Introduction/Purpose: Foot and ankle osteoarthritis (OA) may affect the subtalar, tibiotalar, or both joints, yet the morphological factors that differentiate these variations remain poorly understood. Traditional 2D radiography often fails to capture the complexity of the foot and ankle, limiting the ability to identify subtle shape differences that may explain progression and onset of OA. Statistical shape models (SSMs) are able to quantify and compare joint morphology across populations and may offer new insights into the different presentations of OA in the foot and ankle. With this, the objective of this study was to assess different presentations of hindfoot ankle OA using weightbearing computed tomography (WBCT), statistical shape modeling and radiographic measurements from 3D data.
Methods: WBCT data from 189 patients (50 subtalar OA (STOA), 44 tibiotalar OA (TTOA), 45 subtalar and tibiotalar OA (TTSTOA), and 50 non-OA) were retrospectively collected with IRB approval. A 14-bone SSM was created from this data. Principal component analysis (PCA) was used to characterize variation patterns derived from the shape model. Parallel analysis identified and retained meaningful components, and a one-way ANOVA (α = 0.05) evaluated group-wise differences across each retained PCA mode. Hotelling’s T2 test identified localized correspondence particle differences between the mean shapes of each group. In-house MATLAB code calculated Meary’s angle (MA), calcaneal inclination (CI), and hindfoot ankle alignment (HAA) angles from 3D bony segmentations to assess arch height and varus/valgus hindfoot alignment.
Welch’s ANOVA with Games-Howell post-hoc (α = 0.05) identified significant differences in measurements between the groups.
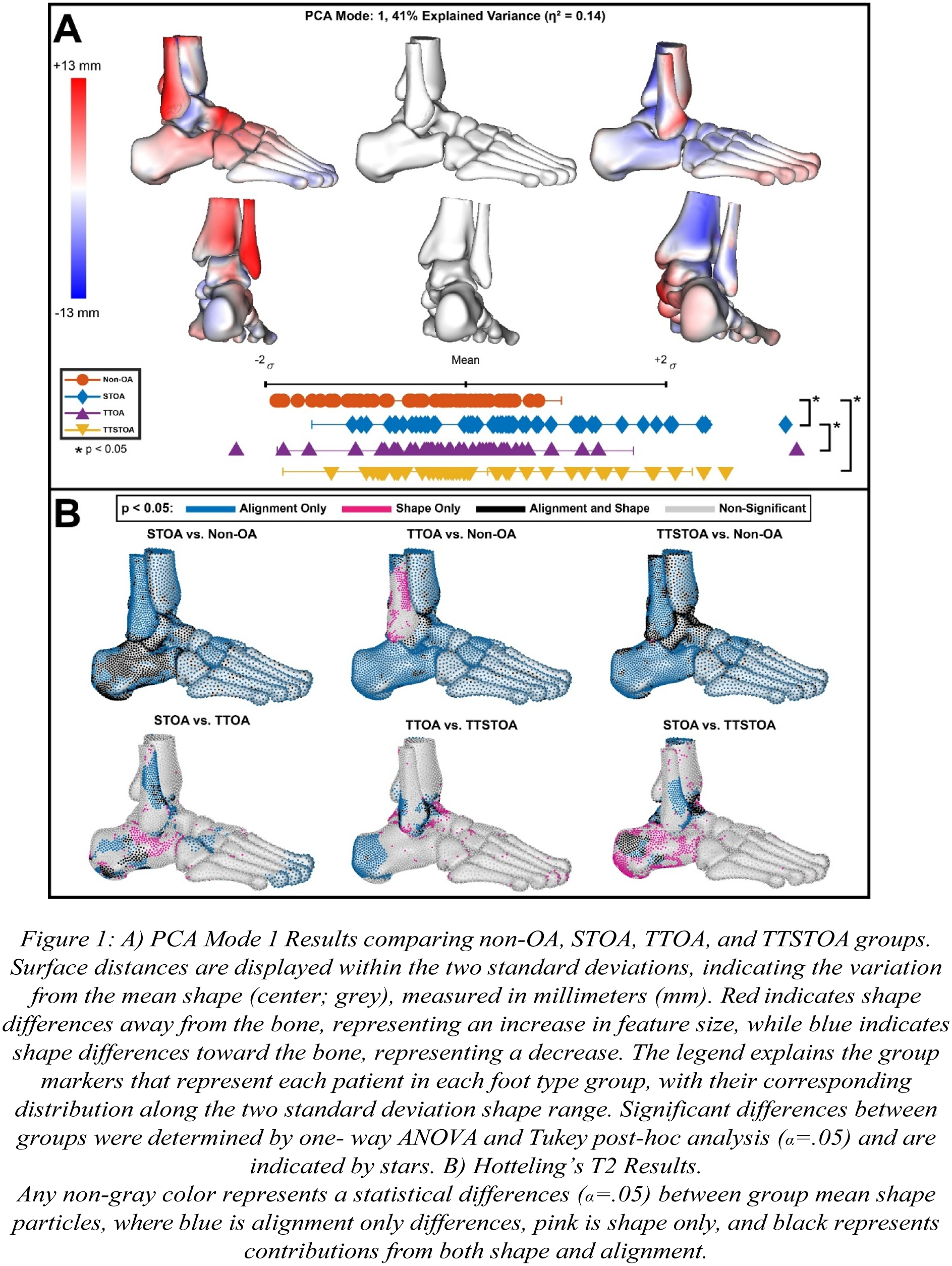
Results: PCA mode 1 (hindfoot alignment and arch height) distinguished non-OA from STOA and TTSTOA, as well as STOA from TTOA. Mode 2 (fibular alignment, arch height and impingement) demonstrated progressive variation across groups, with TTSTOA spanning the full distribution. Modes 4, 6, and 10 identified differences between non-OA and all OA groups, and were driven by fibular alignment, subtalar/tibiotalar joint space narrowing, and calcaneal facet changes. Hotelling’s T2 test confirmed group mean differences, with talar and calcaneal shape-driven differences between TTSTOA and STOA/TTOA, and fibular alignment distinguishing STOA from TTOA. Compared with non-OA, the OA groups had calcaneal and talar driven morphological differences. Hindfoot alignment was significantly more valgus in STOA and TTSTOA compared with non-OA and TTOA, aligning with shape-derived differences mentioned above.
Conclusion: Distinct morphological characteristics were identified for OA presentations at the subtalar and tibiotalar joints, with TTSTOA spanning the broadest variation, supporting its role as an advanced disease state. STOA exhibited hindfoot valgus, while TTOA had higher calcaneal inclination and varus alignment. Many of the morphological differences identified align with literature and clinical observations. These differences, confirmed by SSM and radiographic measures, highlight that each OA variation has unique presentations in alignment and shape. Recognizing these patterns could improve diagnostic precision, inform prognosis, and guide joint-preserving fusion strategies, underscoring the clinical value of SSM and WBCT beyond conventional radiography assessment.