Introduction/Purpose: Approximately 30% of patients with hallux valgus (HV) have concomitant metatarsus adductus (MA), which is characterized by adduction of the lesser metatarsals. MA complicates the surgical management of HV because it obstructs the first-second intermetatarsal space. This leads to higher recurrence rates and decreased patient satisfaction following surgery. To optimize surgical intervention, it is crucial to understand the three-dimensional deformity of MA. The primary aim of this study was to determine if there are differences in lesser metatarsal rotation between HV patients with and without MA. Secondary aims were to investigate differences in hallux valgus angle (HVA), the triplanar angle of pronation (TAP), sesamoid station, and first-second intermetatarsal angle (IMA) between the two groups.
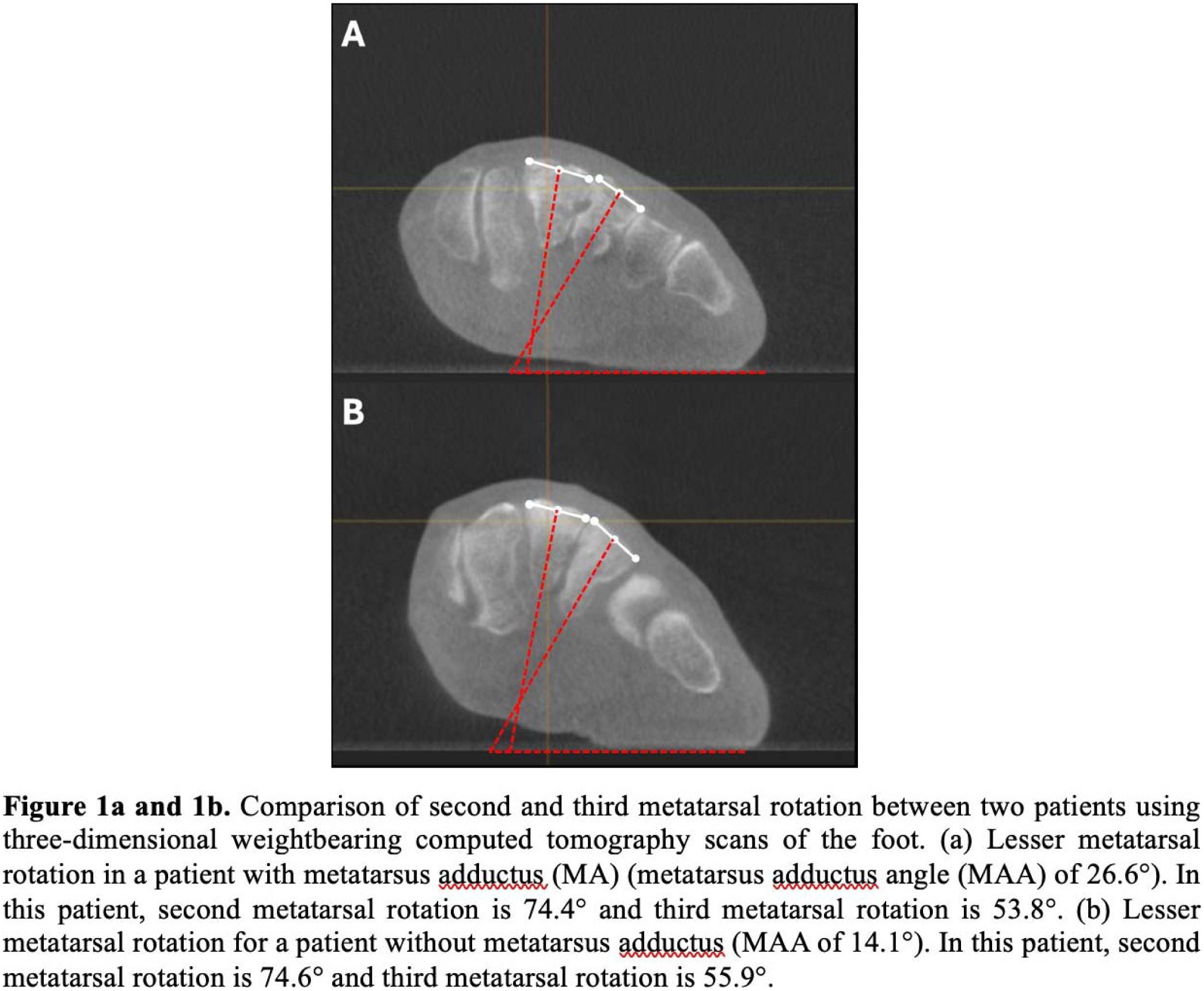
Methods: This retrospective study included patients with a primary diagnosis of HV who were treated at single academic institution between 2017-2023. Patients were included if they had preoperative weightbearing anterior posterior (AP) radiographs and weightbearing CT (WBCT) scans of the foot. Patients who previously underwent ipsilateral forefoot surgery were excluded. Metatarsus adductus angle (MAA), HVA, IMA, TAP, sesamoid station, and first metatarsal rotation were measured as previously described in the literature. To quantify second and third metatarsal rotation, novel measurements were designed and completed by two independent raters (Figure 1). Reliability was assessed using Intraclass Correlation Coefficients (ICC). Differences in radiographic and WBCT measurements between HV patients with and without MA were determined by dichotomizing patients into two groups based on an MAA cutoff of 20°. Multivariable linear regressions were used to investigate the relationships between MAA and other radiologic variables after controlling for age, sex, and body mass index.
Results: 124 patients (mean age 53.1±12.3 years) were included. The average HVA and MAA were 31.8°±8.9° and 20.57°±6.19°, respectively. Intra-rater and inter-rater reliability was greater than 0.70 for all measurements. Patients with MA had a larger HVA than patients without MA (Difference: 3.36°, 95% CI, 2.13°-8.25°). Patients with MA had greater supination of the first and second metatarsals compared to patients without MA (First: 2.33°, 95% CI, 0.29°-3.57° and Second: 2.14°, 95% CI, 0.16°-4.12°, respectively). This relationship was not observed for the third metatarsal. MAA was positively correlated with HVA (Correlation Coefficient (CC): 0.28, p<0.001) but negatively correlated with IMA (CC: -0.53, p<0.001). There was no association between MAA and TAP or sesamoid station.
Conclusion: Patients with HV frequently present with concomitant MA, which complicates surgical management. In this patient population, correcting the IMA may require addressing the second and third metatarsals due to the correlation between increased MA severity and worsening HVA in the setting of a smaller IMA. Despite this, our study suggests that there are minimal differences in the rotational deformities of the first through third metatarsals between HV patients with and without MA. Consequently, surgical correction of the metatarsals in HV patients with MA may primarily focus on correcting the deformity in the axial plane.