
Abstract
Background:
Disparities in health care continue to affect marginalized populations in the United States, contributing to increased morbidity, mortality, and health care costs. Although disparities have been extensively studied in arthroplasty and spine surgery, there is limited understanding of how they manifest in orthopaedic trauma, where treatment is often emergent. Therefore, to explore associations between patient demographics and orthopaedic trauma care beyond the emergent timeframe, this study investigated timing to care in patients that required acute external fixation followed by staged definitive fixation.
Methods:
A retrospective review of trauma patients who underwent lower extremity external fixation at a level 1 trauma center from January 2014 to March 2024 was conducted. Data collected included patient sex, race, age, insurance, comorbidities, fracture type (open vs closed), and substance use. Key outcomes were days from admission to external fixation and from external fixation to open reduction internal fixation (ORIF). Negative binomial post hoc testing was used, with significance set at P <.05.
Results:
A total of 129 patients met the inclusion criteria. There was a significant difference in timing to ORIF between genders (P = .034) but no significant difference in timing to ORIF between races (P = .093); no differences were seen in timing to external fixation. After post hoc analysis, only femur fractures showed a significant difference in timing spending 44% shorter time in external fixation (P = .03).
Conclusion:
These findings suggest that, following initial stabilization, gender may correlate with the timing of definitive fixation in orthopaedic trauma care. Identifying and addressing disparities is essential to reducing inequities in clinical outcomes and health care utilization. This study highlights the need for further research aimed at understanding and mitigating delays in treatment.
Level of Evidence:
Level III, retrospective data from single institution.
Introduction
Health care disparities in the United States contribute to increased morbidity and mortality for minority populations, yet there remains a significant gap in literature investigating disparities in orthopaedic trauma. Most research thus far has primarily focused on orthopaedic disparities in the fields of spine and arthroplasty.1,2 Although previous studies have stated that patients with an acute orthopaedic trauma are treated on an emergent basis and therefore have reduced the opportunity for bias, there is emerging evidence demonstrating the additional challenges marginalized groups face after orthopaedic trauma.1,2 Furthermore, it is known from prior research that minorities make up the largest portion of many orthopaedic traumas; therefore, understanding how to better treat those facing increased barriers is critical. 1
To test whether marginalized patients experience delayed definitive care, but not necessarily delayed acute care, this study specifically looked at patients requiring staged external fixation for their orthopaedic trauma. Briefly, staged external fixation followed by open reduction and internal fixation (ORIF) is commonly used for lower extremity fractures to confer stability and protect soft tissues. 3 However, prolonged intervals to definitive treatment can increase infection risk, potentially resulting in serious complications such as nonunion or limb amputation. 4 Meanwhile, timely definitive treatment shortens hospital stays and reduces health care costs. These staged injuries are an ideal model for investing factors contributing to delayed treatment that may be previously overlooked in trauma literature on acutely treated injuries.
Through this approach, this investigation may be able to identify marginalized groups that are prone to longer care periods. There is already growing evidence that minority patients have extended hospitalizations, are more prone to emergency department visits for an injury-related issue as opposed to clinic appointments, are less likely to use rehabilitation services, and experience worse functional recoveries.5,6 Considering the substantial health care resources and recovery time associated with external fixation for trauma patients, it is essential to investigate any disproportionate impact on racial minorities receiving this treatment.
Therefore, this study aimed to investigate the association of patient characteristics and injury type with timing to external and definitive fixation in patients with fractures of the lower extremity. It was hypothesized that marginalized patients would experience significantly longer times from external fixation to ORIF compared with male patients and patients of other races, but there would be no significant differences between sexes or races in time from admission to external fixation.
Methods
This was a retrospective review of data collected from a single-institution level 1 trauma center patient registry. Inclusion criteria for this study were trauma activation patients requiring lower extremity external fixation between January 1, 2014, and March 31, 2024. International Classification of Diseases (ICD) procedure codes for lower extremity external fixation were used to identify patients in the Trauma Registry. Inclusion criteria were (1) trauma activations and (2) age >16 years; patients were excluded if they remained in external fixation for >60 days (as these patients were either in external fixation devices because of severely unstable knee dislocations or patient refusal for removal) or died before discharge. Patient sex, race, age, date of birth, insurance, and Injury Severity Score were collected from the database. Clinical data including whether the fracture was open or closed, type of fracture, patient smoking, drug, and alcohol use, and patient comorbidities (chronic obstructive pulmonary disease, renal failure, congestive heart failure, cirrhosis, diabetes, peripheral artery disease) were collected from the electronic medical record. Patients who were missing any of the aforementioned information were excluded. The date of external fixation and ORIF were recorded. Because of very small numbers of most race categories other than Black or African American and White (with others representing <15% of the total patients), the analysis was restricted to Black or African American and White patients.
Statistical Analysis
To test the prediction that marginalized groups experience longer time until definitive care, but not longer time until acute care, analyses of variance were used to compare days from admission to external fixation and days from external fixation to ORIF among genders and among races. Data were stratified with gender and race by extremity; therefore, the arithmetic mean and median number of days for each gender and race by each extremity were reported.
To identify variables that affect delays in definitive care, a Poisson model fitted to data was created representing days in external fixation to ORIF, as a function of the following independent variables: age; insurance status, categorized as government or commercial; tobacco, drug, and/or alcohol-use, categorized as no or yes; histories of chronic obstructive pulmonary disease, renal failure, cirrhosis, congestive heart failure, and diabetes, categorized as no or yes; injury severity score; Glasgow Coma Scale, categorized as <15 or 15; and the 2-way interactions between gender and fracture type (categorized as closed or open); race and fracture type; gender and extremity; race and extremity; and gender and race.
Overdispersion was tested for with a Pearson dispersion value of 4.39 indicating substantial overdispersion. Therefore, a negative binomial post hoc analysis was performed to test for variables associated with longer times to ORIF. A reduced model comparing race, gender, extremity and open fractures was used comprising the following independent variables: age, tobacco use, drug use, alcohol use, cirrhosis, congestive heart failure, and diabetes chronic obstructive pulmonary disease, renal failure, cirrhosis; in addition, the 2-way interactions between gender and extremity, race and extremity, and race and fracture type (open vs closed) were tested (Supplementary Table 2). Insurance was not included in the reduced model as it was colinear with race (Supplementary Table 3). Results are reported as Confiende Intervals (CIs), calculated with Wald intervals in line with negative binomial analysis where the estimate is ±1.96 × SE on a log scale, then exponentiated. Exponentiated estimates are incidence rate ratios (IRRs), where an IRR >1 is a predicator associated with more days to ORIF, and <1 is a predictor associated with fewer days to ORIF.
The significance of hypothesis tests with 5% alpha was conducted. The reduced model parameter estimates and conditional post hoc pairwise comparisons on the geometric mean and rate ratio scale and visualized model predictions were reported. All analyses were conducted in the R statistical computing environment (R Core Team 2021). 7 R code and a comprehensive list of software, package, and dependency versions needed to reproduce this analysis is available in the project repository: https://github.com/seanmlee/Delayed_Definitive_Fixation and https://github.com/rstationpro/omara_ortho. Deidentified data needed to reproduce this analysis is available on request.
Results
A total of 129 patients met the inclusion criteria and had complete information for all variables of interest. The average age of patients was 43.5 ± 16.7 (SD) years, and 42.6% were female (n = 55). Most patients had government insurance (56.6%, n = 73). Nearly one-third (29.5%) of all injuries were open. The most common fracture location was tibia (46.5%), followed by ankle/pilon (28.7%), then by femur (24.8%). Further patient data can be seen in Table 1; excluded data can be seen in Supplementary Table 1.
Patient Characteristics and Outcomes. a
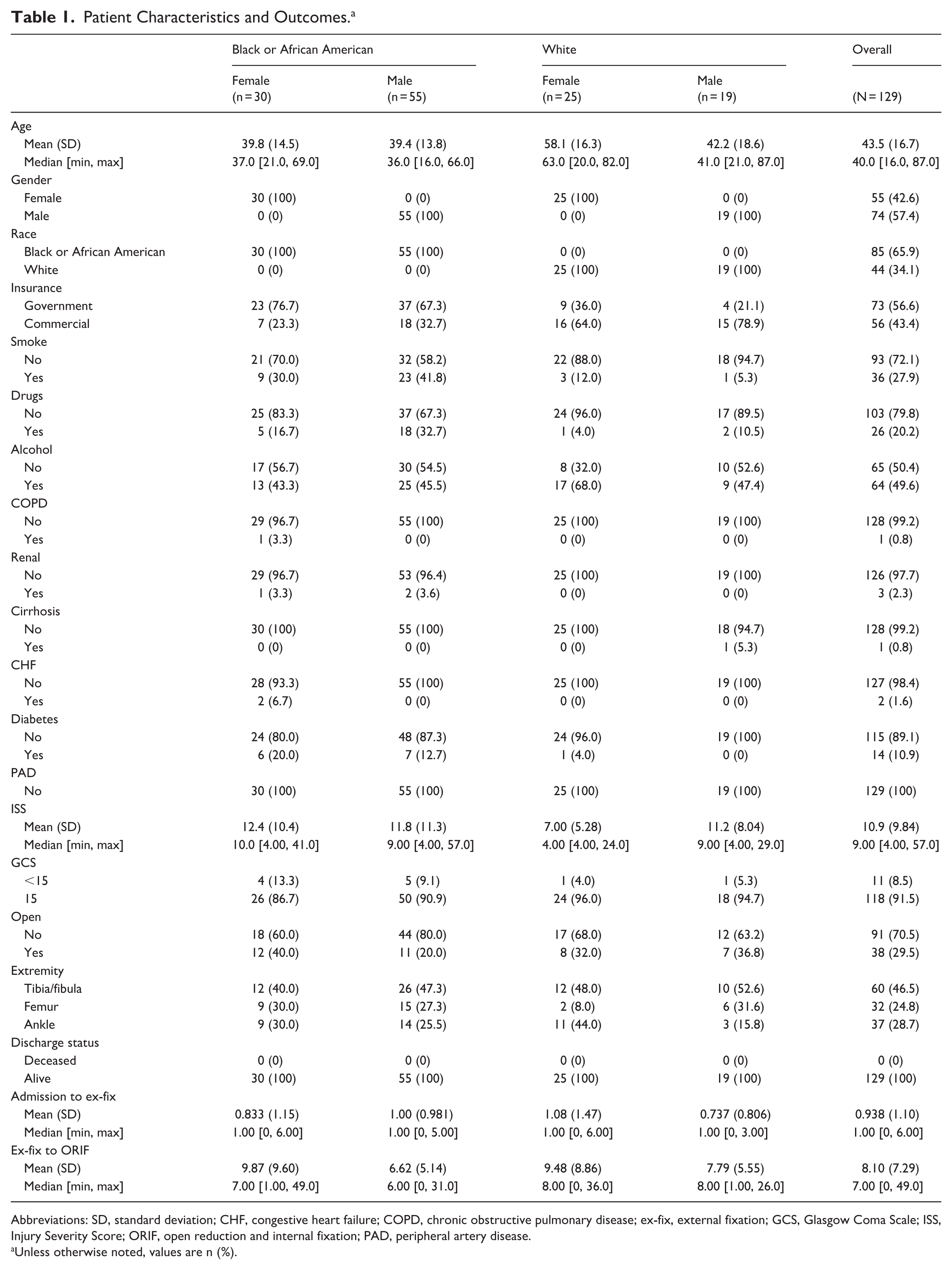
Abbreviations: SD, standard deviation; CHF, congestive heart failure; COPD, chronic obstructive pulmonary disease; ex-fix, external fixation; GCS, Glasgow Coma Scale; ISS, Injury Severity Score; ORIF, open reduction and internal fixation; PAD, peripheral artery disease.
Unless otherwise noted, values are n (%).
When comparing the duration of time to definitive and acute care between genders using analyses of variance, significant differences in external fixation to ORIF (P = .034) but not admission to external fixation (P = .611) (Table 2) were found. When comparing the durations of definitive and acute care between races using analyses of variance, no significant differences in external fixation to ORIF (P = .093) or admission to external fixation (P = .328) were found (Table 3).
Outcomes Stratified by Extremity and Gender.

Abbreviations: SD, standard deviation; ex-fix, external fixation; ORIF, open reduction and internal fixation.
P < .05.
Outcomes Stratified by Extremity and Race.
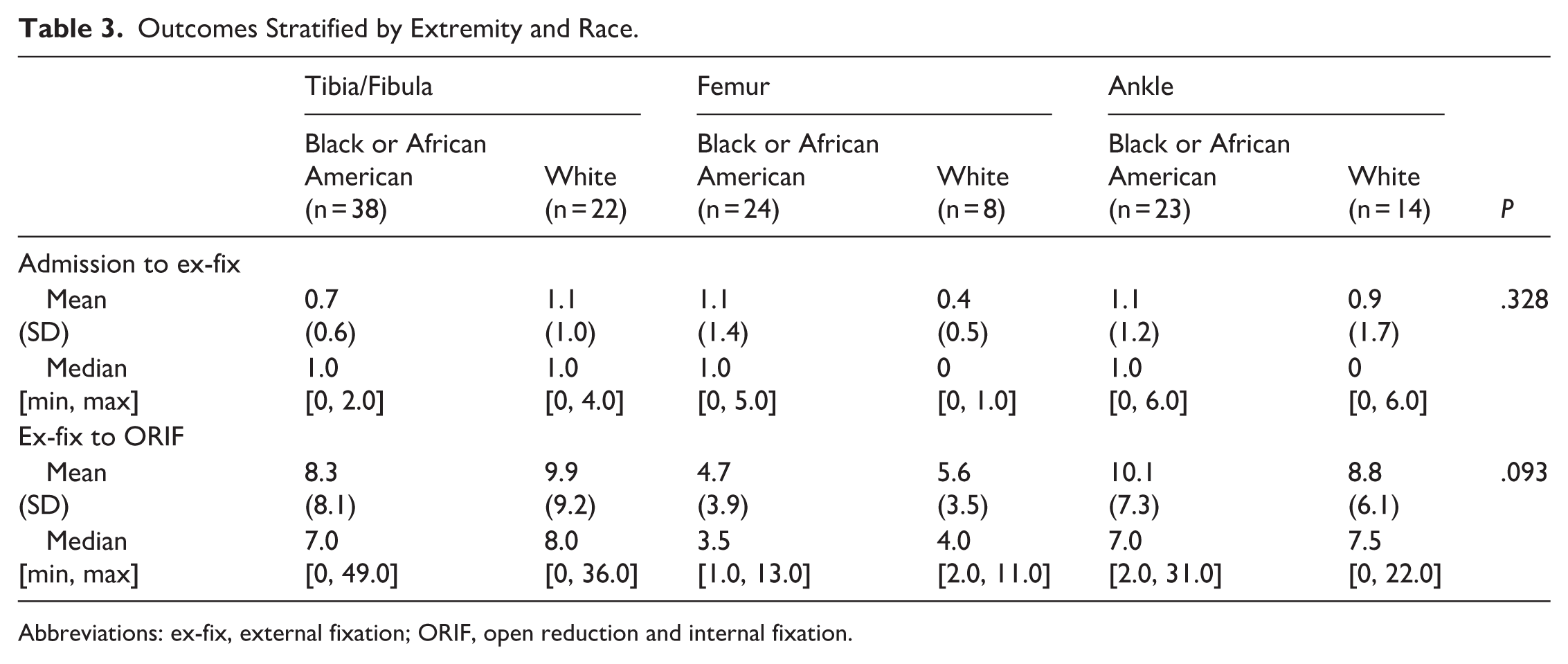
Abbreviations: ex-fix, external fixation; ORIF, open reduction and internal fixation.
Using a negative binomial post hoc analysis, it was found that patients with femur fractures spent 44% less time to ORIF than tibia fractures (IRR: 0.66, 95% CI 0.45-0.96, P = .03), there were no differences between males vs females (IRR: 0.83, 95% CI 0.63-1.08, P = .16), or race with White vs Black or African American patients (IRR 1.11, 95% CI 0.81-1.52, P = .516) (Table 4, Figure 1).
Post Hoc Pairwise Comparisons From the Fitted Negative Binomial Model for Days in Ex-Fix to ORIF. a
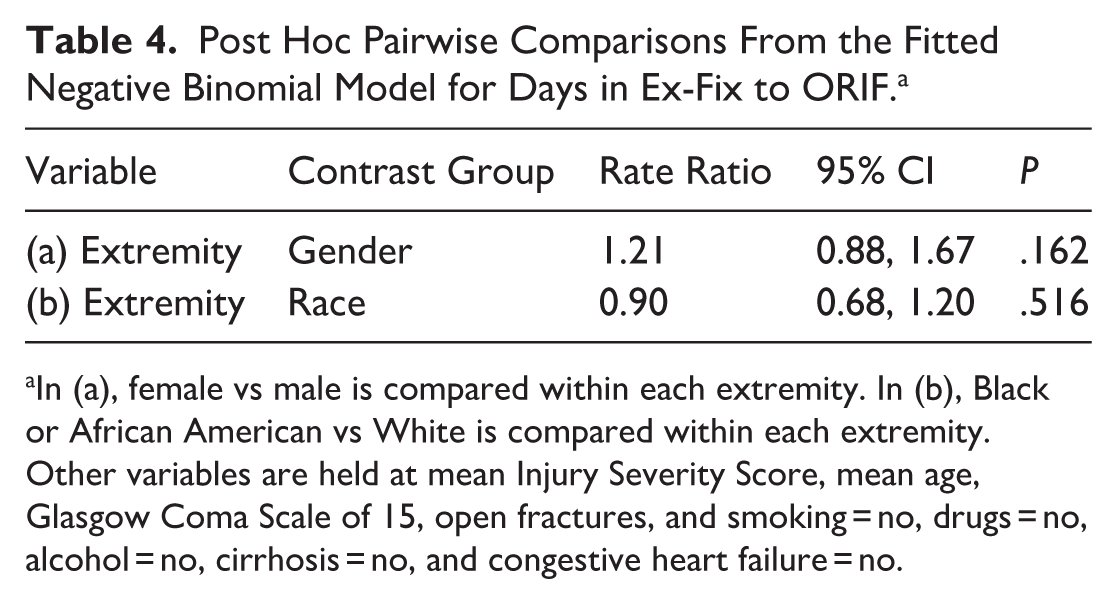
In (a), female vs male is compared within each extremity. In (b), Black or African American vs White is compared within each extremity. Other variables are held at mean Injury Severity Score, mean age, Glasgow Coma Scale of 15, open fractures, and smoking = no, drugs = no, alcohol = no, cirrhosis = no, and congestive heart failure = no.

Estimated ex-fix to ORIF in days (open circles) and 95% CIs (error bars) from negative binomial model as a function of age, smoking status, alcohol use, history of cirrhosis, DM, and the 2-way interactions between race and fracture type (open or closed), race and extremity, and gender and extremity. In (A), differences are seen between females and males based off fractured extremity. In (B), comparisons are between races by fractured extremity. P values from post hoc pairwise comparisons are reported above brackets. Colored circles represent actual data. ex-fix, external fixation; ORIF, open reduction and internal fixation.
Discussion
Although no differences were observed between sexes and racial groups in time from admission to external fixation, this study found that female patients experienced significantly longer times in external fixation waiting for ORIF compared with males. However, no differences were found between genders after post hoc analysis, possibly because of the limited data points available for analysis. In addition, post hoc analysis revealed that femur fractures were often fixed sooner than other extremities. These findings should be looked at in concert with prior literature on disparities in timing to care, which highlight the intricate ways in which intersecting factors—such as sex, race, and fracture type—can exacerbate inequities.
This study found that female patients experience longer delays to definitive care for lower-extremity trauma. This is consistent with a retrospective study that included 9406 patients from 650 trauma centers in the United States, where females were more likely to undergo fixation later than hospital day 2 than men with open femoral fractures. 8 Similarly, Gohel et al 9 observed that a significantly higher portion of females were likely to experience a surgical delay of >24 hours for a femoral shaft fracture requiring fixation. Although these studies identified significant sex-based differences, they did not quantify the duration of delay. This research shows that females spend at times 58% longer in external fixation, which underscores a potential disparity in when females receive care in the hospital. This quantified delay represents a critical first step toward identifying what specific factors contribute to inequities in care for female patients.
As opposed to previous literature, this study did not show any significant differences in timing to definitive fixation based off of race.10-12 A study by Chung et al 13 involving 85924 Medicare patients with distal radius fractures revealed a significant racial disparity in surgical intervention, demonstrating that Black patients were less likely to undergo ORIF than White patients (OR = 0.74, 95% CI 0.65-0.85). Although the authors proposed that differences in osteoporosis prevalence might contribute to this finding, the substantial discrepancy in surgical treatment rates suggests that other factors may be at play. Moreover, it is crucial to acknowledge that existing inequities in bone mineral density testing among Black patients may confound the interpretation of osteoporosis prevalence data in this population.14,15 Other studies, such as work by Driesman and colleagues, found that minority patients with tibial plateau fractures often had longer hospitalizations than White patients (P < .001) with an overall increase in hospital costs of $4000. 5 The presented results may show progress in orthopaedic trauma care that goes past the time of initial external fixation; however, continued focus needs to be on ensuring equal treatment for all races in terms of wait times to address any modifiable health care disparities.
Although causality of these observed differences cannot definitively be established, several strategies have been proposed to confront these disparities. Increasing physician diversity in the workforce is one way, as studies demonstrate that patients value cultural competence and clear communication with their providers. 16 Further studies have shown that expanding educational programs to include race-conscious learning may help address biases. 17 On a larger scale, disparities appear to be compounded by interhospital variability in care quality, suggesting that targeted resource allocation to underperforming facilities may be beneficial. 18 Additional resource constraints, such as bed availability or surgeon staffing, which were not examined in this study, may also contribute to delays in care. 19
One limitation to our study was we did not include insurance status because it was collinear with race in this data set. This pattern raises the possibility that insurance type may play an indirect role in which surgeon ultimately assumes responsibility for definitive care. A hypothesis to explore would be to determine if surgeons consider insurance status when anticipating patients’ ability to access postoperative care. One study by Rogers and colleagues showed that although 96% of clinics within a metropolitan area accepted Medicaid insurance for postoperative anterior cruciate ligament reconstruction patients, only 52% accepted Medicaid. 20 Furthermore, Schairer et al 21 found that White patients with private insurance were more likely to receive operative fixation of clavicle fractures, and female sex, non-White race, and public or self-pay insurance are independently associated with lower rates of meniscus surgery. These observed disparities linked to race and insurance status may reflect broader challenges within the health care system that further disadvantage vulnerable populations. Systemic barriers such as limited access to follow-up care, complex authorization processes, and challenges with discharge planning may contribute to delays in definitive fixation for patients with government insurance. Additionally, concerns regarding access to rehabilitation resources may influence clinical decision making and surgical timing. These issues, compounded by potential implicit bias, may contribute to disparities in timing to definitive fixation, which has the potential to impact clinical outcomes and reinforce cycles of health injustice. 22
We also identified in post hoc analysis that femur fractures were fixed sooner than fractures of the tibia or ankle, likely because of the more vulnerable soft tissue envelope. 23 This anatomical difference often necessitates delaying definitive fixation to allow adequate soft tissue healing. Whether patients’ anatomy, skin color, or body type play a role in this decision in concert with other factors should be explored to understand how to aid in timely surgical management among vulnerable patient populations.
Although this study demonstrated differences among groups, it did not investigate how longer duration of immobilization in external fixation impacts patient outcomes. Many studies in the field of orthopaedic trauma have focused on the ideal timing of definitive fixation, especially for ankle and pilon fractures, recommending delayed treatment until there is evidence of soft tissue wrinkling and decreased swelling. Conversely, Hawkins et al 24 reported on the significant association between longer time to definitive ankle fixation and worse patient-reported outcomes; however, this study was limited to ankle fractures that did not require external fixation. Understanding outcomes in patients who experience longer times in external fixation is an essential part of future research.
Major limitations to this research are due to the small cohort of patients studied. This created a dataset that had moderate enough overdispersion requiring negative binomial modeling. This modeling, although appropriate for this data set, could be improved by having a larger group of patients to study. Furthermore, our data set lacks patient outcomes, limiting any conclusions that can be made about the effects a longer time in external fixation may have on healing, pain, or function outcomes. Further research focusing on patient follow-up and patient-reported outcomes will further elucidate complexities associated with race and the timing of definitive fixation. Additional limitations are due to the inherent nature of using database research, which relies on accurate coding. There are many patient factors that were not recorded that could possibly contribute to the differences seen in our study; however, we tried to limit these by conducting multivariate models. Furthermore, it relies on with ICD terminology, which is often underutilized compared with CPT codes for procedures. This likely reduced the number of eligible patients in our review. We did have to exclude patients in our review because of missing data for categories collected as well as those who remained in external fixation for longer than 60 days. Although more men were in the excluded group, all other categories remained equal between those who were included and excluded (except for days until definitive fixation, which is expected to be different given the exclusion criteria of >60 days). Lastly, limitations of generalizability are a result of these data coming from a single institution.
Conclusions
In conclusion, this study showed that sex and fracture type are associated with timing to definitive fixation for lower extremity trauma; however, results are limited because of the relatively small cohort studied. Although the reasons underlying these delays remain unclear and other etiologies could not be explored, the observed disparities suggest that certain patient populations may be at risk for prolonged hospital stays, which may contribute to higher health care costs and worse overall outcomes. These findings underscore the need for further research to determine the drivers of disparities, whether they are biological, social, or institutional, and to develop strategies that promote timely, equitable care for all trauma patients.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114261450079 – Supplemental material for Examining Delays in Definitive Fixation: An Association of Patient Demographics in Orthopaedic Trauma Requiring External Fixation
Supplemental material, sj-pdf-1-fao-10.1177_24730114261450079 for Examining Delays in Definitive Fixation: An Association of Patient Demographics in Orthopaedic Trauma Requiring External Fixation by Alana O’Mara, Emily Teehan, Andrew W. Fealy, Sean M. Lee, Rongzhe Zhao and James DeBritz in Foot & Ankle Orthopaedics
Footnotes
Appendix
Insurance Type by Race.

| Government n(%) | Commercial, n (%) | |
|---|---|---|
| Black or African American | 60 (70.5) | 25 (29.5) |
| White | 13 (29.5) | 31 (70.5) |
Ethical Considerations
Ethical approval for this study was obtained from the the George Washington University Committee on Human Research, Institutional Review Board (IRB) (ID: NCR245677).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Disclosure forms for all authors are available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.