Introduction/Purpose: Patient-Reported Outcome Measures (PROMs) are invaluable tools to measure and record individual and population responses to treatment, but their collection burdens patients, clinicians, and health care systems with often lengthy and time-consuming questionnaires. We developed the Universal Pain and Function score (UPAF) with only two questions to address this burden: the Visual Analog Scale for pain (VAS) and the Single Assessment Numerical Evaluation for function (SANE). We tested the hypothesis that UPAF is valid, reliable, and responsive for surgeries below the knee.
Methods: Between August 2023 and June 2025, VAS, SANE, PROMIS Global mental health (PROMIS- GMH), PROMIS Physical Function 10b (PROMIS-PF), and Satisfaction with the Outcome of Surgery (SOS) were prospectively collected from 355 patients before and at least 60 days after below knee orthopedic surgeries. UPAF was calculated as [10 * (10 - VAS) + SANE] / 2. Validity was measured using the concepts of convergent, discriminant, and concurrent-criteria validity by calculating Spearman rank order correlation (ρ) between UPAF and PROMIS-PF, PROMIS-GMH, and SOS. Reliability was assessed using the concepts of internal consistency and measurement error by calculating the Spearman rank order correlation (ρ) between VAS and SANE and by calculating the Standard Error of Measurement (SEM), Smallest Detectable Change at 95% confidence (SDC-95), and floor & ceiling effects. Responsiveness was measured using Cohen’s d, standardized response mean (SRM), and the correlation between change in UPAF and change in PROMIS-PF.
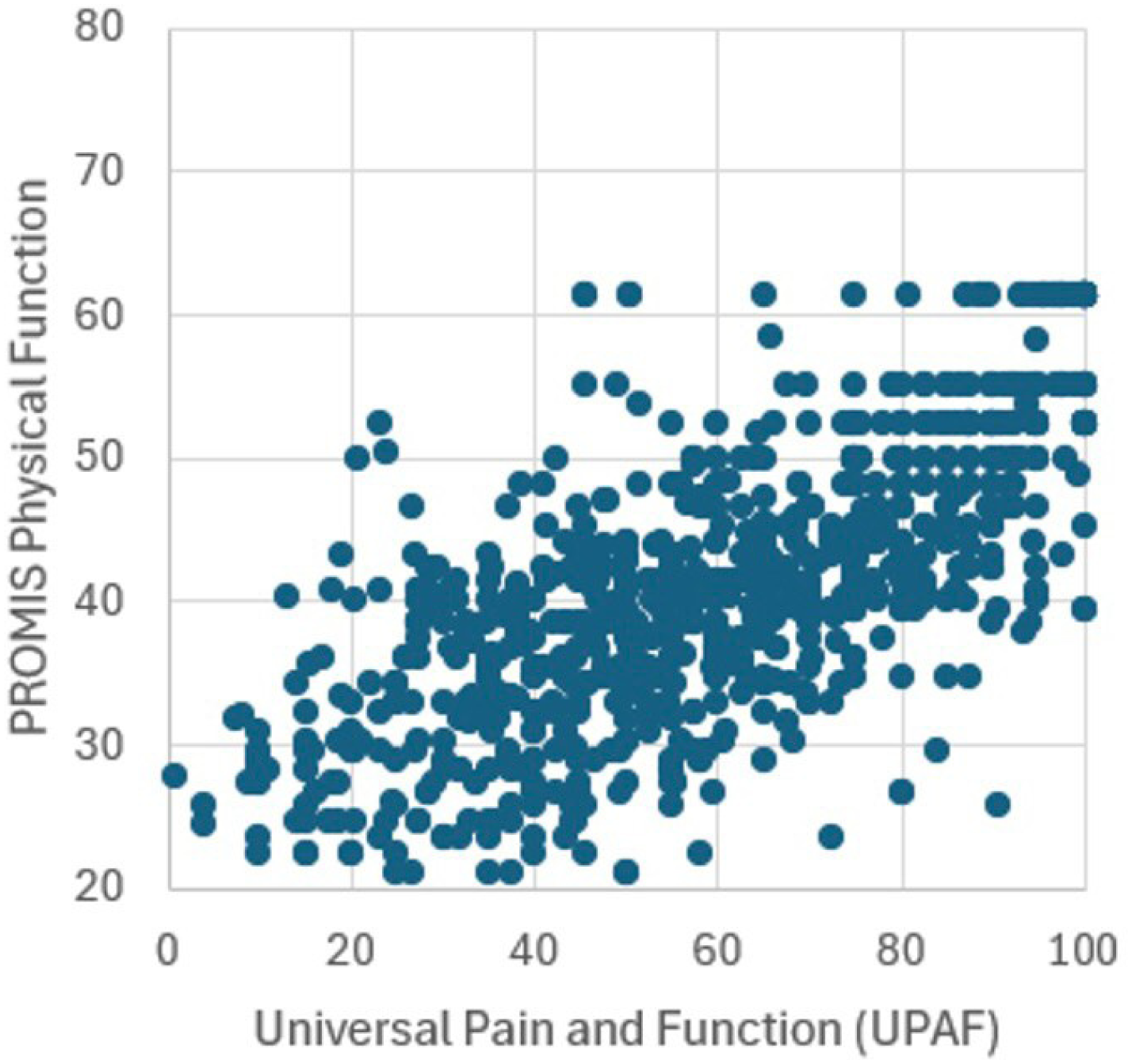
Results: UPAF strongly correlates with PROMIS-PF (ρ=0.71) confirming convergent validity (Fig-1), but not with PROMIS-GMH confirming discriminant validity (ρ=0.18). UPAF moderately correlates with SOS indicating concurrent-criteria validity (ρ=0.46), which is superior to PROMIS-PF (ρ=0.33). VAS and SANE moderately correlate, confirming internal consistency without redundancy (ρ=-0.44). SEM ranges from 6.57- 10.23, and SDC-95 (18.21 to 28.35) is less than change in UPAF for all time points, demonstrating measurement reliability. Floor-ceiling effects are seen in 1.05%-1.58% of preoperative and 0%-4.42% of postoperative patients, respectively. The effect size of surgery is very large for UPAF (Cohen’s d 1.22, SRM 1.10), which exceeds PROMIS-PF (Cohen’s d 1.02, SRM 0.85). Furthermore, the change in UPAF very strongly correlates with the change in PROMIS-PF (ρ=0.89), which confirms UPAF’s responsiveness.
Conclusion: UPAF only requires two questions to deliver a valid, reliable, and responsive measure of outcomes after orthopedic surgeries below the knee. It correlates well with PROMIS-PF and SOS and appropriately does not correlate with PROMIS-GMH. Its component questions measure similar concepts without redundancy, and it reliably delivers measurable changes greater than SDC-95 after surgery with small floor and ceiling effects. Its effect size is comparable to PROMIS-PF, making it suitable for studies requiring limited sample sizes. Surgeons and health care systems wishing to measure surgical outcomes should consider this two-question score given its decreased survey burden, validity, reliability, and responsiveness.
Universal Pain and Function Score (UPAF) strongly correlates with PROMIS Physical Function (ρ=0.71) indicating convergent validity between the two patient reported outcome measures.