significantly lower odds of very low birth weight (OR = 0.42, 95% CI [0.30–0.61]) and very preterm birth (OR = 0.41, 95% CI [0.30–0.57]). 21 MIHP participants also had significantly higher odds of receiving any prenatal care (OR = 1.06, 95% CI [1.01–1.11]) and timely postpartum care (OR = 1.50, 95% CI [1.43–1.57]). 22 The Community Health Access Project in Ohio demonstrated similar results, with participants experiencing less than half the rate of low birth weight births compared to controls (6.1% vs. 13.0%) with an OR of 0.35 (95% CI [0.12–0.96]). 23 Similarly, the Baby Love program in Rochester, New York, showed reduced odds of preterm birth (OR = 0.56, 95% CI [0.31–1.04]) and LBW (OR = 0.62, 95% CI [0.35–1.10]) among participants. 24 Yet, our literature review found no studies or program descriptions of perinatal CHW programs in Alabama, or a “how-to” guide on how interested parties could launch a Perinatal CHW Program to bridge the gap in their own community.
Alabama’s high MMR and IMR calls for such innovative solutions. This article outlines our experience launching a Perinatal CHW Program, using the ConnectionHealth initiative as a model. It provides an in-depth look at the ongoing CHW program offering wrap-around perinatal care to pregnant women, particularly in marginalized communities in Jefferson County, Alabama’s program called From Day One (FDO).
ConnectionHealth
ConnectionHealth, is a 501(c)(3) nonprofit organization founded in December 2014 in Birmingham, Alabama, and is one of the few organizations dedicated to training and deploying CHWs to address the needs of marginalized communities in Alabama. ConnectionHealth is the only Alabama organization recognized by the National Association of CHWs. ConnectionHealth has provided services to over 40,000 community members in Jefferson County and the Black Belt Region of rural Southern Alabama, providing community-based support to assist clients in achieving healthier lives. They offer various services, including training, community partnerships, and research collaborations while receiving federal funding to prevent chronic diseases, address health equity, SDoH, and reduce mortality rates among mothers and infants.
ConnectionHealth’s Perinatal CHW Program
ConnectionHealth’s Perinatal CHW Program was designed to address persistent disparities in maternal and infant health outcomes by providing comprehensive, community-based support to underserved women. The overarching roles of ConnectionHealth Perinatal CHWs include delivering culturally competent health education, offering social support, navigating health care, and connecting parents to social and financial resources as needed.
By addressing obstacles like lack of transportation, childcare, and health care discrimination, ConnectionHealth CHWs ensure that the marginalized population receives equitable and respectful care. Each ConnectionHealth CHW supports approximately 20 clients, building trust through face-to-face contact at home visits or meetings in public spaces. This trust is further strengthened through ongoing communication via phone calls, texts, and, when permitted by clients, accompanying them to health care appointments. Within these broad roles, specific responsibilities include:
Educating/promoting positive health practices specific to the prevention of tobacco, drug, and alcohol use, healthy eating and lifestyle strategies, oral health, breastfeeding, contraception methods, infant safety, childhood injury prevention, and infant nutrition. Comonitoring blood pressure. Maintaining communication and engagement with clients from enrollment to program discharge Reminding clients of appointments and facilitating transportation by linking clients to local transport resources. Accompanying clients to prenatal, postnatal, and pediatric visits based on their preference/needs. Navigating and assisting with Medicaid enrollment Assisting in locating healthy food through grocery stores; food banks; and women, infants, and children. Connecting the clients with local diaper banks and milk banks. Project monitoring—activity and client documentation via an online database software such as the Research Electronic Database Capture (REDCap).
ConnectionHealth, in partnership with the Jefferson County Department of Health, leads the FDO Program. FDO launched in 2018 as an initiative under ConnectionHealth’s broader maternal and infant health training program structure, addressing comprehensive perinatal support. Clients are enrolled in the program through referrals from health department clinical staff, case managers, or self-referral. CHWs also engage in outreach activities within underserved neighborhoods to identify and recruit eligible pregnant women. Once enrolled, CHWs conduct an intake assessment to identify needs and begin providing wrap-around support from conception up to 12 months postpartum to clients who live in the Jefferson County area, Alabama’s fifth largest county (population of 658,466). 25 The goal of FDO is to improve health behaviors and outcomes that significantly affect maternal and infant well-being, for example, smoking cessation and postpartum care attendance.
Data collected from 2018 serve as the baseline for comparison. Notably, some variations in outcomes during 2019–2021 can be attributed to the widespread disruptions caused by the COVID-19 pandemic, which significantly impacted health care access, service delivery, and in-person outreach. Despite these challenges, the 2022 data reflect a strong recovery and increasing program effectiveness.
For smoking cessation, data from the early years of CHW implementation (2018–2021) show some variation in outcomes. In 2018, the first full year of the FDO CHW program, 71% of enrolled smokers achieved cessation. This rate declined from 50% in 2019 to 2020, likely influenced by challenges related to the COVID-19 pandemic. However, by 2020–2021, the program achieved a 100% cessation rate for enrolled smokers. This positive trend continued in 2022, with all nine smokers in the program achieving cessation.
Postpartum visit attendance showed a similar trend. In 2018–2019, again representing the early impact of CHW support, 84.4% of women completed their postpartum visits. This percentage declined during the COVID-19 pandemic to 53.8% in 2020 to 2021 but increased to 92% of participants attending their postpartum visits in 2022. While there is no available data prior to the CHW program’s launch in 2018, these year-over-year comparisons illustrate program impact over time, with improvements in smoking cessation and postpartum care attendance.
Figure 1 describes educational content and activities for each CHW-client touchpoint targeted to that point along the pregnancy to postpartum continuum. The case vignettes presented here describe the different types of support CHWs offer.
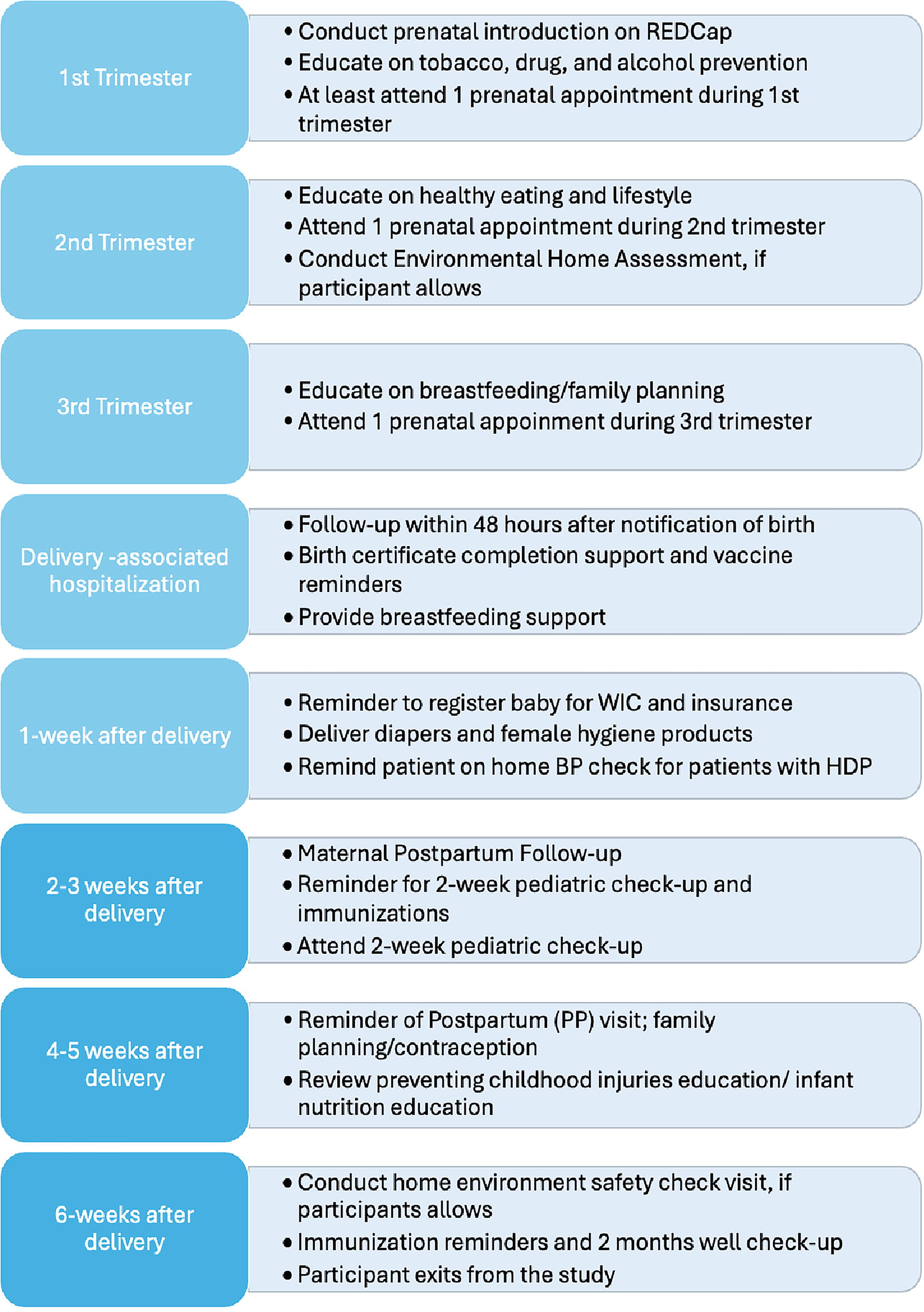
Prenatal and postpartum workflow (can be modified depending on study or program needs). HDP, hypertensive disorders of pregnancy.
“In Birmingham, Alabama, Maggy, a CHW with over eight years of experience in a perinatal program, showed attentiveness during a routine home visit. She identified a dangerous gas leak, promptly contacted the fire department, and facilitated the installation of smoke detectors, ensuring the safety of a pregnant mother and her children. This case underscores the wrap-around nature of CHW support in which CHWs pair their keen awareness of the social and physical context with their training and connections to bring life-saving services to their clients.”
“Samantha, mother of preterm twins, one of whom has cerebral palsy, faced substantial healthcare and social challenges. The twins’ health problems were exacerbated by mold in the house. Despite the formal conclusion of their initial support program, their CHW Stephanie continued to advocate for necessary medical tests and helped Samantha manage frequent healthcare visits that were disruptive to them. By facilitating access to medical care and finding safer living conditions, the CHW played a crucial role in enhancing the family’s quality of life, illustrating the importance of persistence and tailored support in community health practice.”
“Araceli, a 20-year-old woman, discovered she was pregnant and faced significant barriers to accessing healthcare. Through a perinatal CHW program, CHW Amalia built a trustful relationship with Araceli, assisting her in navigating the healthcare system and securing Medicaid benefits. Amalia’s support included overcoming language barriers, assisting with required paperwork, and empowering Araceli to understand and advocate for her rights. This case highlights the CHW’s comprehensive knowledge of healthcare systems and their ability to support individuals facing complex challenges in accessing care.”
ConnectionHealth CHW Training Curriculum Overview
ConnectionHealth partnering with multiple departments and centers within the University of Alabama at Birmingham School of Medicine, including the Diabetes Research Center, the Department of Medicine, the Divisions of Preventive Medicine, the Center for Women’s Reproductive Health, and the Department of Obstetrics and Gynecology adapted content drawn from a broad review of national certification and licensing programs, tailoring it to focus on the wide-ranging social, emotional and physical needs of clients across the pregnancy to postpartum continuum.
Perinatal CHWs employed by ConnectionHealth undergo 180 h of rigorous training that equips them to work effectively with underserved populations. The training sessions are conducted in-person and via virtual sessions, using Canvas™ as the learning management system and Zoom™ video conferencing to facilitate synchronous virtual classes. The CHW core training curriculum comprises approximately 80 h of synchronous and asynchronous instruction in the CHW core roles and competencies, as outlined by The CHW Core Consensus Project (C3 project). 26 The training includes case study reviews, group work, and role-play exercises to reinforce learning. Additionally, CHWs complete over 40 h of self-study readings, assignments, and assessments. The Foundations for Community Health Workers textbook is the main text for the core training curriculum. 27 After completing the core CHW training, Perinatal CHWs undergo an additional 30 h of specialized synchronous training in maternal and child health topics, including maternal morbidity and mortality, infant morbidity and mortality, breastfeeding support, infant safety, connecting to resources, and mental health conditions during and after pregnancy. New CHWs are matched with senior Perinatal CHWs who serve as mentors during this phase of the training process. This mentorship includes weekly check-ins, joint client visits, and real-time feedback to ensure CHWs are supported as they apply their training in the field.
Once employed, CHWs complete an additional 30 h of in-service training to strengthen their skills on the job. This in-service level training combines in-person, virtual, synchronous, and asynchronous, including reading and take-home assignments. Continuing education opportunities such as mental health first aid, suicide prevention, infectious disease prevention, chronic disease self-management, diabetes prevention, kidney health, health insurance marketplace navigator, and emergency preparedness/recovery are offered to CHWs to help them build their skills and stay up-to-date with the latest health care practices. CHWs undergo ongoing assessments, including self-evaluations and client feedback surveys. These continuous evaluations help guide skill development and ensure the fidelity to the program model. ConnectionHealth’s training program content is regularly updated based on CHW and client feedback and revised based on emerging public health issues and best practices. While live training is preferable to increase training flexibility, ConnectionHealth continues to develop on-demand modules that can be completed virtually and asynchronously.
See Table 1 for an example of ConnectionHealth’s training curriculum.
ConnectionHealth Community Health Worker Training Curriculum
CWH, community health worker.
Learning and Training Evaluation Tools
ConnectionHealth uses various tools to evaluate the CHW training. The training is led by the Director of Education who is responsible for developing, updating, and delivering the training to CHWs. The Director of Education holds a doctoral degree (PhD/DrPH) and has over 5 years of experience in community-based health education, curriculum development, and CHW workforce training. While not required, having a Certified Health Education Specialist or Community Health Worker Instructor (CHWI) credential may be beneficial for individuals in similar roles seeking to replicate this model. The director oversees the creation of training materials and ensures that the CHWs are well-prepared to address community health needs. We evaluate trainee knowledge through pre- and post-tests with multiple-choice questions and assess training acceptability through satisfaction interviews. The feedback from these evaluations helps identify areas that need improvement, which helps develop targeted training and support. Additionally, the director and CHW supervisors encourage CHW trainees to self-assess their knowledge and identify areas where they need further support by completing a skills checklist and/or self-assessment questionnaires. Once the CHWs complete their training, they are supervised in their roles by senior CHWs or former CHWs. These experienced CHWs meet weekly to provide ongoing support, guidance, and feedback as the new CHWs carry out their responsibilities in the field. The supervisors help monitor their progress in their project assignments, offer practical advice, and assist in addressing challenges they may encounter.
See Table 2 for an example of ConnectionHealth’s pre- and post-test questions.
ConnectionHealth’s Pre- and Post-Test Questions
Program Monitoring and Evaluation, Continuous Improvement and Adaptation
ConnectionHealth CHWs use REDCap, a secure web application for building and managing online surveys and databases to capture client and project data, which helps them effectively manage their large caseloads and also tailor the program to the needs of each individual client. This real-time data collection allow ConnectionHealth leadership and CHW teams to meet weekly to discuss challenges, share opportunities and resources, and check in on program milestones. Additionally, surveys and questionnaires are used to gather feedback from CHWs, clients, and other stakeholders on the program’s quality, including training. In particular, ConnectionHealth uses client satisfaction surveys, which assist in identifying areas of strength and opportunities for growth for individual CHWs and areas for improvement or expansion of the program. For example, based on client feedback, ConnectionHealth has adjusted and expanded the program to better care for individuals who have experienced pregnancy loss, have preterm babies, and other adverse pregnancy outcomes.
This case study highlights the design, implementation, and preliminary outcomes, as well as offering practical guidance on staffing, training, supervision, data use, and community engagement of the FDO Perinatal CHW Program in Jefferson County, Alabama. Developed in response to persistent inequitable maternal and infant health outcomes, this model provides a replicable framework for others seeking to develop a perinatal CHW intervention in their communities. ConnectionHealth has demonstrated how locally embedded CHWs can build trust, enhance access to care, and navigate structural barriers in real time. The program’s improvements in smoking cessation and postpartum care attendance—despite challenges such as the COVID-19 pandemic—suggest that community-based models like this one can yield tangible health benefits, particularly when CHWs are fully integrated into public health ecosystems. Ultimately, this model underscores the value of CHWs as agents of health equity and provides a concrete starting point for designing perinatal CHW programs rooted in trust, lived experience, and community voice.
Footnotes
Authors’ Contributions
All authors contributed to the opinions expressed in this article, participated in the writing or editing of the article, and agreed with its submission for publication.
Author Disclosure Statement
No competing financial interest exists.
Funding Information
ConnectionHealth is funded by the Jefferson County Department of Health. C.T. is funded by the National Institute of Health (K23HL157618). R.G.S. is funded by the National Institute of Health (K23HL195331). V.V.S. is funded by the National Institute of Health. This study received funding from the American Heart Association (Grant Numbers 22HERNCMI980273, 22HERNPMI985239, 24POST1198805, and 23CDA1048106).