Keywords: Osteochondral Lesions of the Talus, Bone Marrow Aspirate Concentrate, Lateral Ankle Ligament Reconstruction
Introduction/Purpose: Osteochondral lesions of the talus (OLTs) frequently coexist with lateral ankle instability, which can compromise cartilage repair outcomes if left unaddressed. Arthroscopic microfracture (MF) with bone marrow aspirate concentrate (BMAC) is an established biologic adjunct for cartilage restoration, yet the decision to perform concomitant lateral ligament stabilization (LLS) remains debated due to concerns about overtreatment, added morbidity and delayed rehabilitation, particularly in active individuals with equivocal instability. This study compared outcomes of MF+BMAC versus MF+BMAC+LLS, with emphasis on patient reported outcomes and patient-acceptable symptom state (PASS) achievement.
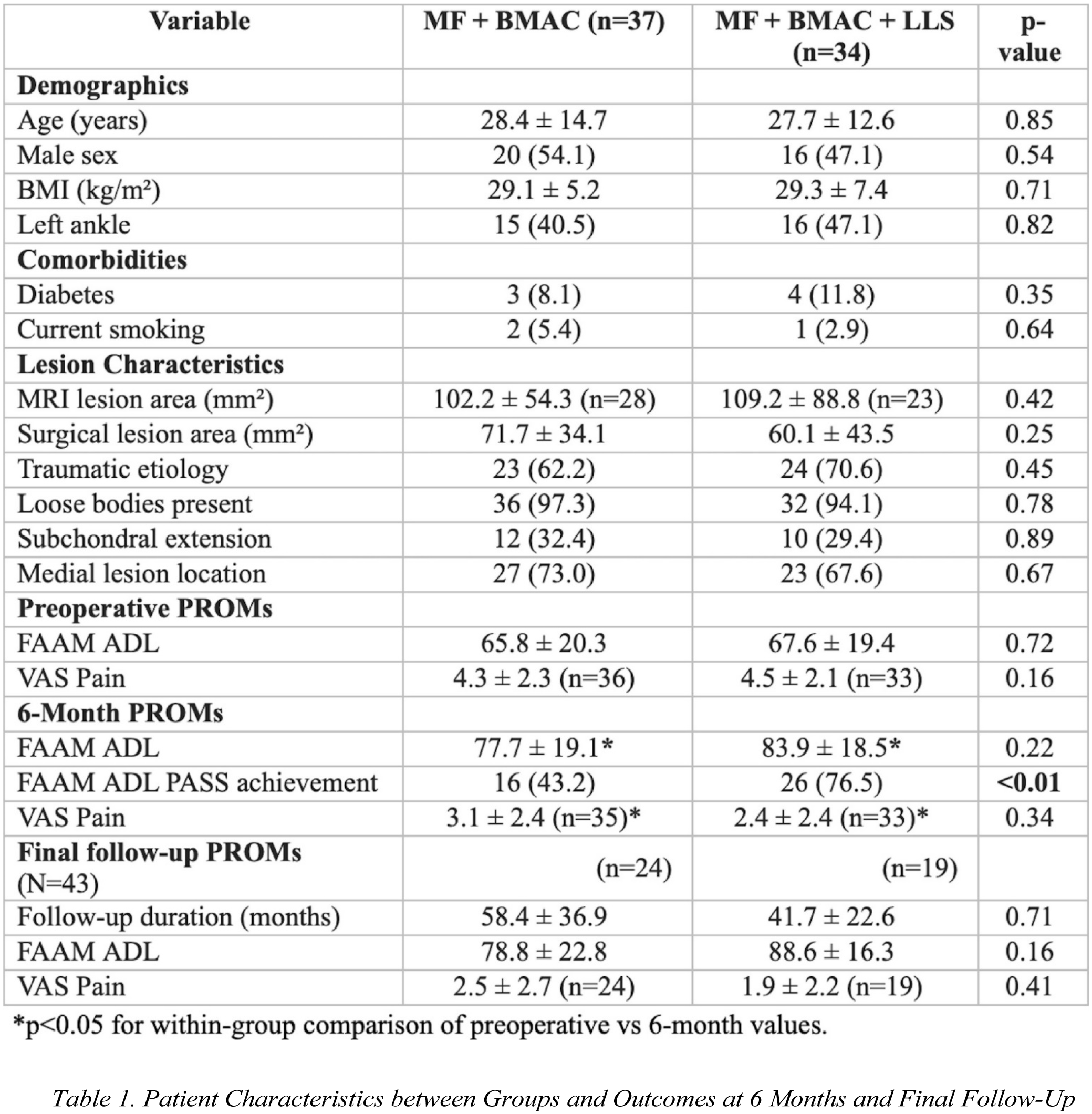
Methods: We retrospectively reviewed consecutive patients with MRI-confirmed OLTs between 2016–2024 treated by a fellowship-trained foot and ankle surgeon at a tertiary academic center. Exclusion criteria: Missing FAAM-ADL and PASS data at baseline and 6-months postoperatively. Patients were stratified by presence of clinical instability: MF+BMAC (n=37) and MF+BMAC (n=34). Arthroscopic MF used a standard technique, BMAC was harvested and concentrated per institutional protocol and applied to the prepared defect, LLS used a modified Broström-Gould. Demographics, comorbidities, and lesion characteristics were compared between groups. Patient-reported outcomes included FAAM-ADL, VAS Pain, and PASS rates preoperatively, at 6-months, and at final follow-up (>1 year). Independent/paired t-tests and chi-square tests used (with significance at p<0.05).
Results: At 6 months, LLS+BMAC demonstrated a significantly higher PASS rate (76.5% vs 43.2%, p<0.01). Both cohorts achieved significant within-group FAAM-ADL improvement from baseline (p<0.05), with no decline between 6-months and final follow-up (mean 51.0±32.2 months). FAAM-ADL scores remained high (88.6 LLS vs 78.8 non-LLS, p>0.05) and pain scores low (VAS 1.9 vs 2.5, p>0.05) in both groups.
Conclusion: For OLTs with clinical instability, adding LLS to MF+BMAC significantly improves early PASS achievement at 6-months and may facilitate earlier return to activity without penalty. This data supports selective stabilization, particularly in active patients with equivocal or suspected instability, as part of a comprehensive strategy.