Introduction/Purpose: Minimally invasive metaphyseal transverse and Akin osteotomies (META) have gained global popularity, with satisfactory mid- and long-term outcomes. Various instrumentation systems have been developed to guide bone correction and screw placement. These systems aim to reduce the learning curve, improve deformity correction, and optimize screw placement. To date, no comparative studies have evaluated the outcomes of the conventional unguided technique and the guided technique using instrumentation.
Methods: This retrospective cohort study included patients with symptomatic hallux valgus who underwent surgery using the META technique performed by two fellowship-trained foot and ankle surgeons with over 10 years of experience. The first 20 feet operated on by each surgeon were included, with a total of 40 patients included in the study. One surgeon began their learning curve using the standard technique without a guide jig (NG), whereas the other surgeon began with the guided jig technique (GT). Functional outcomes were assessed using the Manchester-Oxford Foot Questionnaire (MOXFQ) preoperatively and at one-year follow- up. Weight-bearing radiographs were used to measure pre- and postoperative parameters, including the hallux valgus angle (HVA), intermetatarsal angle (IMA), proximal IMA, sagittal angulation, and anterior and lateral head translation percentages. Complications were recorded from medical charts during a minimum of one year of follow-up and were compared between the groups.
Results: All MOXFQ domains showed significant improvement (p < 0.05) in both groups, with no significant differences in the magnitude of improvement between the two techniques (p < 0.01). Significant correction was achieved in both groups for HVA, IMA, and proximal IMA. No significant differences were found between the groups in terms of the magnitude of correction for HVA (p = 0.39) or IMA (p = 0.41). However, the GT group showed significantly greater correction of the proximal IMA angle (p < 0.01) and head translation percentage (p = 0.02). First-TMT Slippage was significantly higher (p< 0,01) in the GT group (55%) than in the NG group (10%). The complication rate was 20% in the NG group and 25% in the GT group, with no statistically significant difference.
Conclusion: Percutaneous META osteotomy, with or without a guide jig, yielded comparable clinical and radiological outcomes. However, the guided technique results in greater proximal segment medialization and head translation, leading to more distal screw positioning and a wider midshaft foot width postoperatively. The use of a jig in this study was significantly related to postoperative 1st TMT joint slippage. The long-term implications of this compensatory locking effect warrant further investigation. The complication rates were similar between the groups during the follow-up period.
Six different measurements were defined to compare the deformity correction achievements of both techniques
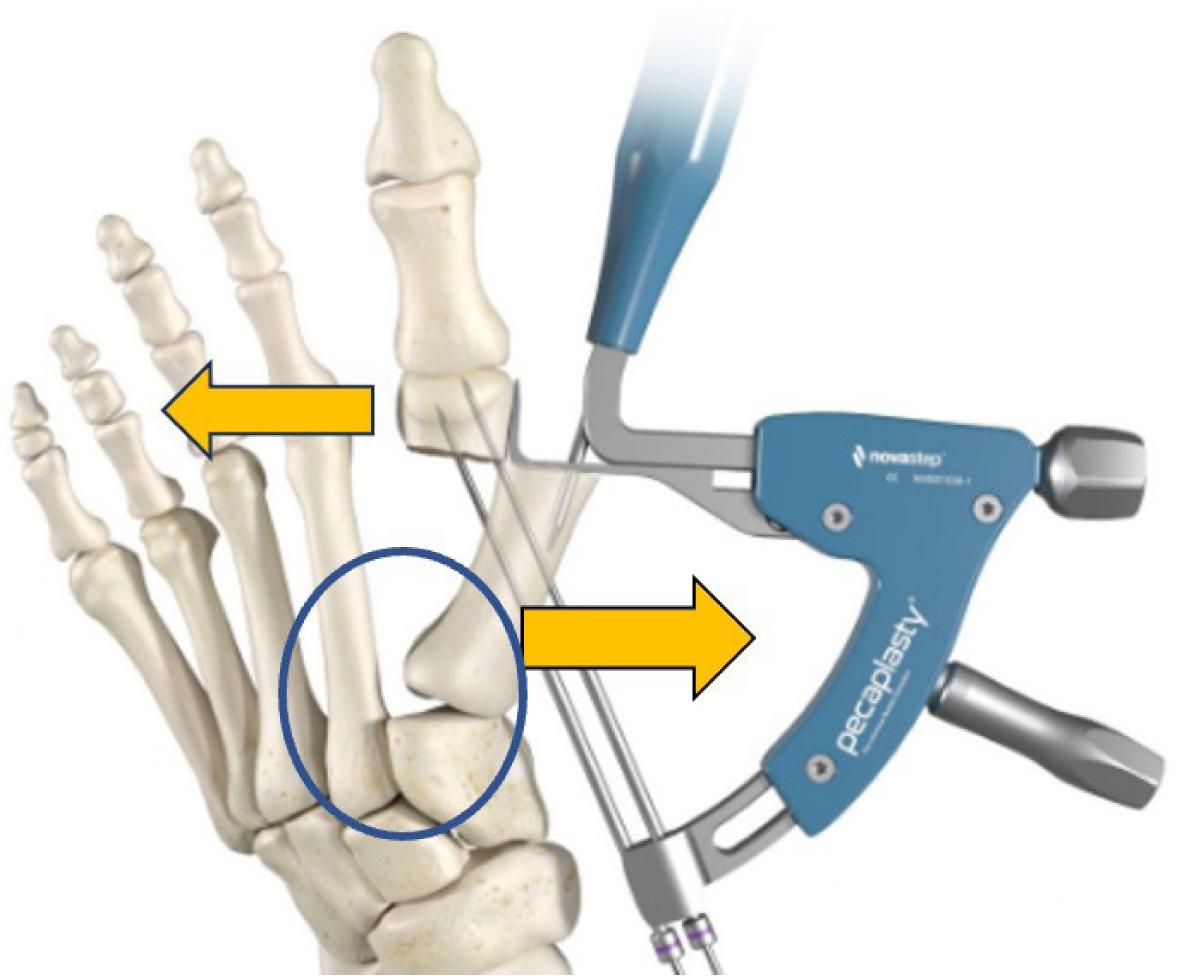
In this set of patients the use of a corrective jig was related to a higher proximal IMA angle and head shift with a significant higher rate of 1st - TMT slippage.