
Abstract
Background:
Pronation of first metatarsal (M1) in hallux valgus (HV) is currently the subject of a growing body of scientific research. Several methods of manual measurements have been developed, providing heterogeneous results. Our objective was to develop automatic 3D weightbearing computed tomography (WBCT) measurements in a retrospective case-control design to compare coronal rotation of M1 head relative to the ground, M1 intrinsic torsion, and valgus deviation of M1 distal articular surface (or distal metatarsal articular angle [DMAA]) in HV and controls.
Methods:
Forty-four symptomatic HV and 44 matched controls were retrospectively enrolled, all of whom had undergone WBCT acquisition. Bone segmentation was performed (Bonelogic 2.1 software). Two methods were developed to assess position of the M1 head. One was based on automatic geometric fitting of a cylinder on the head, and the other on automatic selection of the position of the sesamoid gutters. Similarly, 2 methods were developed to assess the position of the M1 base. One was defined using principal components analysis (PCA) of the proximal articular surface of M1, and the other using the longest diagonal of the M1 base.
Results:
First metatarsal head rotation relative to the ground was, respectively, 8.9° ± 8.4° (95% CI 6.1°-11.7°) and 2.1° ± 6.4° (95% CI 0.1°-4.1°) via the cylinder method (P < .001) and 9° ± 8.3° (95% CI 6.2°-11.8°) and 0.7° ± 6.8° (95% CI −1.4° to 2.8°) via the gutters method (P < .001) in the HV and control groups. Combining the different sets of head and base measurements, the increase in M1 intrinsic torsion in HV ranged from 2° to 5°. The DMAA was 11.4° ± 6.9° (95% CI 9.3°-13.5°) in the HV group and 5.6° ± 4.7° (95% CI 4.1°-7.0°) in the control group (P < .001).
Conclusion:
Using automatic 3D WBCT measurements, we found that HV showed an increase in M1 head pronation relative to the ground of 7° to 8° greater than controls, with an increase in M1 intrinsic torsion in pronation of 2° to 5° and an increase in valgus deviation of the M1 distal articular surface of approximately 6°. Changing measurements reference points altered angular values in our study, particularly when moving from measurements based on the sesamoid gutters to gutter-independent measurements, highlighting that these methods may capture different anatomic constructs.
Level of Evidence:
Level III, case control study.
Keywords
Background
Hallux valgus (HV) pathogenesis is still unclear and involves several factors. 1 Furthermore, the outcomes of HV surgical correction are variable, with notable recurrence rates reported in several studies.2,3 First metatarsal (M1) dysplasia is considered to be a factor influencing both pathogenesis and surgical outcomes.4,5 The pronation of M1 is thought to be part of this dysplasia and is currently the subject of a growing body of scientific research.6,7
However, there are a number of controversial points on this subject. First, there is confusion between the rotation of the M1 head relative to the ground and the intrinsic torsion of M1 (from M1 base to head). M1 head rotation describes the degree of pronation or supination of the first metatarsal head axis in the coronal plane relative to a reference axis defined as the ground. Intrinsic M1 torsion, in contrast, refers to the difference in pronation or supination between the axis of the M1 base and that of the M1 head in the coronal plane. It therefore represents the rotational differential of the first metatarsal in the coronal plane from the base to the head. Assessment of M1 pronation based exclusively on coronal plane rotation of the metatarsal head does not reliably predict the magnitude of intrinsic torsion inherent to first-metatarsal morphology even though both may contribute to pronation.8,9
Second, there is no consensus on the method to be used to measure this rotation and, consequently, pronation values vary according to the different methods.10,11 Third, previously defined as a valgus deviation of the distal articular surface of M1, the distal metatarsal articular angle (DMAA) appears to be, at least in part, an artifact created by this pronation combined with 2-dimensional radiographic analysis.6,12
Nevertheless, beyond these controversies, increased pronation of the M1 head and increased valgus deviation of the distal articular surface of M1 seem to be associated with poorer surgical outcomes and increased recurrence rates in HV.4,13 -16 It therefore seems essential to define an easy and reproducible method for assessing M1 pronation. Initially, M1 head rotation were measured on conventional 2D weight-bearing radiographs, while M1 intrinsic torsion was measured by CT scan, as there was no need for a ground reference to perform this measurement.6,7,9,17 -19 To this end, several methods have been described, leading to inconsistencies in the results of studies comparing HV and controls.6,10,20,21 Valgus deviation of the distal articular surface was also measured on conventional 2D radiographs, as defined with the DMAA, but these measurements suffer from a lack of reliability.22 -24 This lack of reliability seems to be linked to M1 head pronation, which causes the lateral plantar condyle to project onto the M1 distal articular surface on dorsoplantar 2D measurements.12,24 This problem could be solved with 3D weight-bearing measurements. 12
Recently, weight-bearing cone-beam computed tomography (WBCT) has enabled 3D acquisitions of foot bones with ground references in standing position.25,26 In addition, a growing number of semi-automatic and automatic measurements have been defined to assess foot morphology, and can serve as a starting point for increasing data collection and improving the power and objectivity of scientific studies.27 -29 However, to our knowledge, no automatic WBCT measurement has been developed to assess pronation of the M1 head relative to the ground, M1 intrinsic torsion and valgus deviation of the distal articular surface of M1 in HV and controls.
Therefore, our objective was to compare coronal rotation of M1 head relative to the ground and M1 intrinsic torsion and valgus deviation of M1 distal articular surface in HV and controls using automatic 3D WBCT measurements. Our hypothesis was that HV subjects compared to controls would show increased pronation of the M1 head relative to the ground and increased M1 intrinsic torsion in pronation, but no increase in valgus deviation of the distal articular surface of M1, being considered an artifact of 2D analysis rather than a true deformity.
Methods
This retrospective case-control study received institutional review board approval (IRB 201904825) and complied with the Health Insurance Portability and Accountability Act (HIPAA).
We reviewed our database 30 and included patients who had WBCT images (PedCAT; Curvebeam) as standard care acquired for symptomatic HV between January 1, 2015, and December 31, 2021. Patient who presented prior surgery, inflammatory arthritis or neuromuscular conditions before inclusion were excluded. A group of control subjects was then selected to match the HV group in terms of age, BMI and gender. The control group was composed of subjects who were clinically evaluated for this purpose. In the absence of any foot disease (inflammatory arthritis, arthritis conditions, neuromuscular conditions) or prior surgery, subjects subsequently underwent WBCT. Forty-four feet (38 patients) were included in the HV group and 44 feet (38 subjects) in the control group (Table 1).
Demographics.
Abbreviations: BMI, body mass index; HV, hallux valgus.
Manual 2D Measurements of the M1 Head Rotation
Metatarsal Pronation Angle (MPA) and α angle are 2 previously described manual measurements of M1 head rotation relative to the ground, widely used and considered as gold standards.6,7 Therefore, 2 independent foot and ankle surgeons performed these measurements (CubeVue, Curvebeam software) in the HV group using previously published methods.6,7,19
Automatic 3D Measurements of the Hallux Valgus Angle and the Intermetatarsal Angle
All 3D measurements were performed using Bonelogic 2.1 (Helsinki, Finland) software. The longitudinal axis for each bone was defined according to a previously published method. 31 The hallux valgus angle (HVA) was defined as the angle between the longitudinal axis of the M1 and the longitudinal axis of the hallux first phalanx. The intermetatarsal angle (IMA) was defined as the angle between the longitudinal axis of M1 and the longitudinal axis of the second metatarsal (M2).
Automatic 3D Measurements of the M1 Head Rotation
To assess M1 head rotation, the axis of M1 distal end was calculated relative to the ground. The axis of the M1 distal end was calculated using 2 methods.
Cylinder method
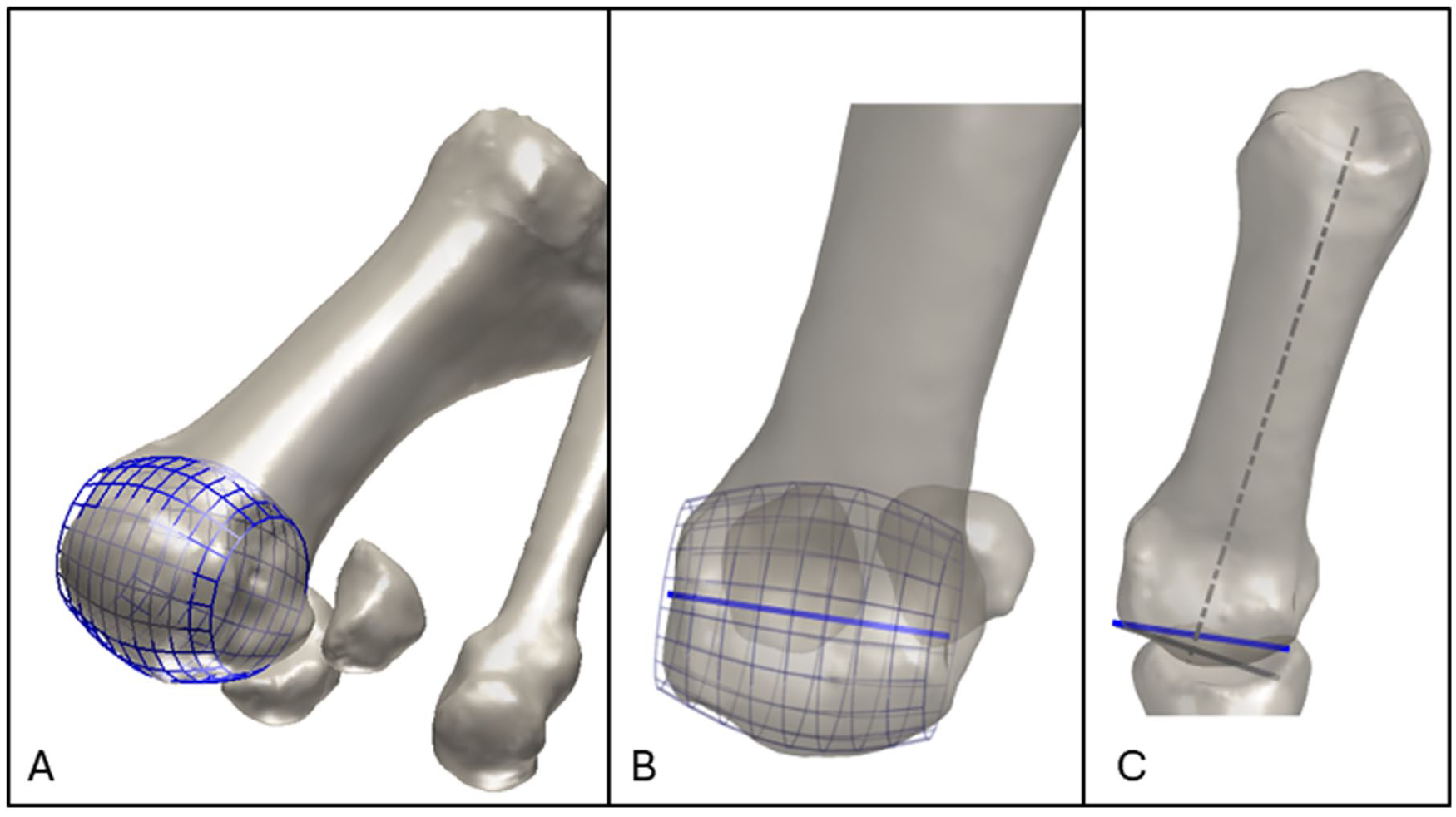
First, a modulated cylinder was fitted to the surface of the M1 head, excluding the medial and lateral sides. This fitting routine automatically finds the location, direction, and radius of the cylinder, together with cylinder fitting parameters. The coronal and axial axes of this cylinder were then determined relative to the longitudinal axis of M1 (Figure 1).
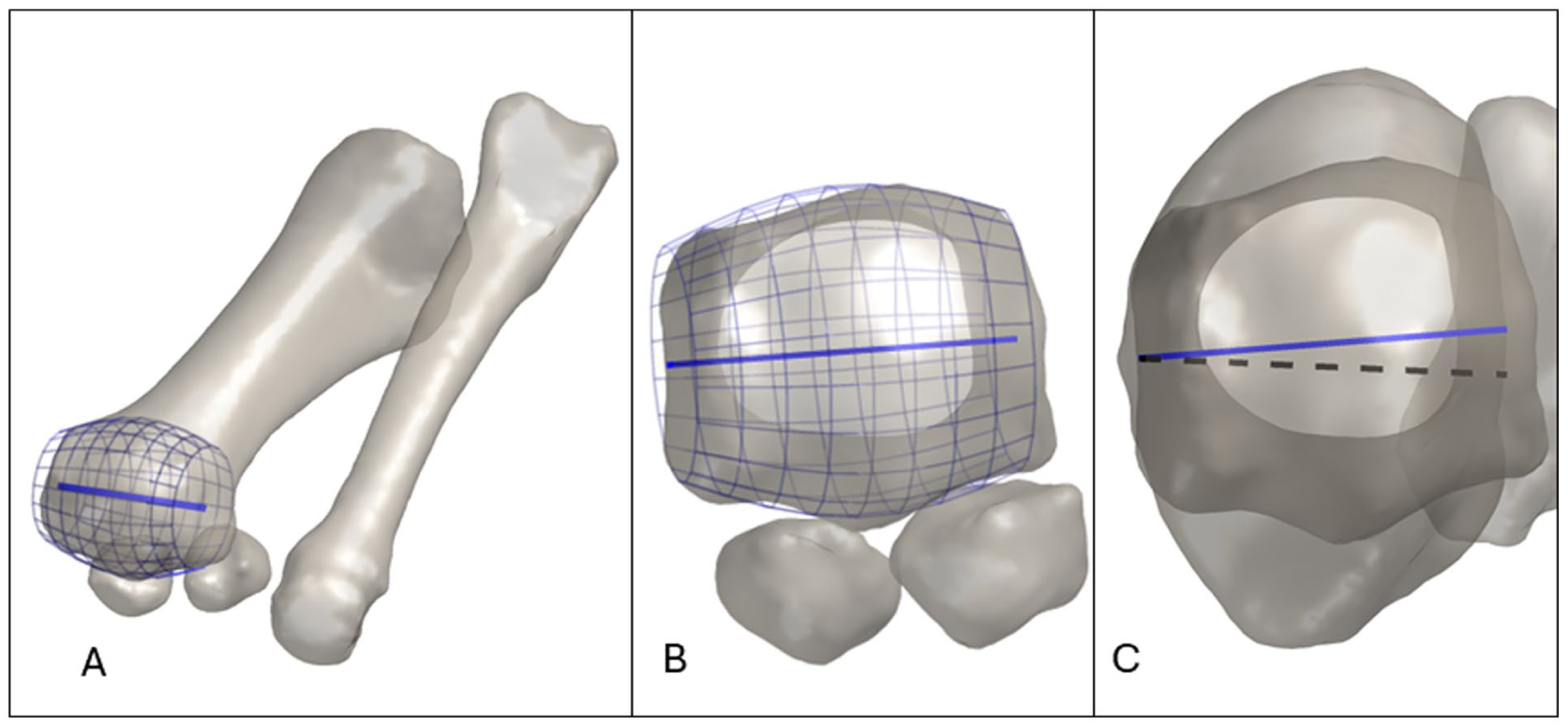
First metatarsal head coronal rotation measurement using the cylinder method. (A) Fitted cylinder method: software automatically finds the location, direction, and radius of the cylinder, together with cylinder fitting parameters. (B) Coronal representation of the M1 distal end axis approximated by the cylinder method (cylinder axis, dark blue line). (C) M1 head coronal rotation (dark blue line) relative to the ground (black pointed line) using the cylinder method.
Gutters method
Second, we automatically calculated the axis of the sesamoid gutters in the coronal plane; the distal end of M1 was isolated and projected along the entire longitudinal axis of the bone. The projection of the distal end of M1 was split into 2 subsets containing 20% of the most medial points of the medial side of the distal end and 20% of the most lateral points of the lateral side of the distal end of M1. Then the 2 subsets were combined to create a convex hull. From the resulting convex hull, we picked the edge that pointed downwards where one edge endpoint belonged to the medial subset and the other belonged to the lateral subset. Ultimately, this edge became finally our gutter axis (Figure 2).
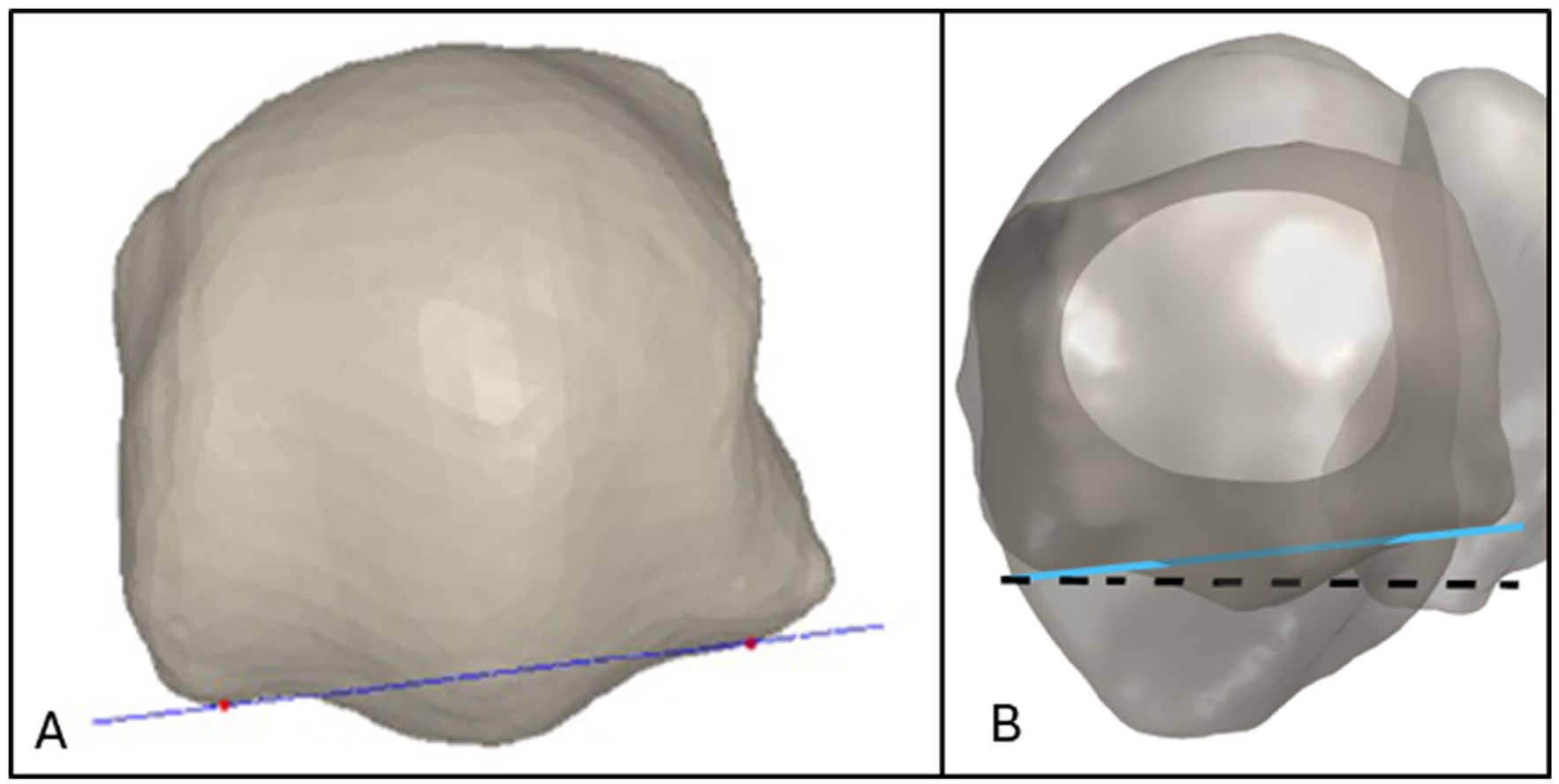
First metatarsal head coronal rotation measurement using the gutters method. (A) Gutters line method: the 2 red points represent the edge that pointed downwards, where one edge endpoint belonged to the medial 20% subset and the other belonged to the 20% lateral subset of M1 gutter. These 2 points were used to determine the axis of M1 gutter (dark blue line) to measure M1 pronation relative to the ground. (B) M1 head coronal rotation relative to the ground (dark pointed line) using the gutters method (light blue line).
Automatic 3D Measurements of the M1 Base Rotation
The M1 base axis and its rotation along the longitudinal axis of M1 were determined using 2 methods.
PCA method
First, we used a principal components analysis (PCA) for the proximal articular surface of M1. We extracted points belonging to the articular surface area and applied the PCA method to identify the main directions of variance in the 3D point cloud. The first principal component explaining the largest variation represents the inferior-superior axis. The second component is perpendicular to the first component and corresponds to the medio-lateral axis. Then the near medio-lateral component was used in the direction of the longitudinal axis of M1 (Figure 3A).
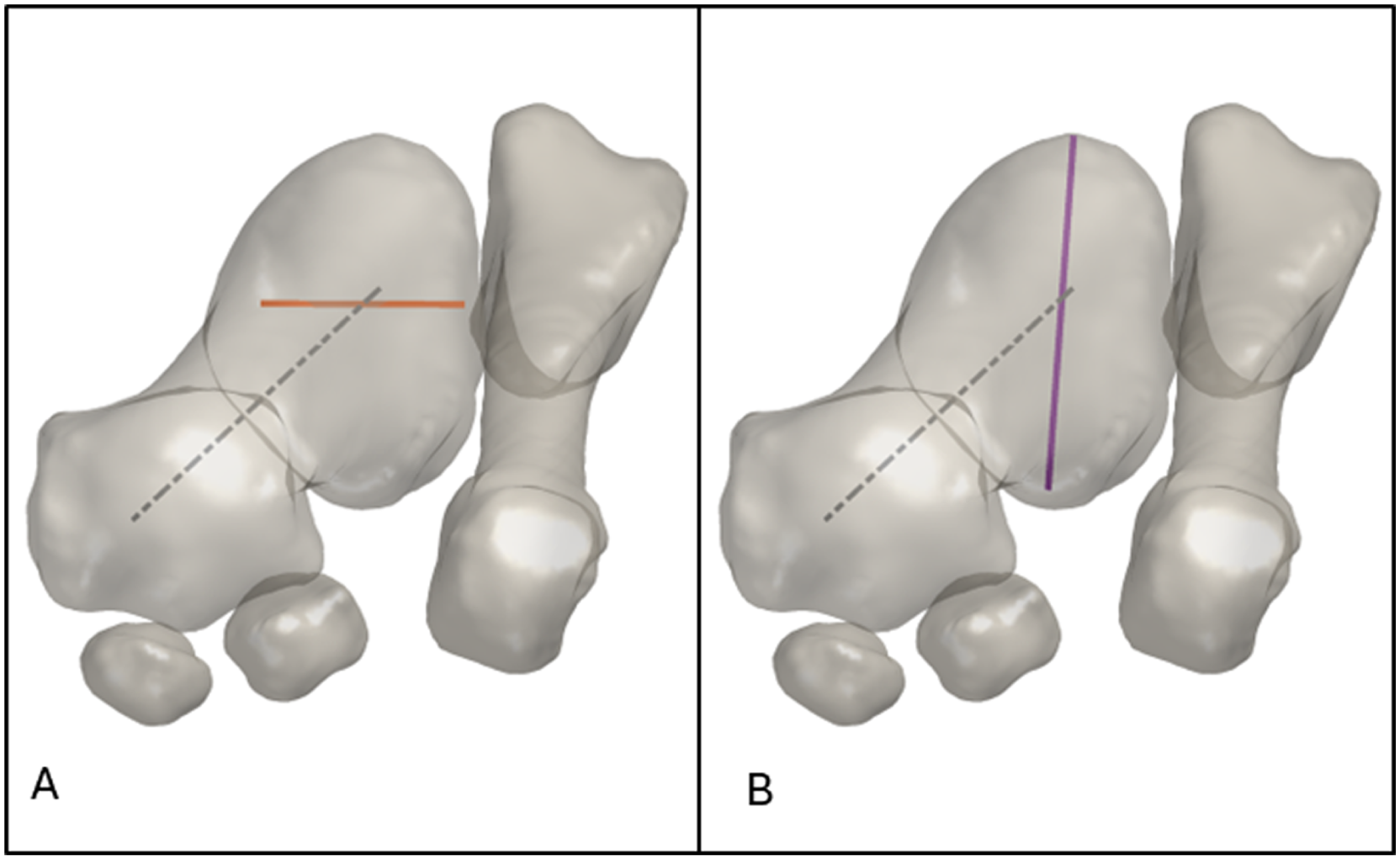
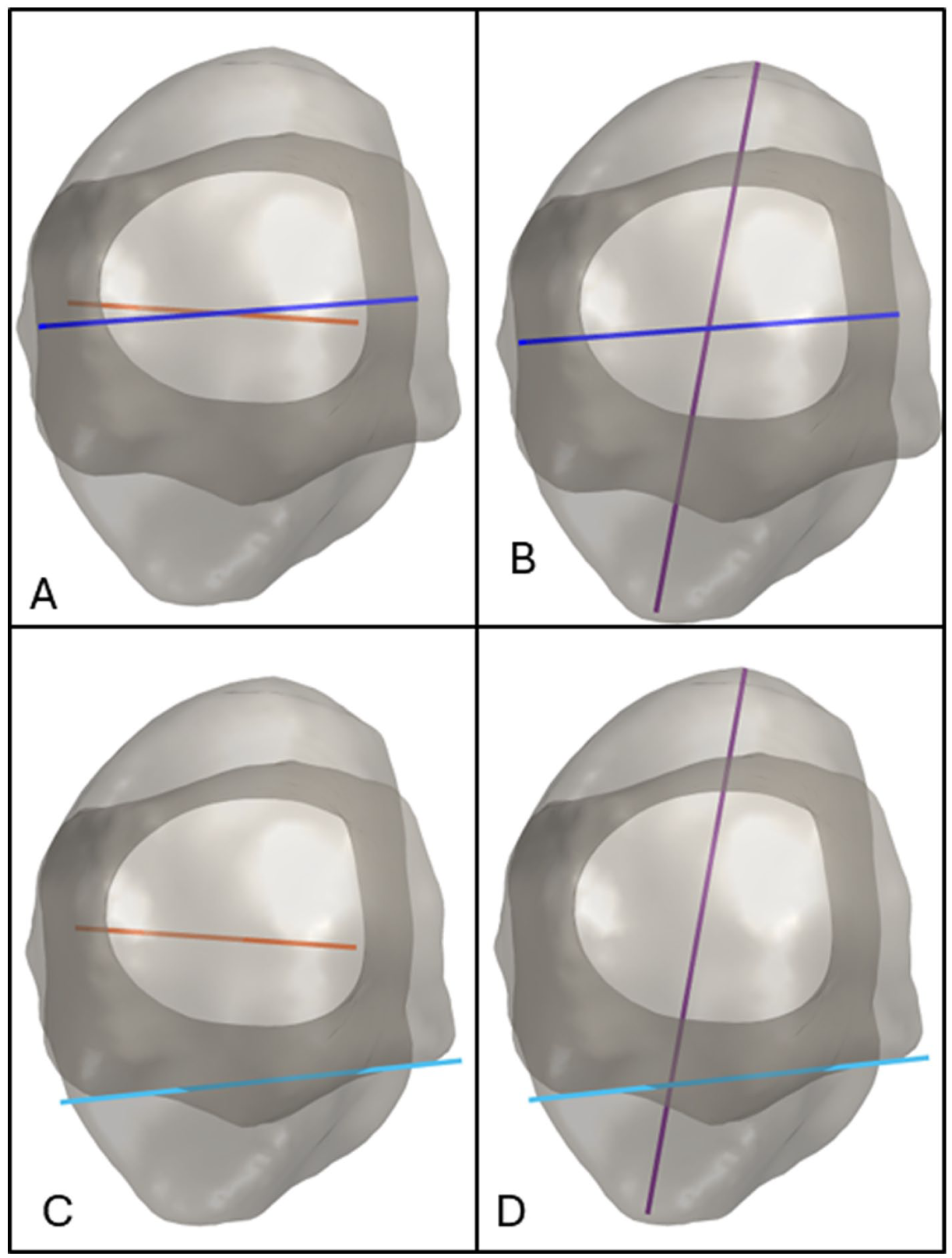
First metatarsal base coronal rotation measurements. (A) PCA method: points belonging to the articular surface area of M1 are extracted, and then the PCA method is applied to identify the main directions of variance in the 3D point cloud. The first principal component explaining the largest variation represents the inferior-superior axis. The second one is perpendicular and represents the medio-lateral axis. Then the near medio-lateral component was used in the direction of the longitudinal axis to measure axis of proximal articular surface of M1. This component is represented as the orange line. (B) Diagonal method: the software automatically located the highest and lowest points on the articular surface of M1. These 2 points were used to draw the longest diagonal and therefore the axis of the base of M1 (purple line). The angle between this line and the vertical axis was used to measure the axis of the base of M1.
Diagonal method
Second, as reported by Ota et al, 9 the longest diagonal of the M1 base was calculated, and the angle between the vertical axis and the axis of this diagonal was determined (Figure 3B).
Automatic 3D Measurements of the M1 Intrinsic Torsion
The various combinations of these 4 methods (2 for the M1 head and 2 for the M1 base) were then used to assess the M1 intrinsic torsion, which was determined as the angle between the M1 head axis and the M1 base axis, resulting in four measurements: Cylinder-PCA method, Cylinder-Diagonal method, Gutters-PCA method, and Gutters-Diagonal method (Figure 4).
First metatarsal intrinsic torsion measurements. (A) Cylinder-PCA method: the angle between the fitted cylinder method axis (dark blue line) and the PCA method (orange line) was used to calculate the intrinsic torsion of M1. (B) Cylinder-Diagonal method: the angle between the fitted cylinder method axis (dark blue line) and the longest diagonal method axis (purple line) of M1 base method was used to calculate the intrinsic torsion of M1. (C) Gutters-PCA method: the angle between the gutter method axis (light blue line) and the PCA method axis (orange line) was used to calculate the intrinsic torsion of M1. (D) Gutters-Diagonal method: the angle between the gutter method axis (light blue line) and the longest diagonal method axis (purple line) of M1 base method was used to calculate the intrinsic torsion of M1.
Automatic 3D Measurements of the Distal Metatarsal Articular Angle
The distal metatarsal articular angle (DMAA) was measured as the angle between the perpendicular to the M1 longitudinal axis and the medio-lateral axis of the cylinder model in the axial plane (Figure 5).
Valgus deviation of the first metatarsal distal articular surface measurement (distal metatarsal articular angle). (A) Fitted cylinder method as explained in Figure 1A. (B) Axial representation of the M1 distal end axis approximated by the cylinder method. (C) Distal metatarsal articular angle measurement using the cylinder method: dark blue line represents the axial axis of the distal head of M1 approximated by the cylinder method, and the gray line represents the perpendicular to the M1 longitudinal axis in the axial plan. DMAA is the angle between the gray and dark blue lines.
Statistical Analysis
Normality and hetereoskedasticity of continuous data were assessed with Shapiro-Wilk and Levene test, respectively. Continuous outcomes were compared with unpaired Student t test, Welch t test, or Mann-Whitney U test according to data distribution. Discrete outcomes were compared with χ2 or Fisher exact test accordingly. The intraclass correlation coefficient (ICC) was used to assess the interobserver and intermethod reliabilities. Spearman coefficients were used to assess correlations. The alpha risk was set to 5%, and 2-tailed tests were used. Multiple parameters were compared between the HV and control groups. Given the number of comparisons, the risk of type I error was acknowledged. These analyses were considered exploratory, with emphasis placed on effect sizes and 95% CIs. Statistical analysis was performed with EasyMedStat (version 3.36; www.easymedstat.com).
Results
The mean HVA was 12.5° ± 5.5° in the control group and 26.9° ± 10.2° in the HV group (P < .001). The mean IMA was 11.1° ± 2.1° in the control group and 15.4° ± 3.5° in the HV group (P < .001).
Reliabilities
Interobserver reliability for α angle and MPA was excellent (ICC = 0.95 and 0.96 respectively, P < .001).
Reliabilities between α angle and M1 head rotation using the cylinder (ICC = 0.46; P < .001) and the gutters methods (ICC = 0.49; P < .001) were poor. Reliabilities between MPA and M1 head rotation using the cylinder (ICC = 0.72; P < .001) and the gutters method (ICC = 0.73; P < .001) were moderate.
Other intermethod reliabilities are shown in Table 2.
Measurement Reliability.

Abbreviations: ICC, interclass correlation coefficient; MPA, metatarsal pronation angle; M1, first metatarsal; PCA, principal component analysis.
Correlations
Moderate positive correlations were found between the α angle and M1 head rotation using the cylinder (r = 0.56; r2 = 0.498; P < .001) and the gutters methods (r = 0.59; r2 = 0.484; P < .001). Strong positive correlations were found between MPA and M1 head rotation using the cylinder (r = 0.71; r2 = 0.663; P < .001) and the gutters methods (r = 0.76; r2 = 0.598; P < .001) (Figure 6).
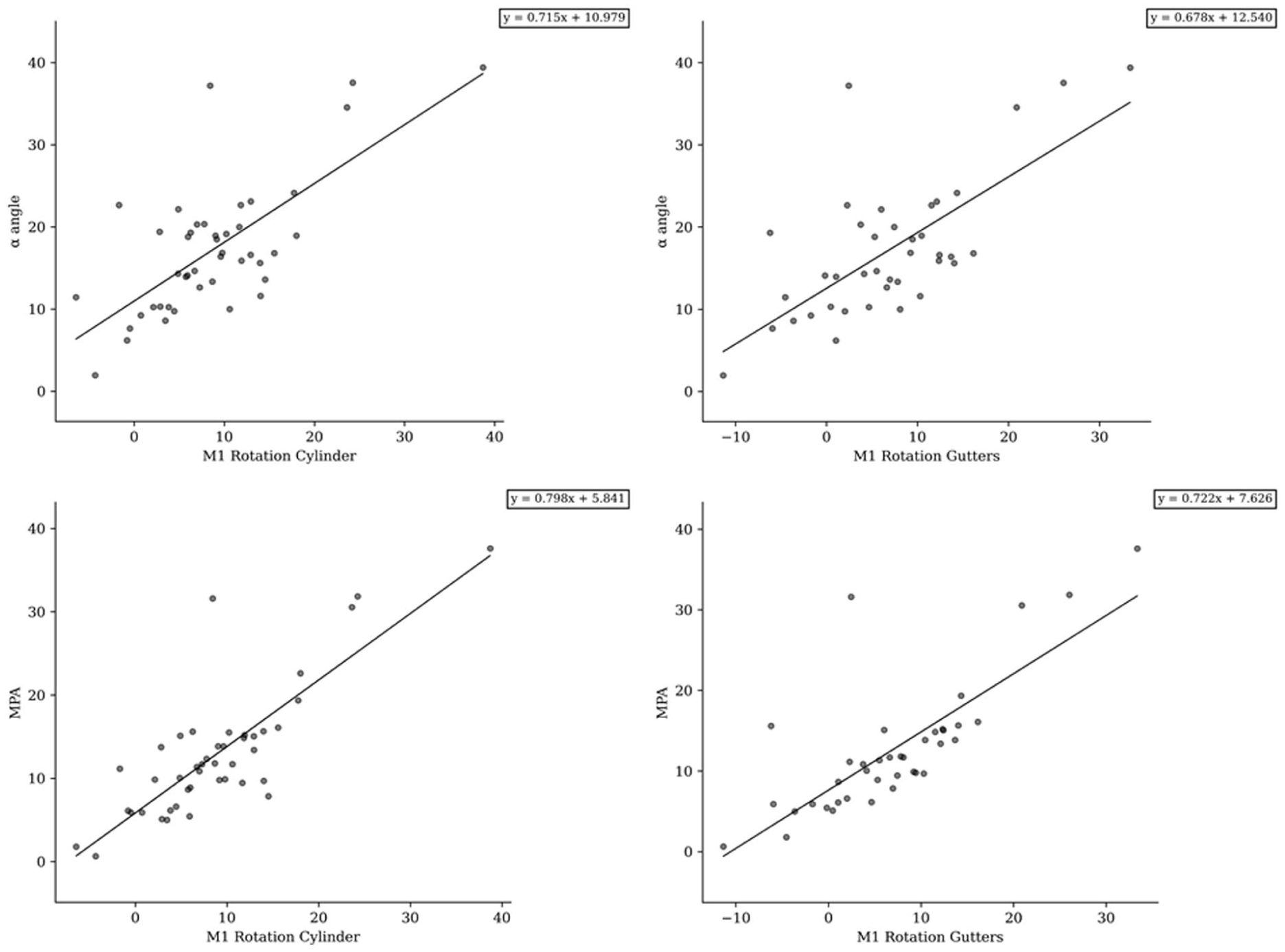
Correlation diagrams between manual and automatic measurements. M1, first metatarsal; MPA, metatarsal pronation angle.
Automatic 3D Measurements of the M1 Head Rotation in HV and Controls
According to the cylinder method, M1 head rotation was respectively 8.9° ± 8.4° and 2.1° ± 6.4° in HV and control groups (P < .001).
According to the gutters method, M1 head rotation was respectively 9° ± 8.3° and 0.7° ± 6.8° in HV and control groups (P < .001).
Automatic 3D Measurements of the M1 Intrinsic Torsion in HV and Controls
According to the Cylinder-PCA method, M1 intrinsic torsion was 4.1° ± 6.9° and 2° ± 5.5°, respectively, in the HV and control groups, with the numbers available, no significant difference could be detected (P = .134).
According to the Cylinder-Diagonal method, M1 intrinsic torsion was 11.8° ± 6.3° and 8.3° ± 5.4°, respectively in the HV and control groups (P = .009).
According to the Gutters-PCA method, M1 intrinsic torsion was 4.3° ± 6.9° and 0.6° ± 5.2°, respectively, in the HV and control groups (P = .011).
According to the Gutters-Diagonal method, M1 intrinsic torsion was 12° ± 6.1° and 6.9° ± 6.3°, respectively, in the HV and control groups (P < .001).
Automatic 3D Measurements of the DMAA in HV and Controls
The mean DMAA was 5.6° ± 4.7° in the control group and 11.4° ± 6.9° in the HV group (P < .001). Thus, the M1 distal articular surface in the HV group was 5.8° more deviated in valgus than in the control group (P < .001).
All automatic 3D measurements are shown in Table 3.
Comparison of HVA, DMAA and Rotational Parameters of M1 in HV and Control Groups.
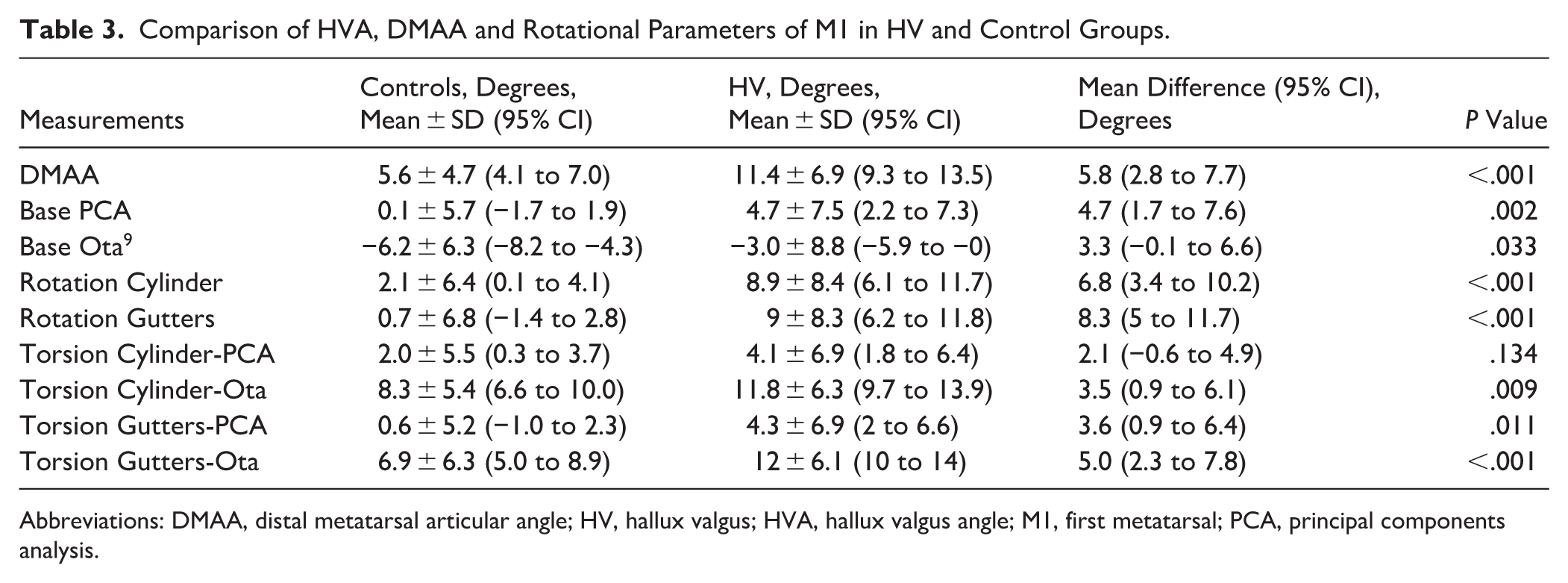
Abbreviations: DMAA, distal metatarsal articular angle; HV, hallux valgus; HVA, hallux valgus angle; M1, first metatarsal; PCA, principal components analysis.
Discussion
It was found that HV showed an increase in M1 head pronation relative to the ground of 7° to 8° greater than controls, with an increase in M1 intrinsic torsion in pronation of 2° to 5°, which confirmed part of our hypothesis. On the other hand, contrary to our hypothesis, automatic measurements showed an increase in valgus deviation of the M1 distal articular surface of approximately 6° in HV compared with controls.
According to the automatic measurements of M1 head pronation relative to the ground, using the gutters method alone showed a greater increase in pronation in HV patients compared with the cylinder method (Table 3), which considered the entire M1 head morphology. This suggested that the pronation values were substantially influenced by the position of the sesamoid gutters.11,32 However, this study could not determine whether the pronated malposition of the gutters was secondary or constitutional. One could argue that metatarsosesamoid arthritis and inherent gutter erosion1,33 might explain the pronated malposition of the gutters. Nonetheless, it could also have been due to a developmental anomaly of the M1 head, and this study did not provide evidence to support either theory. Given these results, gutter-independent measurements, such as the cylinder method, could be more reliable. Additionally, the magnitude of M1 head pronation in our study is similar to those reported in previous studies.10,34
It is also surprising to observe that the M1 intrinsic torsion in pronation that we found, independently of the method, was notably lower (2°-5°) than those previously reported in the literature.7,8,10 -12,19,34 -37 For example, Ota et al 9 reported an increase in intrinsic torsion of M1 of around 13° more in HV compared with controls. Our values are much lower and closer to those reported by other authors. 29 This should reopen the debate on whether the pronation of the M1 head originates from an intrinsic torsion of that bone or not. According to our study, this pronation malposition may be proximal to M1 and could be present at the level of the first tarsometatarsal joint as previously reported,29,38 or originate directly from a valgus position of the hindfoot.8,39,40 Future studies that explicitly account for these confounding factors would be warranted.
Another important matter of debate was the existence of a valgus deviation of the M1 distal articular surface in HV. The DMAA was initially described to quantify this deviation using 2D dorsoplantar conventional radiographs. However, numerous authors criticized this angle, suggesting it might be solely an artifact of M1 head pronation relative to the ground, which causes the lateral plantar condyle (which is round) of the M1 head to be superimposed with its distal articular surface.6,16 Other authors proposed three-dimensional measurements of the DMAA after computerized correction of M1 head pronation relative to the ground, finding a remaining increase of approximately 8° of valgus deviation in HV compared with controls. 12 In our study, we also found a 6° increase in valgus deviation using the automatic cylinder method, which accounted for the overall morphology of the M1 distal end. This study supported the hypothesis that even though valgus deviation of the M1 distal articular surface is overestimated on dorsoplantar conventional radiographs, partially because of pronation, some degree of increase in valgus deviation remains in the HV. This supports both previous sides of the literature in that the DMAA really exists but is only part of M1 dysplasia in HV combined with M1 intrinsic torsion.
The gutter method showed closer agreement with currently used manual measurements, namely, the alpha angle and the metatarsal pronation angle, compared with the cylinder method. However, these measurements are all largely dependent on the orientation of the sesamoid groove and therefore may primarily reflect gutter position rather than the morphology of the entire metatarsal head. In addition, the gutter region may be influenced by local anatomic changes, including metatarsosesamoid arthritis or gutter dysplasia. For this reason, although our results do not demonstrate superiority of the cylinder method, a gutter-independent approach based on the overall geometry of the metatarsal head may still be of interest. This interpretation should remain cautious, as it reflects a conceptual advantage rather than a finding directly established by the present study.
One of the aims of this study was to explore the transition from manual to automated measurements of first metatarsal morphology. Although agreement with currently used manual measurements was not perfect, this may reflect not only measurement limitations but also the fact that manual 2D and automated 3D approaches do not assess exactly the same constructs. 41 A 2-dimensional measurement cannot be expected to fully reproduce the 3-dimensional geometry of the first metatarsal. In this respect, automated 3D analysis may provide a more objective and less observer-dependent assessment of metatarsal morphology, which could be particularly valuable for future large-scale studies. The fact that our findings are broadly consistent with previous literature may also be considered a strength in the context of a validation study, as it suggests that the automated approach captures morphologic patterns already identified using established methods.
The interpretation of the cylinder-based measurement as a surrogate for distal articular valgus should remain cautious. Because we did not perform manual DMAA or 3D DMAA measurements, we were unable to directly validate this parameter against established articular measurements. Accordingly, our findings regarding distal articular valgus should be considered more exploratory than those related to M1 head rotation relative to the ground and intrinsic M1 torsion, which were the main focus of the present study.
This study presented several limitations. First, we did not consider whether or not HV was combined with flatfoot deformity, which could be seen as a confounding factor.8,39,40 However, we focused on a standard cohort of HV patients who consulted for a painful bunion rather than a painful flatfoot, and some studies suggest the absence of impact of asymptomatic flatfoot deformity on both post-operative surgical correction and on functional outcome. 42 Second, the method we described is dependent on the software we used, which may differ from one center to another. Nonetheless, this software is commercially available and can be used by any foot and ankle specialist. Third, we decided to use the ground as a reference to measure first metatarsal pronation. This measurement allows, with an extrinsic reference to the patient, the assessment of first metatarsal pronation independently of other midfoot and hindfoot deformations and focuses on the amount of pronation at the distal M1 head. However, Conti et al 10 showed different measurements of first metatarsal pronation when using a patient-intrinsic reference such as the second metatarsal axis. This approach allows for considering patient-intrinsic deformation in the calculation of first metatarsal pronation (as the whole foot pronates in asymptomatic flatfoot deformity, for example). It should be noted that, depending on the reference selected to measure first metatarsal pronation, there is no correlation between the different measurements, and the choice of one or the other reference (ground or second metatarsal) will have an impact on surgical planning. No gold standard has been defined yet. Fourth, although WBCT is a weight-bearing imaging modality, it remains a static assessment. Although intrinsic M1 torsion and DMAA are not influenced by this static nature, as they reflect purely osseous deformities, the rotation of the M1 head relative to the ground is not evaluated dynamically and does not capture its variation during gait. Fifth, this was a retrospective study conducted on a small cohort, with inherent potential biases. However, to our knowledge, this is the first study to describe automatic methods for assessing pronation and valgus deviation of the M1 distal articular surface in HV and controls. Sixth, several geometric parameters were analyzed. As this is an exploratory study, no formal correction for multiple comparisons was applied, and the results should therefore be interpreted with caution. Effect sizes and 95% CIs are provided to highlight the clinical relevance of the findings. Lastly, another limitation is that a small number of patients contributed both feet to the analysis, which may have introduced some degree of within-patient dependence, although this concerned only a limited proportion of the cohort.
Conclusion
Using automatic 3D WBCT measurements, we found that HV showed an increase in M1 head pronation relative to the ground of 7° to 8° greater than controls, with an increase in M1 intrinsic torsion in pronation of 2° to 5°. An increase in valgus deviation of the M1 distal articular surface of approximately 6° in HV compared with controls was also observed. Changing measurements reference points altered angular values in our study, particularly when moving from measurements based on the sesamoid gutters to gutter-independent measurements, highlighting that these methods may capture different anatomic constructs. These automated measurements should be used to generate large data sets, providing a more accurate and standardized, objective approach to address questions regarding pronation in HV.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114261448850 – Supplemental material for Automated 3-Dimensional Measurements of First Metatarsal Dysplasia in Hallux Valgus
Supplemental material, sj-pdf-1-fao-10.1177_24730114261448850 for Automated 3-Dimensional Measurements of First Metatarsal Dysplasia in Hallux Valgus by Luc Meuric, Matthieu Lalevée, Nacime Salomao Barbachan Mansur, Scott Ellis, Albert DaCosta, François Lintz, Matthew S. Conti and Cesar de Cesar Netto in Foot & Ankle Orthopaedics
Footnotes
ORCID iDs
Ethical Considerations
Ethical approval for this study was obtained from the University of Iowa Hospitals & Clinics Review Board (IRB : 201904825).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Scott Ellis, MD, reports disclosures relevant to manuscript of Paragon 28 (Now Zimer-Biomet): paid consultant, product development (with royalties); Stryker/Wright Medical: paid consultant, product development (with royalties); Vilex: paid consultant, product development (with royalties); Medartis/Nextremity: paid consultant, product development (with royalties), now with IBRA (International Bone Research Association); FAI/FAO reviewer: current reviewer for both journals, previous Associate Editor for FAO; managerial board of FAI/FAO; Foot Innovate: leadership team, paid consulting; WBCT Society: board member, no direct payment incentive; Curve Beam (indirectly through Stryker and the International WBCT society); editor for Master Techniques in Foot and Ankle Surgery (Wolters Kluwer); Extremis Robotics: consultant and shareholder; Extremity Medical: leadership board of directors, equity; Elsevier (guest editor, Foot and Ankle Clinics); Wolters Kluwer (Master Techniques in Foot and Ankle Clinics) and Springer (fourth edition of Operative Techniques in Orthopaedic Surgery [PCFD book]); JEASO DME HSS initiative (Joint Effort Administrative Services Organization) which invests into the Recovery Shop, LLC (DME at HSS); Healio Orthopaedics Today, editorial board; HS2, LLC: stock or stock options; ADN Ambulatory Surgery Center Holding Company, HSS; and One Ortho Holdings, LLC. François Lintz, MD, PhD, reports disclosures relevant to manuscript of Newclip Technics: royalties; CurvebeamAI: stock; Podonov/Enovis: royalties; Paragon28/Zimmer-Biomet: consulting. Matthew S. Conti, MD, reports disclosures relevant to manuscript of BICMD, Inc: consulting payments; Extremity Medical: consulting payments; SIMULATE Technologies: equity; Paragon28: consulting payments; Medline UNITE: consulting payments; DJO Foot and Ankle: consulting payments; Joint Effort Administration Services Organization: equity; Ossiform Aps: consulting payments. Disclosure forms for all authors are available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.