
Abstract

Introduction
The foot represents a very rare site of primary bone and soft tissue tumors, accounting for less than 1% of all sarcomas; the forefoot is a relatively common site among foot sarcomas. 1 The first metatarsal plays a crucial role in load bearing and gait, making its reconstruction crucial after tumor resection. 2 Several reconstructive options have been described, including massive allografts, iliac crest autografts, and vascularized fibular grafts (VFGs).3 -8 VFG offers biological advantages compared with nonvascularized reconstructions, such as earlier union, remodeling, and hypertrophy under mechanical stress—although union typically requires several months and hypertrophy up to a year—even after adjuvant therapies; furthermore, considering metatarsal reconstructions, VFG has a similar shape and diameter of the host bone.
The aim of this work is to describe our technique for the reconstruction of the first metatarsal with VFG after resection for bone and soft tissue sarcoma, reporting its complication rate and functional result, and discussing their advantages and drawbacks in the long term.
Indications and Contraindications
VFG reconstruction is usually adopted in our institution after resection of the first metatarsal bone for primary malignant or aggressive benign tumors in patients with long life expectancy and high functional demands. In contrast, in metastatic patients without long life expectancy or in old patients, we prefer to perform a first ray or Lisfranc amputation, according to tumor extension. Perioperative chemotherapy does not represent a contraindication for this reconstruction as well as preoperative radiotherapy; however, preoperative radiotherapy may alter skin quality and recipient vessel integrity, increasing intraoperative and wound-healing complexity. This reconstruction should be avoided if postoperative radiotherapy is required, to not jeopardize VFG biological properties in terms of remodeling, early fusion, and spontaneous healing after fracture.
Technique
Operations are performed with the patient in supine position, through an incision on the medial aspect of the foot, that provides a straightforward exposure of the first metatarsal, disarticulating both the first metatarsophalangeal and tarsometatarsal joints (Figure 1). If involved, the second metatarsal has to be resected along with the first using a dorsal approach.

Figure shows the surgical approach in (A) the medial aspect of the foot excising the previous scar after a local recurrence of a giant cell tumor of bone, (B) disarticulating both the first metatarsophalangeal and tarsometatarsal joints.
The VFG is harvested by a microsurgical team using separate instruments through a posterolateral approach from the contralateral leg, to avoid contamination between the 2 surgical fields and to reduce the surgical time thanks to the simultaneous work of the 2 teams. Although this may affect both lower limbs, we usually prefer to adopt the contralateral fibula, considering the low incidence of donor site complications in our experience. The harvested fibula should be 1 cm longer than the first metatarsal to restore the length of the medial column after cartilage burring, with a median length of the metatarsal defect in our series of 6.5 cm (5.5-7) (Figure 2). VFG can also be harvested as an osteo-cutaneous flap with the skin island based on its perforator vessels, to cover a skin defect secondary to tumor excision.

Figure shows (A) the harvested fibula, then (B) fixed in an arthrodesis-like fashion using a nonbridging fixation with two separate plates.
The first phalanx and the medial cuneiform articular cartilages are burred, then the fibula is inserted inside the defect and fixed through an arthrodesis. Bone fixation can be performed either using a nonbridging fixation with two 2.4-mm or 2.7-mm plates or a bridging plate fixation; the use of thin plates is advised to achieve a less bulky reconstruction (Figure 3). The metatarsophalangeal arthrodesis has to be performed in a slight (10°-20°) extension, to easily allow the stance during the walk (Figure 4).

Figure shows the 2 types of fixation described: (A) Bridging fixation with a single plate. (B) Nonbridging fixation with 2 separate plates.

Figure shows the metatarsophalangeal arthrodesis performed in a slight extension, to easily allow the stance during the walk.
After VFG fixation, the vascular pedicle of the flap, including the peroneal artery and one of the 2 venae comitans, is anastomosed with recipient vessels in an end-to-end fashion. The peroneal artery is anastomosed with the medial plantar artery when the medial approach is adopted, and with the dorsalis pedis artery using the dorsal approach; one of the comitans venae is anastomosed with the subcutaneous dorsal vein, according to their larger size compared with the dorsalis pedis vein. Given the relatively long pedicle of the fibula flap, particularly after preoperative radiotherapy, an anastomosis with the anterior tibial vessels in a non-irradiated field would reduce the risk of failure.
All patients received perioperative antibiotic prophylaxis with intravenous vancomycin (1 g every 12 hours) and piperacillin and tazobactam (4.5 g every 8 hours), which is continued until drain removal. After surgery, the operated foot is protected with a below-knee cast for 4 weeks, to protect the fibula and the osteotomy fixation during the early postoperative period. Controlled passive movements of the ankle are then allowed. No weightbearing is allowed until radiographic evidence of VFG union; then the patient could walk with partial weightbearing. Full weightbearing is started after evidence of complete VFG union, which in our series occurred 6 months after primary surgery in all patients who retained their graft. The donor leg is left free postoperatively, encouraging active and passive movements of the knee, ankle, and toes. Full weightbearing on the donor side is allowed after 3 weeks from surgery.
Complications
Between 2004 and 2021, 3 patients were treated at our institution for a primary bone or soft tissue malignant or benign aggressive tumor with resection of the first metatarsal and reconstruction with VFG. Descriptive data are reported in Table 1.
Patient Characteristics.
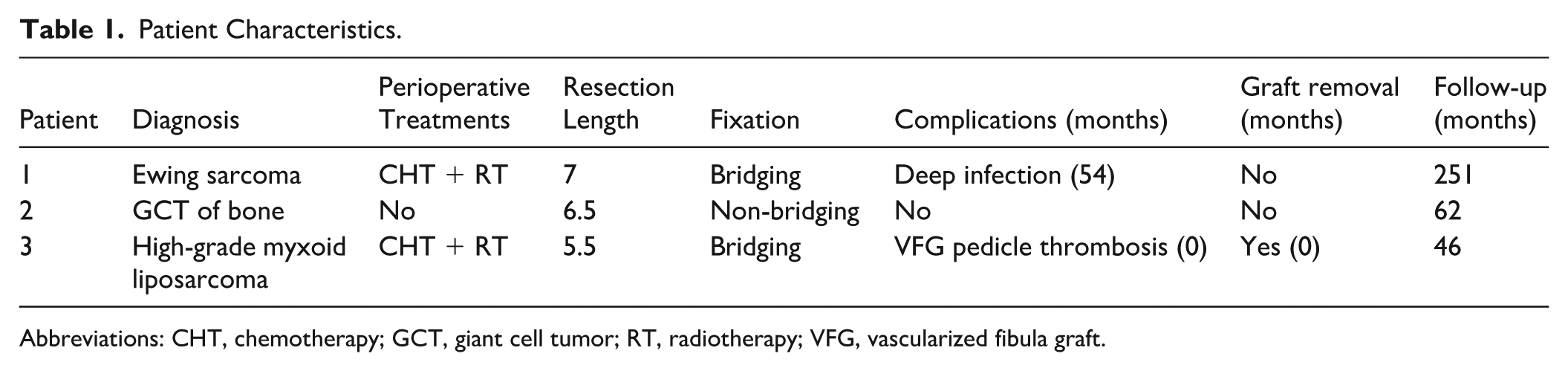
Abbreviations: CHT, chemotherapy; GCT, giant cell tumor; RT, radiotherapy; VFG, vascularized fibula graft.
None of the patients had donor site complications. During follow-up, 1 patient had a deep infection after 54 months from surgery, healed after surgical debridement with a screw removal and intravenous antibiotics administration; the other patient underwent excision of a high-grade myxoid liposarcoma infiltrating the first 2 metatarsal and part of the dorsalis pedis vessels after preoperative chemo- and radiotherapy, had a thrombosis of the pedicle 12 days after primary surgery leading to a necrosis of the skin pad and of the first toe that was managed with a Lisfranc amputation; this complication could be related both to the neoadjuvant radiotherapy and to the double arterial anastomosis performed distally between the peroneal artery and the lateral digital artery, and proximally with the dorsalis pedis artery, in an attempt to salvage the forefoot. No nonunions or fractures were assessed. At last clinical control, at a median of 156 months (range, 62-251) from primary surgery, both patients that retained their VFG regularly long-walk and practice nontraumatic sport activities, with a Musculo-skeletal Tumor Society (MSTS) score of 30 in both and an American Orthopaedic Foot & Ankle Society (AOFAS) midfoot score of 90 and 100, respectively. Ankle motion on the fibula donor side was complete and painless in all patients.
Discussion
Despite a high rate of complications leading to further surgeries, VFG reconstruction allows for an effective reconstruction with excellent long-term functional results.6 -8 Using this technique, a high risk of perioperative complications should be expected, particularly in patients who have undergone preoperative radiotherapy; however, once healed, the autologous fibula graft allows for a durable long-term reconstruction also in this group of patients. Soft tissue coverage is often required in the foot, but the VFG harvesting with its skin paddle increases surgical complexity and complication rates and should be reserved only for patients with skin defects 8 ; in case of tumor extension in the sole, free flaps coverage or a Lisfranc amputation should be considered, considering the high mechanical stress during weightbearing.
Despite the high mechanical stress affecting the first ray, neither fractures nor nonunions have been assessed even when using a nonspanning fixation, likely reflecting the ability of VFG to hypertrophy under mechanical stress6 -8; therefore, in metatarsal reconstructions, a nonbridging fixation using 2 different plates may be advised, in order to enhance the fibula remodeling, and to achieve a compression of both osteotomies, with a less bulky reconstruction. Although spanning fixation is usually advised after VFG reconstruction to protect the graft from fractures, it does not appear to be recommended at this site. In contrast to that reported from other authors, 7 first metatarsophalangeal joint restoration is not mandatory to enable the gait6,8; therefore, according to the restricted mobility of mid- and forefoot joints, we prefer to fix the fibula through 2 different arthrodesis, with the metatarsophalangeal arthrodesis performed in slight extension, to easily allow the stance during the walk.
Good outcomes have been reported after first metatarsal reconstruction with nonvascularized graft, either autologous iliac crest graft, fibula graft or fibular allograft, after resection for benign aggressive tumor.3 -5 None of these patients underwent adjuvants therapies; therefore, in this situation nonvascularized grafts may be enough. In contrast, in patients in whom perioperative treatments are required, the reconstruction using a VFG may be advised.7,8 Finally, in our experience, the harvest of the fibula graft did not affect the ankle motion and the syndesmosis stability on the donor side, according to the relative short length of the fibula resection, also considering long-term follow-up.
Conclusion
VFG may represent a viable reconstructive option to reconstruct a functional and cosmetic foot after first metatarsal resection for primary bone and soft tissue tumors; in this small preliminary series, satisfactory long-term functional results were achieved in patients who retained their graft, although a high perioperative complication rate should be anticipated. This technique may be considered for active patients with long life expectancy and high functional demands, particularly when perioperative adjuvant therapies are required. Larger comparative studies are warranted to assess the potential benefits of one technique over the other.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114261440468 – Supplemental material for First Metatarsal Reconstruction After Resection for Musculoskeletal Tumors: A Technical Tip Using Vascularized Fibula
Supplemental material, sj-pdf-1-fao-10.1177_24730114261440468 for First Metatarsal Reconstruction After Resection for Musculoskeletal Tumors: A Technical Tip Using Vascularized Fibula by Roberto Scanferla, Francesco Muratori, Laura Fratangelo, Luca Delcroix and Domenico Andrea Campanacci in Foot & Ankle Orthopaedics
Footnotes
Ethical Considerations
The present retrospective observational study was approved from our local institutional review board; ref. 10197/2017.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Disclosure forms for all authors are available online.
Data Availability Statement
All data generated or analyzed during this study are included in this published article.
Patient Consent
All participants provided written informed consent prior to participating.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.