Keywords: Total Ankle Arthroplasty, Subtalar Arthrodesis, Clinical Outcomes
Introduction/Purpose: Previous literature reports variable outcomes for concomitant total ankle arthroplasty (TAA) with subtalar arthrodesis (STA). Several studies suggest higher failure and nonunion rates than isolated procedures. Approximately one in seven TAA patients undergo concomitant STA for subtalar pathology refractory to conservative management. However, the specific contributors to failure remain poorly defined, and results across cohorts are inconsistent. Biomechanical investigations also conflict regarding the clinical impact of altered hindfoot mechanics after STA. Moreover, staging procedures in patients with comorbidity can increase anesthetic exposure, prolong rehabilitation, and escalate healthcare costs. This study evaluated outcomes of concomitant TAA with STA and sought to identify factors associated with failure and nonunion, emphasizing implant design features and surgical technique variables that might influence union and survivorship in this challenging population.
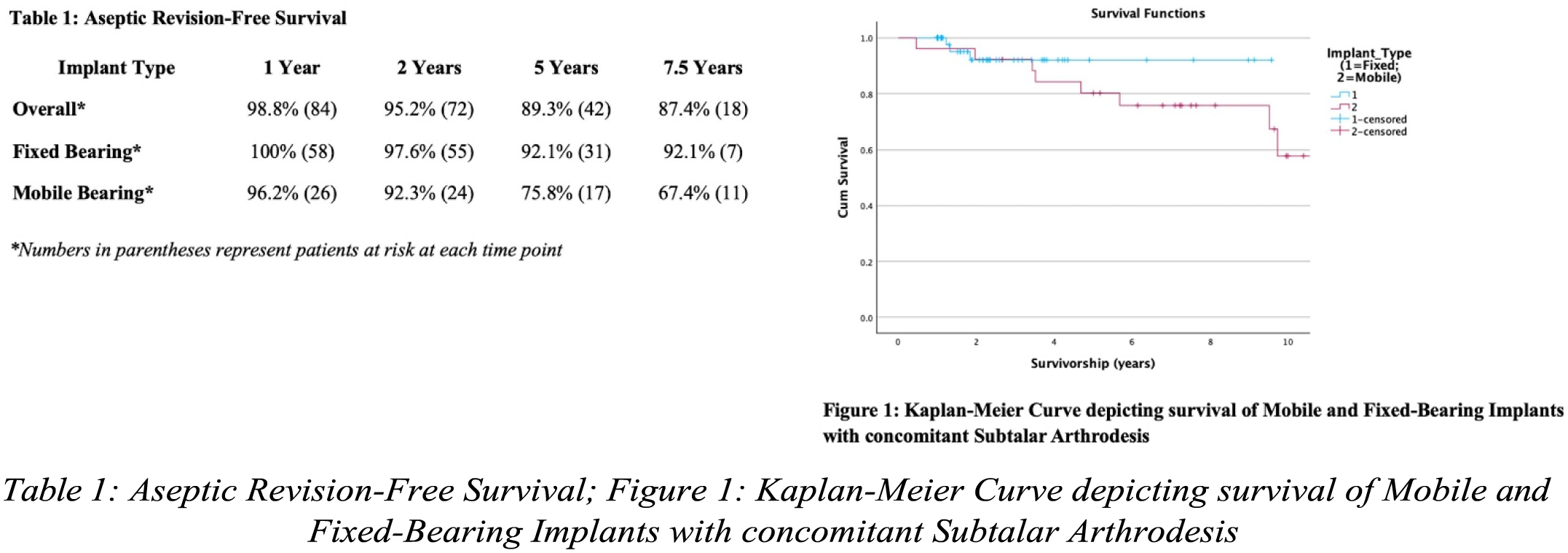
Methods: We conducted an IRB-approved, single-center retrospective cohort study of consecutive primary TAA with simultaneous STA performed between 2010-2023. Exclusion criteria included revision total ankle replacements, staged procedures, total talus replacements, triple arthrodesis, midfoot fusion, or <1-year follow-up. Three implant systems were utilized: STAR (mobile-bearing), INFINITY, and INBONE II (both fixed-bearing). Primary endpoints were aseptic TAA revision (removal/replacement of metal components, conversion to arthrodesis) and radiographic subtalar union rates assessed by plain radiography and computed tomography when indicated. Cases of periprosthetic joint infection were excluded from survivorship analysis. Revision-free survival was analyzed using Kaplan-Meier methodology comparing fixed versus mobile bearing implants. Secondary outcomes included complications requiring re-operation. Statistical analysis utilized chi-square tests and Fisher exact tests. Significance was set at P<0.05.
Results: 87 ankles in 85 patients (55 males, 30 females, mean age 65.2±9.5), follow-up 4.4 years (range 1– 13.5). TAA revision 17% (15/87), time to revision 43.7 months. Three revisions for deep infection excluded, yielding aseptic revision 14.3% (12/84). Mobile-bearing implants had higher aseptic failure than fixed- bearing (34.6% vs 5.2%, p<0.001). Subtalar fusion 81.6% (71/87). STA failure: seven nonunions and nine partial unions (six asymptomatic). Failed STA predicted TAA failure: 6.66-fold higher revision risk (56.3% vs 8.5%, p<0.001) with partial/nonunion. Fusion differed by bearing: fixed 86.9% vs mobile 69.2% (p=0.043). Complications in 25%: hardware removal 18%, arthroscopic debridement 17%. No associations between revision risk or nonunion and age, BMI, diabetes, smoking, etiology, corticosteroid injection, BMAC, or graft type.
Conclusion: Concomitant TAA with STA, when necessarily indicated, achieves excellent function without compromising implant longevity when implants and technique are selected appropriately. Bearing design is pivotal: mobile-bearing implants showed higher failure and inferior fusion than fixed-bearing designs, noting their longer mean follow-up (8.3 vs 2.6 years). Even mobile-bearing “failures” retained good long-term function, one bilateral patient experienced a decade of activity before revision. Fixed-bearing outcomes approximated isolated procedures reported in the literature. Surgeons can offer this combined procedure, counseling that despite reduced hindfoot adaptability on uneven terrain, patients could expect pain relief, improved walking ability, and high satisfaction and functional gains.