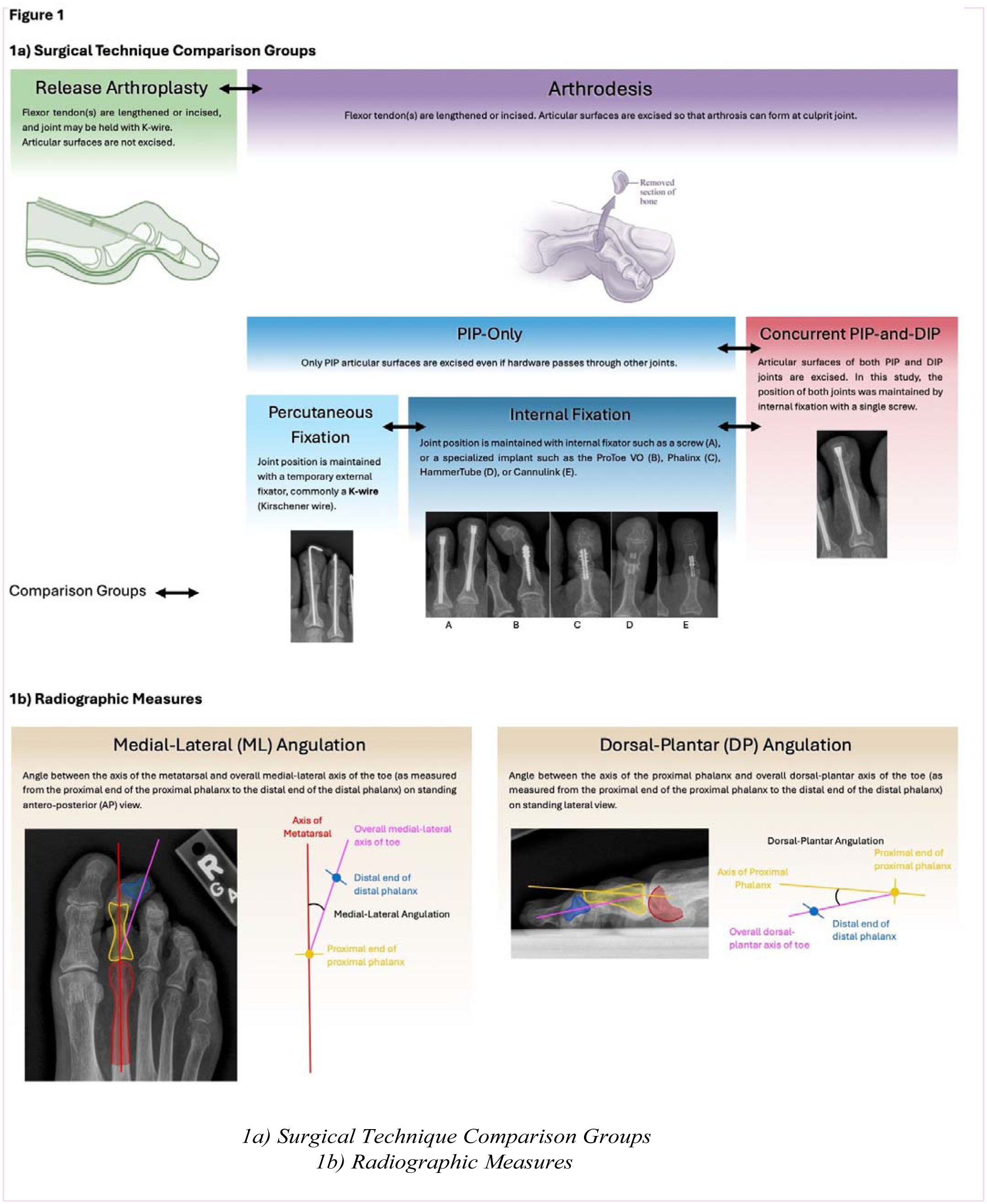
Introduction/Purpose: Hammertoes, claw toes, and mallet toes are common deformities of the lesser toes. Most result from excessive extension across the metatarsophalangeal (MTP) joint, which can beget contracture of the proximal interphalangeal (PIP) and/or distal interphalangeal (DIP) joints. Common surgical options include release arthroplasty or arthrodesis. Arthrodesis can be performed through internal fixation (implants) or percutaneous fixation (K-wires), either with PIP preparation alone or with both the PIP and DIP joints concurrently (Figure 1a). Concurrent PIP-and DIP fixation has been proposed to yield a straighter construct and reduce recurrent deformity but may increase complication risks due to additional surgical sites. The purpose of this study was to compare surgical outcomes, complication rates, and patient-reported measures among release arthroplasty, PIP-only arthrodesis, and concurrent PIP-and-DIP arthrodesis techniques.
Methods: A retrospective chart review was conducted of all lesser toe surgeries performed at a single academic orthopedic department over four years. Preoperative demographics and comorbidities relevant to surgical healing were collected. Surgical technique comparison groups (Figure 1a) included release arthroplasty versus arthrodesis. Further, within arthrodesis, comparisons were made between concurrent PIP- and-DIP fusion versus PIP-only fusion, within PIP-only fixation– between internal versus percutaneous fixation. Outcomes were assessed per surgical case for complications and, when available, per toe for radiographic and patient-reported outcomes (PROs). PRO measures included Pain Interference (PI) and Foot and Ankle Outcome Scores (FAOS). Radiographic measures (Figure 1b) included medial-lateral (ML) and dorsal-plantar (DP) angulation. Statistical comparisons were made between surgical comparison groups for complication rates, PROs, and radiographic correction.
Results: A total of 173 cases were reviewed: 45 release arthroplasty, 128 arthrodesis (49 concurrent PIP-and- DIP fusion fixation, 47 PIP-only fusion, 32 PIP-only percutaneous fixation). Minor complications occurred in 30% and major complications in 16% of cases. Non-union or recurrence was higher in PIP-only versus PIP- and-DIP arthrodesis (18% vs 2%). Hardware failure was more common in arthroplasty (10% vs 0%). Revision surgery and hardware removal occurred in 9% overall, significantly higher in release arthroplasty than arthrodesis (16% vs 6%). In the PRO subset (41 cases, 87 toes), all groups showed significant FAOS improvement, while PI scores remained unchanged. Radiographs demonstrated improved alignment in all groups, with arthrodesis achieving better ML and DP angulation than arthroplasty, and concurrent PIP-and- DIP arthrodesis achieving the best DP angulation.
Conclusion: Arthrodesis, compared with release arthroplasty, is associated with fewer complications, lower revision rates, and straighter toes. Within PIP-only arthrodesis, internal and percutaneous fixation demonstrated similar favorable outcomes. Importantly, concurrent PIP-and-DIP arthrodesis resulted in the lowest recurrence rates and the most favorable dorsal-plantar alignment, despite theoretically higher complication risk. Patient-reported outcomes improved equally across all techniques, indicating comparable symptom relief regardless of approach. These findings suggest that while all methods are effective for improving function, arthrodesis—particularly concurrent PIP-and-DIP arthrodesis—offers superior structural correction and durability in the surgical management of lesser toe deformities.