
Abstract
Background:
Hallux valgus is a common forefoot deformity. Sensory complications after correction can result from iatrogenic injury to the medial branch of the medial dorsal cutaneous nerve (MDCNm), lateral dorsal cutaneous nerve (LDCN), medial plantar cutaneous nerve (MPCN), and lateral plantar cutaneous nerve (LPCN). We synthesized evidence and landmarks to aid nerve identification and reduce injury.
Methods:
Following PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines, PubMed, Embase, and Cochrane were searched to February 2025 using ‘nerve anatomy’, ‘hallux valgus’ and ‘bunion’. English/French studies describing course, measurements or localization of hallux sensory nerves from the first tarsometatarsal to interphalangeal joints were included.
Results:
From 863 records, 13 studies were included comprising cadaveric, imaging, and clinical series with both normal and hallux valgus feet. Evidence was most robust for MDCNm localization. Palpation during resisted hallux extension and targeted ultrasonography were reported as low-cost methods to define the MDCNm in relation to the extensor hallucis longus (EHL). Palpation showed 100% sensitivity (positive predictive value [PPV] 99%), whereas novice ultrasonography achieved 75% sensitivity (PPV 100%) in cadaveric feet before dissection. At the metatarsophalangeal (MTP) level, a transverse ‘clock-face’ reference (EHL at 12 o’clock) typically locates the MDCNm between 10 and 12 o’clock for a right foot. A communicating dorsoplantar ‘sentinel’ vein crosses the MDCNm about 2 cm proximal to MTP, with the nerve running deep to the vein. Limited data place the LDCN at 11-12, LPCN at 5-6 and MPCN at 7-8 o’clock. Most maps were derived from non-deformed feet. Hallux valgus severity shifts the MDCNm-EHL intersection proximally and may widen the medial danger zone to ~19 mm. Ultrasonography suggests MPCN lies within 3 to 4 mm of the metatarsal head and medial sesamoid, helping define capsulotomy limits; data for LPCN remain still limited.
Conclusion:
Combining palpation, ultrasonography and vein-based landmarks with awareness of axial danger zones may reduce sensory nerve injury during hallux valgus surgery; clinical validation in deformed feet remains necessary.

Background
Hallux valgus (HV), the most common forefoot deformity with a reported prevalence of approximately 35% in the general population, remains primarily treated with surgery. 1 However, postoperative complications and complaints are not uncommon, a proportion of which are related to neurological injury. 2 The literature reports postoperative discomfort in 30% to 65% of patients, with severe forms occurring in 3% to 8%.3 -9 Although most of these symptoms resolve over time, up to 0.5% of patients may experience permanent sequelae. 10 Regardless of surgical technique, iatrogenic nerve injury is a substantial risk. Therefore, new surgical approaches, particularly percutaneous techniques, require a precise understanding of the regional anatomy and safe zones to minimise the risk of iatrogenic neurological damage.
The hallux is innervated by 4 main sensory nerves.11,12 The plantar medial digital nerve of the hallux (MPCN) is a direct branch of the medial plantar nerve, whereas the plantar lateral digital nerve of the hallux (LPCN) corresponds to the medial branch of the first common plantar digital nerve. Both nerves arise from the tibial nerve and provide sensory innervation to the plantar aspect of the hallux. The medial dorsal cutaneous nerve (MDCN) corresponds to the medial branch of the superficial peroneal nerve and innervates the dorsomedial aspect of the big toe. Meanwhile, the lateral dorsal cutaneous nerve (LDCN) arises from the deep fibular nerve and innervates the dorsal-lateral aspect. These 4 nerves are of particular interest because they are vulnerable to injury during commonly used surgical approaches for hallux valgus, which may contribute to postoperative sensory complications.
This study aims to perform a systematic review of the literature to summarise the anatomical relationships and landmarks that define the course of these nerves. This is intended to reduce the risk of iatrogenic injury during hallux surgery.
Materials and Methods
Search Protocol
This systematic review was conducted in accordance with the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines and was registered in the PROSPERO international database under the reference number CRD420251082299.13,14 We included all studies that describe the anatomical relationships of the hallux sensory nerves as well as techniques for identifying them, from the tarsometatarsal joint (C1M1) to the interphalangeal joint. Studies published in English or French with an available online abstract were included. Studies were excluded if they were case reports, focused solely on anaesthetic techniques for HV surgery, reported iatrogenic nerve injuries without anatomical description, did not address hallux innervation, or concerned pathologies other than HV.
Database Search
A systematic review of articles published up to February 2025 was conducted using the PubMed, Embase, and Cochrane databases. The keywords ‘nerve anatomy’, ‘hallux valgus’ and ‘bunion’ were used individually or in combination.
Study Selection
Two independent authors (P.C. and G.R.) screened the articles. An initial selection was performed based on titles and abstracts. The selected articles were then thoroughly reviewed and included or excluded according to the predefined inclusion and exclusion criteria. The authors also examined the reference lists of the selected articles to identify any additional relevant information. Where an article was selected by one author but not the other, a consensus was reached by all authors on its inclusion in the study.
Data Extraction
Two independent authors performed data extraction from the selected articles. The extracted information included the number of subjects, anatomical relationships (in relation to adjacent structures such as joints, tendons, and vessels), the surgical technique when applicable, and the level of evidence for each study. In accordance with Cochrane recommendations, all authors independently assessed the methodology of each included study, taking potential confounding factors into account, following the PRISMA guidelines.13,14 Because of the heterogeneity of the included anatomical, imaging, and clinical studies, the findings were synthesised descriptively, as direct quantitative comparison across study designs was not possible.
Results
Study Selection
The literature search identified 863 articles. After applying the selection criteria, 13 articles were included in the systematic review (Figure 1).15 -26 The main findings of these studies are summarized in Table 1.

PRISMA 2020 flow diagram of study selection. Database searches (PubMed, Embase, and Cochrane) identified 863 records. After removal of duplicates (n = 286), 595 records were screened and 282 were excluded. Full texts were assessed for 301 reports, and 13 studies were included in the systematic review, including 1 additional study identified through reference screening. Reports of included studies (n = 0) indicate that no additional secondary reports of the included studies were identified.
Characteristics and Scope of Included Studies on Sensory Nerve Anatomy Relevant to Hallux Valgus Surgery.
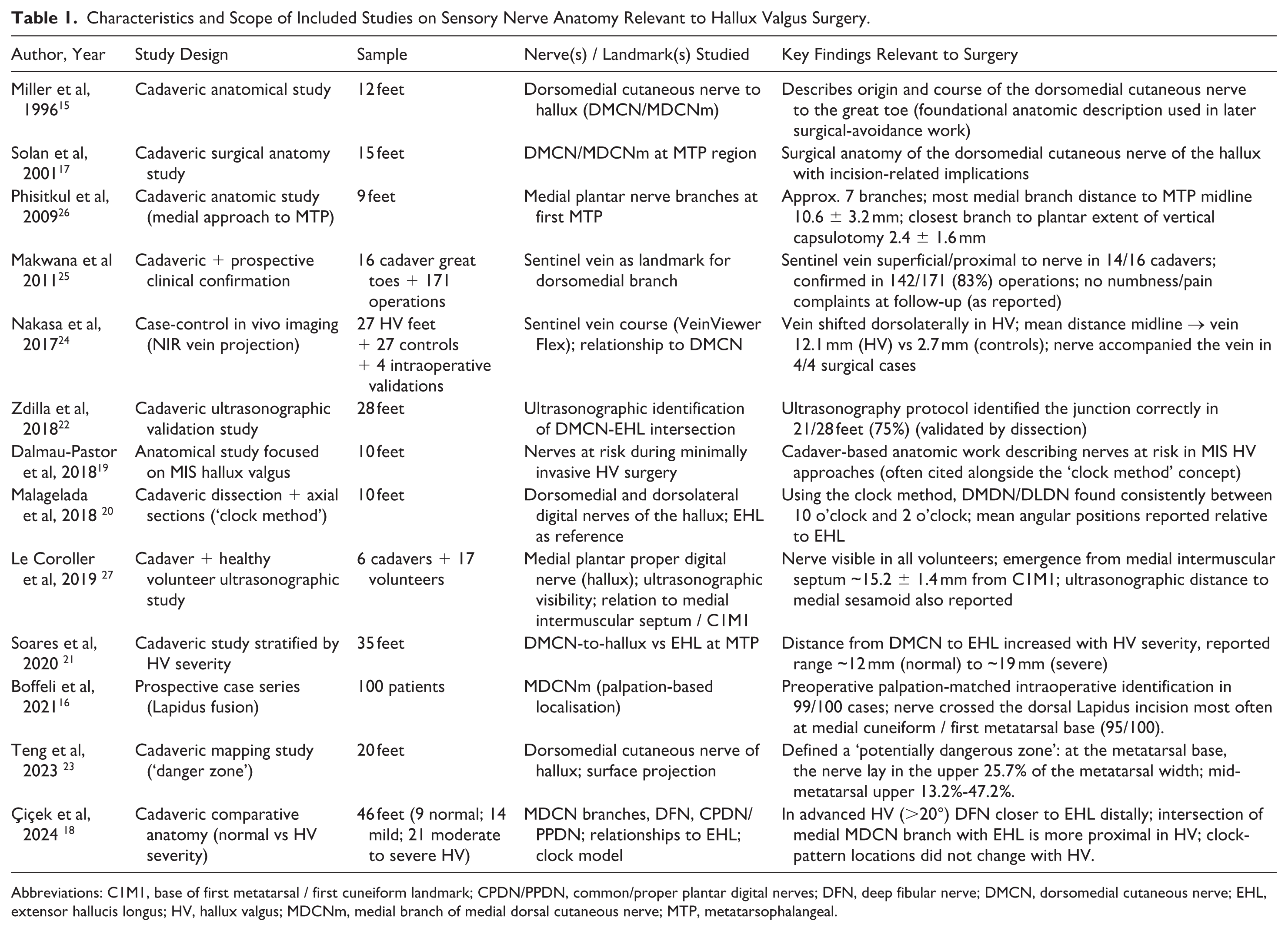
Abbreviations: C1M1, base of first metatarsal / first cuneiform landmark; CPDN/PPDN, common/proper plantar digital nerves; DFN, deep fibular nerve; DMCN, dorsomedial cutaneous nerve; EHL, extensor hallucis longus; HV, hallux valgus; MDCNm, medial branch of medial dorsal cutaneous nerve; MTP, metatarsophalangeal.
Medial Dorsal Cutaneous Nerve
Relationship with the extensor hallucis longus tendon
From the tarsometatarsal joint (C1M1)
The origin of the medial dorsal cutaneous nerve (MDCN) has been reported at an average of 40 mm (range: 8-61 mm) proximal to the base of first metatarsal / first cuneiform landmark (C1M1), with a diameter ranging from 1 to 3 mm (Table 2). 15 In 95.6% of cases, the nerve divides into two branches: a medial branch (MDCNm), continuing towards the hallux, and a lateral branch (MDCNl), supplying the lateral toes. This bifurcation occurs proximal to the joint in 69.6% of cases and distal to the joint in 26% of cases. 15 During dorsal Lapidus procedures, the MDCNm frequently crosses the dorsal incision, intersecting the medial cuneiform in 95% of cases. 16 The crossing between the MDCNm and the extensor hallucis longus tendon (EHL) is consistent: Solan et al 17 reported it at an average of 7.8 mm (range: 0-16 mm) proximal to C1M1, whereas Miller et al 15 described a broader crossing zone, beginning at 32 mm (range: 8-50 mm) and ending at 16 mm (range: 0-41 mm).
Anatomical Landmarks and Quantitative Relationships of Nerves at Risk During Hallux Valgus Surgery. a
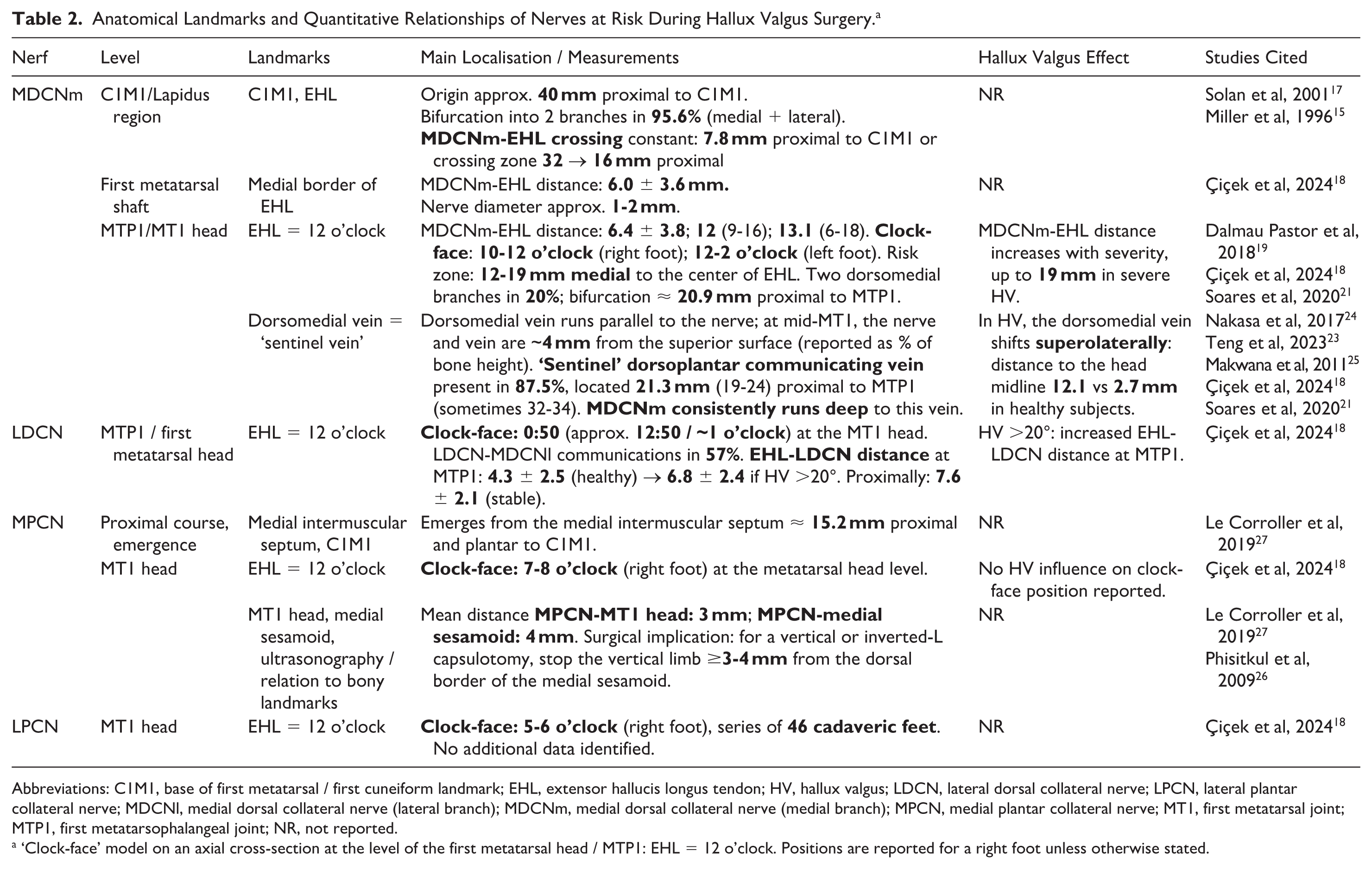
Abbreviations: C1M1, base of first metatarsal / first cuneiform landmark; EHL, extensor hallucis longus tendon; HV, hallux valgus; LDCN, lateral dorsal collateral nerve; LPCN, lateral plantar collateral nerve; MDCNl, medial dorsal collateral nerve (lateral branch); MDCNm, medial dorsal collateral nerve (medial branch); MPCN, medial plantar collateral nerve; MT1, first metatarsal joint; MTP1, first metatarsophalangeal joint; NR, not reported.
‘Clock-face’ model on an axial cross-section at the level of the first metatarsal head / MTP1: EHL = 12 o’clock. Positions are reported for a right foot unless otherwise stated.
From the first metatarsal and the first metatarsophalangeal joint
At the midshaft of the first metatarsal, the distance between the medial branch of the MDCNm and the medial border of the EHL tendon has been reported as 6.0 ± 3.6 mm and 11 mm (range: 6-15 mm), respectively, with an estimated nerve diameter of between 1 and 2 mm. 18 At the first metatarsophalangeal (MTP1), the average MDCNm-EHL distance varies: 6.4 ± 3.8 mm, 12 mm (range: 9-16 mm), and 13.1 mm (range: 6-18 mm).15,17 To simplify the description of nerve trajectories around the head of the first metatarsal, Dalmau-Pastor et al 19 proposed using a transverse section combined with a clock-face reference system. The EHL is positioned at 12 o’clock, and the MDCNm is positioned between 10 and 12 o’clock for a right foot and 12 and 2 o’clock for a left foot. 20 These findings were confirmed by Çiçek et al, 18 who found no sex-based differences. Soares et al 21 recommend considering an expanded danger zone, ranging from 12 to 19 mm medial to the EHL centre. In 20% of cases, the MDCNm divides into 2 dorsomedial branches, with an average bifurcation point 20.9 mm proximal to the MTP1 joint. A constant distal (medial) branch, similar in caliber to the main trunk in 80% specimens, was identified and followed a plantar and distal course without crossing the plantar plane of the metatarsal head. 17
Percutaneous and ultrasonography-guided localization techniques
Palpation during resisted hallux extension has been described as a simple clinical manoeuvre for localising the MDCNm in the medial column/C1M1 region. The cited study reported a 100% sensitivity and a 99% positive predictive value (PPV) for this manoeuvre. 16 Ultrasonography performed by an inexperienced operator on 28 cadaveric feet identified the MDCNm-EHL intersection with 75% sensitivity, and 100% PPV. 22 These findings suggest that both techniques can be used to confirm nerve location, but that ultrasonography may miss some nerves and should therefore be interpreted with caution.
Sentinel vein and nerve-vein relationships
Nakasa et al 24 and Teng et al 23 identified the dorsomedial vein of the hallux as a landmark. This vein runs parallel to the medial branch of the medial dorsal cutaneous nerve (MDCNm). At the C1M1 joint, the vein is located 13.8 mm from the superior aspect of the joint, and ranges from 23.5% to 71.9% of the joint’s height. At the midshaft of the first metatarsal, the nerve lies between 13.2% and 47.2% of the metatarsal height, and the vein between 4.1% and 52.7%. On average, both structures were located approximately 4 mm from the superior aspect of the metatarsal. 23 The nerve follows the same direction as the dorsomedial vein and is positioned slightly superiorly in the proximal portion of the metatarsal. Eventually, it crosses the vein. In addition, Makwana described a communicating dorsoplantar ‘sentinel’ vein, which was found in 87.5% (14/16) of dissections. 25 This vein was located 21.3 mm (range: 19-24 mm) proximal to the MTP1 joint, and was found to be located more proximally in 12.5% of cases (32-34 mm). 25 This vein is oriented transversely across the first metatarsal and connects the dorsal arch to the lateral plantar network. The MDCNm consistently crossed deep to this ‘sentinel’ vein. In a prospective clinical series of 171 operations, the sentinel vein was confirmed intraoperatively in 142 cases (83%), supporting its utility as a surgical landmark. 25
Influence of hallux valgus
Çiçek et al 18 did not observe any radial variation in position when using the clock-face model (approximately 11:15), but they did report a more proximal crossing with the EHL in cases of moderate or severe HV. In cases of HV, the dorsomedial vein shifts superolaterally at the MTP1 joint level, with an average distance of 12.1 mm from the midline of the metatarsal head, compared with 2.7 mm in healthy subjects (Figure 2). 24 Soares et al 21 confirmed a progressive and substantial increase in the MDCNm-EHL distance according to the severity of the deformity, reaching up to 19 mm in severe HV.

Diagram of the anatomical relationships reported in the literature (right foot).
Lateral dorsal cutaneous nerve
Çiçek et al 18 positioned the LDCN at 0:50 on the clock-face model at the level of the first metatarsal head (for a right foot) (Table 2). Communications between the LDCN and the lateral branch of the medial dorsal cutaneous nerve (MDCNl) were observed in 57% of cases. When HV was greater than 20°, the EHL-LDCN distance at the MTP1 joint increased from 4.3 ± 2.5 mm to 6.8 ± 2.4 mm. Proximally, the distance remained stable at 7.6 ± 2.1 mm. 18
Medial plantar collateral nerve
The MPCN was identified in relation to the medial intermuscular septum, approximately 15.2 mm proximal and plantar to C1M1 (Table 2). 26 On the clock-face model, it is located between 7 and 8 o’clock, at the level of the metatarsal head (for a right foot), with no influence from HV. 18 Using ultrasonography, Le Corroller et al 27 measured an average distance of 3 mm between the MPCN and the first metatarsal head, and 4 mm between the MPCN and the medial sesamoid. These findings support Phisitkul et al’s 26 recommendation that during a vertical or inverted-L capsulotomy of the MTP1 joint, the vertical branch should stop at least 3-4 mm from the dorsal edge of the medial sesamoid.
Lateral plantar collateral nerve
Çiçek et al 18 reported the LPCN in their series of 46 cadaveric feet, positioning it at the level of the metatarsal head between 5 and 6 o’clock (for a right foot) (Table 2). No additional anatomical data on the LPCN was identified.
Discussion
The main finding of this study is that no single anatomical or radiological landmark is fully reliable for identifying the sensory nerves at risk during hallux surgery. However, combining several criteria or defining safety zones could improve identification of the nerves most at risk of iatrogenic injury.
At the C1M1 joint level, Boffeli et al’s 16 method of palpating the MDCN has been suggested as a simple and low-cost method of nerve localisation. Nevertheless, this technique requires active patient participation, making it impractical intraoperatively, and only allows nerve identification at a single point. Furthermore, the authors did not report any objective measurements, and the reproducibility of this approach across different patient morphologies, particularly in overweight or previously operated patients, remains uncertain. Using ultrasonography, Zdilla et al 22 achieved a sensitivity of 75% for MDCN identification at the same level. However, this technique requires a high-performance ultrasonography machine and appropriate training.
At the MTP level, approaches based on the predefined safety quadrants described by Dalmau-Pastor et al 19 or the danger zone proposed by Teng show promise.20,23 However, these concepts were developed from studies on healthy cadaveric feet, which limits their generalisability to pathological conditions. Similarly, while the ‘sentinel vein’ concept is anatomically appealing, it should be interpreted with caution, as these veins are closely related to the EHL, the course and tension of which are altered in HV deformity. Furthermore, although the sentinel veins described by Makwana et al 25 and Nakasa et al 24 are well characterized anatomically, they lack precise, practical landmarks for surgical osteotomy. Data regarding the LDCN, the LPCN, and the MPCN remain limited in the literature.
In clinical practice, several authors have investigated the risk of nerve injury during HV correction. For tarsometatarsal procedures, Barg et al 28 reported an overall rate of 5% for sensory disturbances in a meta-analysis, without specifying the affected nerve. The MDCN appears to be the structure at greatest risk. Comparable complication rates have been reported for dorsal and plantar approaches using plate fixation. Cadaveric studies have demonstrated the proximity between hardware and the MDCN in percutaneous fixation; So et al 29 recommended positioning the screw at least 18 mm distal to the second tarsometatarsal joint in modified Lapidus procedures.
Numerous studies have analysed the incidence of neurological injury in metatarsophalangeal surgery, comparing open and minimally invasive techniques. The reported frequency of postoperative paresthesia ranges from 0% to 45% following distal correction using open approaches and from 2.4% to 15% after percutaneous procedures. 30 In a meta-analysis of 1088 patients who underwent percutaneous correction, Gonzalez et al 31 observed an overall rate of 2.2% neurological complications. During percutaneous intra-articular chevron osteotomy, the MDCN is considered to be at the highest risk, particularly during medial eminence resection. 32 In a cadaveric study, Malagelada et al 20 proposed that using the ‘clock-face’ reference method could reduce the risk of nerve injury during osteotomy. In double minimally invasive chevron and Akin procedures, no increased risk of MDCN injury has been observed.33,34 Kaipel et al compared the rates of iatrogenic nerve injury between experienced and novice surgeons performing Bosch osteotomies on cadaveric specimens and found that the MDCN was injured in 30% of cases by the junior surgeon compared with only 5% by the senior surgeon. 35 This emphasises the critical role of experience and training in mastering minimally invasive techniques.
During lateral release procedures, the LPCN and LDCN are the nerves primarily at risk. Anatomical studies have shown a low rate of nerve injury, with no substantial difference between open and percutaneous approaches, or between transarticular and medial approaches involving dissection, or intermetatarsal ligament sacrifice. 36 -38 The extent of release also appears to influence risk: ranging from minimal (adductor tendon only) to extensive (adductor tendon, suspensory ligament, sesamoid-phalangeal ligament, lateral head of the flexor hallucis brevis, and deep transverse metatarsal ligament). 39 In a prospective study of 86 patients, Lee et al compared distal chevron osteotomy with and without lateral release, reporting postoperative neuritis of the LPCN or LDCN in 33% of patients undergoing the release. 40 Although most cadaveric studies report no direct nerve injury, clinical findings suggest an increased incidence of postoperative discomfort within the first web space following lateral release.
It is important to recognise that nerve injury is a multifactorial process, and distinguishing between pre-existing neurological symptoms and those resulting from surgical trauma can be challenging. Herron et al recommended the use of systematic preoperative sensory testing with Semmes-Weinstein monofilaments, as they found that 65% of patients demonstrated measurable sensory reduction, despite only 21% being symptomatic. 41 Jastifer et al reported similar findings in a cohort of 54 patients, noting that surgery substantially improved neurological symptoms, and reduced the hypoesthetic area by a factor of 4.3. 7 To minimise medicolegal risk, all preoperative neurological deficits should be carefully documented, and patients should be informed about the potential for iatrogenic nerve injury. 2
This study has several limitations. Most of the anatomical landmarks and reference points described in the literature were derived from healthy cadaveric specimens, whereas HV deformity alters the local anatomy and the course of nerves. Further research is needed to validate these reference points in relation to different deformity patterns, such as pronation angle, first-ray instability, and flatfoot. Furthermore, these identification techniques have rarely been tested in clinical settings, although combining them with adequate surgical experience likely reduces iatrogenic risk. Finally, data regarding the LDCN, LPCN, and MPCN remain scarce, representing an area for future investigation. Future clinical studies involving patients with hallux valgus should evaluate whether the systematic use of these anatomical landmarks, combined with a preoperative sensory assessment and careful surgical technique, can minimise the risk of postoperative sensory nerve injury.
Conclusion
The risk of iatrogenic nerve injury may be reduced using simple and low-cost techniques. For the MDCNm, palpation combined with ultrasonography and sentinel vein mapping may help localize the nerve. Surgeons should familiarize themselves with the locations of the 4 nerves on an axial section distal to the first metatarsal and adapt their incisions accordingly. However, these measurements have most often been performed on healthy subjects, whereas HV deformity alters the anatomical relationships. Therefore, junior surgeons should be encouraged to refine their technique using anatomical specimens before performing the procedure on patients.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114261451225 – Supplemental material for Sensory Nerves at Risk During Hallux Valgus Surgery: Anatomical Insights and Preventive Strategies—A Systematic Review
Supplemental material, sj-pdf-1-fao-10.1177_24730114261451225 for Sensory Nerves at Risk During Hallux Valgus Surgery: Anatomical Insights and Preventive Strategies—A Systematic Review by Paul Chanzy, Agathe Yvinou, Hugues Pascal-Moussellard, Laura Marie-Hardy and Grégoire Rougereau in Foot & Ankle Orthopaedics
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Disclosure forms for all authors are available online.
Data Availability Statement
All articles cited in this study are publicly available through searches of the PubMed, Embase, and Cochrane databases.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.