
Abstract
Background:
Weber B ankle fractures with medial clear space (MCS) widening on stress radiographs are unstable injuries that may require surgical stabilization. Initial emergency department management varies, with patients receiving a cast or splint after reduction, although concerns for soft tissue complications often limit cast use. It remains unclear whether splint or cast immobilization affects clinical or radiographic outcomes.
Methods:
We retrospectively reviewed 295 patients treated for closed Weber B ankle fractures between January 1, 2017, and February 15, 2025; among them, 96 were determined to have an unstable pattern based on MCS widening on stress radiographs. Inclusion criteria were age ≥18 years, isolated fibular fracture with MCS widening indicating deltoid incompetence, and ankle radiographs at initial, postreduction, and follow-up time points. Patients with bimalleolar or trimalleolar fractures were excluded. We compared MCS values, surgical rates, reduction attempts, and complications across initial immobilization types.
Results:
Postreduction MCS was significantly smaller in the cast group compared to the splint group (2.79 ± 0.50 vs 3.41 ± 0.83 mm, P < .01). MCS at follow-up remained lower in the cast group and below the 4-mm threshold commonly used to guide surgical decision making (2.73 ± 0.54 vs 4.14 ± 1.10 mm, P < .01). A greater proportion of casted patients maintained reduction at follow-up (n = 72 vs 19, P = .04), reinforcing the association between initial casting and radiographic stability. There were no statistically significant differences in surgical or complication rates between groups.
Conclusion:
Initial immobilization with a cast in unstable Weber B ankle fractures was associated with improved postreduction and follow-up radiographic alignment measured by MCS. The absence of increased complication rates among cast patients indicates that the superior radiographic stability with casting is not offset by increased complications, although the study may have been underpowered to detect a difference in safety profiles. Future prospective studies can inform the development of standardized immobilization protocols for unstable Weber B fractures.
Level of Evidence:
Level III, retrospective comparative study.

Introduction
Ankle fractures have an annual incidence rate of 4.22 per 10 000 person-years in the United States, with more comprehensive international population studies reporting an incidence of 164 per 100 000 person-years.1,2 Management of ankle fractures varies widely depending on the fracture pattern, ranging from nonoperative to operative approaches. Patients’ preinjury mobility level and comorbid conditions also play an important role in guiding management decisions.
One classification system often used to describe the location and stability of ankle fractures is the Weber classification, where Weber B ankle fractures are defined as fractures of the lateral malleolus at the level of the syndesmosis.3,4 Weber B ankle fractures may be stable or unstable depending on accompanying soft tissue injury—in particular, the competence of the deltoid ligament. 5 Stability is determined by plain film radiograph and stress radiographs with evaluation of the medial clear space (MCS) and tibiofibular overlap. Widening of the MCS is used as an indication of deltoid ligament competence and overall stability, determining the need for surgical intervention. 6 Ankle instability, as defined by MCS widening greater than 4 mm, generally dictates the need for operative intervention with open reduction and internal fixation, whereas stable Weber B fractures, defined as MCS widening less than 4 mm, are generally treated with a period of immobilization.
Initial emergency department management of unstable Weber B ankle fractures varies at our institution, with patients receiving either a non-bivalved cast or splint following initial reduction. Casts are often thought to more stably hold a reduction, although there are concerns that the pressure from circumferential casting in the setting of acute swelling at the time of injury may increase the risk of soft tissue complications such as the formation of pressure ulcers potentially requiring wound debridement or various additional soft tissue interventions. 7 Splints apply less circumferential pressure than casts, potentially mitigating risk of soft tissue complications, but raise concern for loss of reduction and subsequent dislocation or subluxation.8,9 It remains unclear whether cast or splint immobilization influences subsequent clinical or radiographic outcomes, and whether maintaining a better reduction at follow-up may allow patients with this injury to avoid surgery.
The primary aim of this study is to determine whether the initial method of immobilization in unstable Weber B ankle fractures affects the maintenance of an acceptable reduction, defined by MCS measurements, as well as the need for operative intervention. Secondary outcomes include complications associated with the initial immobilization method.
Methods
This study is a single-center retrospective review of all patients presenting with Weber B ankle fractures to a level 1 trauma center between January 1, 2017, and February 15, 2025, for whom the orthopaedic surgery department was consulted. At this institution, it is standard practice for the emergency department to consult orthopaedics for all ankle fractures. A total of 295 patients with Weber B ankle fractures were identified for review in this study.
Inclusion criteria were age ≥18 years, isolated fibular fracture with MCS widening on external rotation stress radiographs indicating deltoid instability, isolated fibular fracture with questionable MCS widening that needed to be stressed to assess stability, and availability of 3-view ankle radiographs at initial presentation, postreduction, and follow-up. Patients with all other fracture patterns were excluded, such as grossly dislocated ankle fractures, as well as patients with incomplete radiographic imaging or lack of follow-up.
Of the 295 Weber B injuries reviewed, 96 were determined to have an unstable Weber B pattern based on MCS widening observed on mortise stress radiographs compared with nonstress radiographs obtained with the ankle in the same position of dorsiflexion and rotation relative to the x-ray beam. At our institution, it is standard practice to immobilize unstable Weber B fractures in either a nonbivalved cast or splint at the discretion of the on-call orthopaedic resident. Casts are constructed with 3M Scotchcast Plus Fiberglass Casting Tape, whereas splints are constructed with Gypsona Plaster of Paris. Postimmobilization 3-view radiographs are routinely obtained. For this study, MCS was measured on prereduction, immediate postreduction, and first clinic follow-up radiographs. The number of reduction attempts, need for surgical intervention, and complications potentially related to the type of initial immobilization, such as wound issues, skin infections, and compartment syndrome, were also recorded. Patient demographics were also collected, including smoking status (packs per day), recreational drug use, diabetes status, and baseline mobility.
Normality of MCS measurements at each time point and for calculated change scores was assessed using the Shapiro-Wilk test. Data were normally distributed for the splint group at follow-up and for the change from postreduction to follow-up, but pre- and postreduction and the change score from pre- to postreduction were not normally distributed. Comparisons between cast and splint groups were performed using independent t tests for normally distributed data and Mann-Whitney U tests for nonnormally distributed data. For nonnormal data, group differences are reported as Hodges-Lehmann estimates with 95% CIs. The analysis assessed whether initial immobilization with a cast vs splint was associated with improved maintenance of reduction at first clinic follow-up, which occurs between 1 and 2 weeks after the date of initial evaluation at our institution, as well as differences in complications and surgical intervention rates between groups.
Results
Of the 96 unstable Weber B patients who were eligible for study inclusion, 74 were initially casted and 22 splinted. The mean age of the cohort was 54 ± 16 years, with no significant difference between casted (55 ± 16 years) and splinted (52 ± 17 years) patients. Females represented 56% of the cohort (n = 54), comprising 45 patients (61%) in the cast group and 9 patients (41%) in the splint group. Diabetes was present in 18 total patients (19%); 14 casted (19%) and 4 splinted (18%). Active smoking was reported by 19 patients (20%); 14 casted (19%) and 5 splinted (22%). Three patients in the cast group had body mass indexes (BMIs) ≥40 (4%) vs 1 patient in the splint group (5%) (Table 1).
Demographics.

Abbreviation: BMI, body mass index.
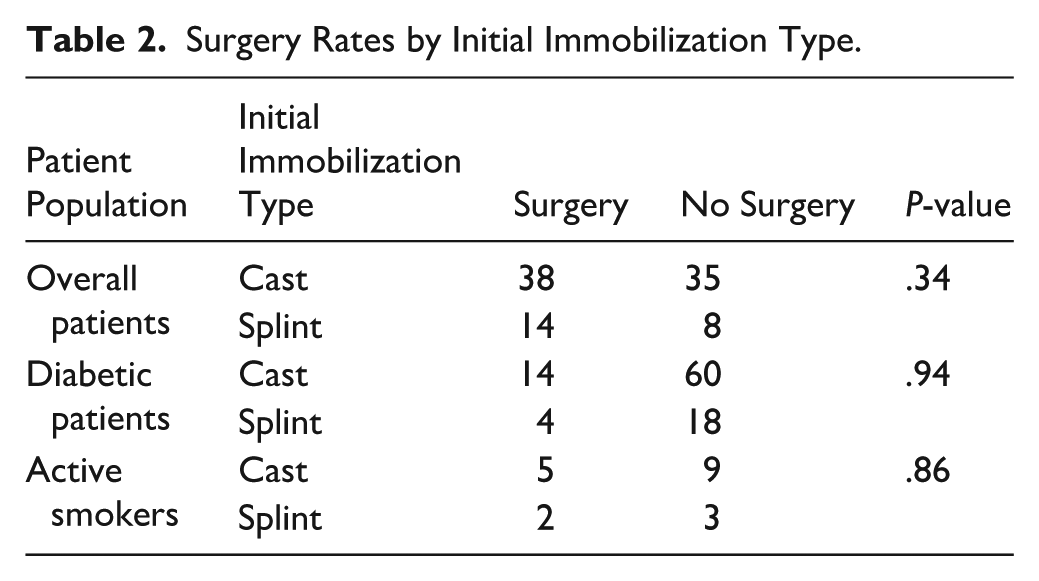
There was no significant difference in surgical rates between casted (n = 38) and splinted patients (n = 14) (P = .34). Additionally, among high-risk patients who underwent surgery, including diabetics and smokers, there was no significant difference in initial immobilization method (P = .94 for diabetics; P = .86 for smokers) (Table 2). Initial prereduction MCS values were not significantly different between groups (6.73 ± 3.01 mm in the cast group vs 7.09 ± 4.18 mm in the splint group, Hodges-Lehmann median difference = 0.09, 95% CI −0.99, 0.99; Mann-Whitney U test, P = .87). The number of patients requiring multiple attempts to achieve reduction also did not differ significantly (n = 4 in cast vs 3 in splint, P = .19). However, postreduction MCS was significantly smaller in the cast group compared to the splint group (2.79 ± 0.50 vs 3.41 ± 0.83 mm, Hodges-Lehmann median difference = 0.49, 95% CI 0.20, 0.79; Mann-Whitney U test, P < .01), and follow-up MCS remained significantly lower in the cast group (2.73 ± 0.54 mm vs 4.14 ± 1.10 mm, mean difference = 1.41, 95% CI 0.93, 1.89; independent t test, P < .01). Figures 1 to 3 depict MCS measurements at times of ankle dislocation, reduction, and clinic follow-up, demonstrating loss of reduction for a patient with a splint. Although the change in MCS from initial injury to immediate postreduction did not differ significantly (Hodges-Lehmann median difference = 0.50, 95% CI −1.67, 2.18; Mann-Whitney U test, P = .25) between groups, the change from postreduction to follow-up was significant, with splinted patients having a greater change in MCS (mean difference = 0.62, 95% CI 0.29, 0.94; independent t test, P < .01), suggesting more stable maintenance of reduction over time in casted patients. Additionally, a significantly greater proportion of casted patients maintained the reduction (MCS < 4 mm) at follow-up compared with splinted patients (n = 72 vs 19, P = .04), indicating initial immobilization with casting was associated with longer term stability of the ankle joint (Table 3).
Surgery Rates by Initial Immobilization Type.

Medial clear space measurement (6.0 mm) at ankle dislocation for a splinted patient.

Medial clear space measurement (2.9 mm) upon reduction for a splinted patient.

Medial clear space measurement (4.2 mm) at follow-up for a splinted patient.
Radiographic Outcomes (Medial Clear Space in mm). a

Abbreviation: MCS, medial clear space.
Differences between groups are reported as Hodges-Lehmann median differences for nonnormal data and mean differences for normally distributed data, both with 95% CIs. Mann-Whitney U tests were used for nonnormal comparisons and independent t tests for normally distributed comparisons.
There were no statistically significant differences in complication rates between casted and splinted groups, whether analyzed as overall complication percentages or by individual complication type, including pre- and postoperative skin issues, emergency department visits, or infections occurring pre- or postoperatively (Table 4). No cases of compartment syndrome occurred in either group. Five patients developed postoperative skin-related complications; none of the patients had diabetes or BMIs ≥40, and 2 were active smokers (with 1 patient in the cast group and 1 in the splint group). The 2 infections occurred postoperatively in nondiabetic, nonsmoking patients without BMIs ≥40. The skin-related complications included a fracture blister, eschar wound, and wounds with bloody or scant drainage. The wounds were lateral, mitigating concern that the wounds developed from medial applied pressure from molding the cast or splint.
Complication Rates by Initial Immobilization Type.

Discussion
This study found that initial cast immobilization in patients with unstable Weber B ankle fractures was associated with significantly smaller postreduction MCS and significantly smaller follow-up MCS (P < .01 for both), suggesting that casting may represent a more effective method of immobilization compared to splinting. Although immediate postreduction MCS measurements in both groups averaged within the acceptable <4-mm threshold, only the cast group maintained an average MCS below this threshold at follow-up. At our institution, the initial clinic follow-up visit for these patients is between 1 and 2 weeks from the date of injury. The change in MCS measurements from the initial reduction to follow-up was also significantly smaller in the cast group (P < .01), further supporting the finding that casting was associated with more stable maintenance of reduction than a splint over the course of 1-2 weeks.
Despite casting maintaining improved congruency of the ankle, surgical intervention rates did not differ significantly between groups (P = .34), suggesting that maintenance of reduction may not play an important role in surgical decision making. Recent data suggest that nonoperative treatment may be noninferior to surgery in patients with Weber B ankle fractures that maintain ankle congruency even in the presence of initial instability on external rotation stress radiographs; however, this practice has not been widely adopted at our institution.10 -12 This may be due to the fact that our institution has historically splinted more of these fractures and thus has found that ankle congruency was poorly maintained. This may also be due to the fact that when a shared decision-making conversation is had with the patient regarding operative and nonoperative management, patients are uneasy with the idea of risking further displacement with nonoperative management and thus choose to proceed with surgery. However, this type of data may encourage more nonoperative management in the future if the reduction can be maintained, especially for patients with significant comorbidities.
Recent data suggest that patients with initially gravity stress–positive unstable Weber B fractures may be treated weightbearing as tolerated, without increased MCS widening on follow-up weightbearing radiograph, and with outcomes equivalent to those without MCS widening.13,14 These findings call into question the importance of maintaining reduction while immobilized. However, ankle position may influence the radiographic appearance of stability. Because of the shape of the talus, MCS increases when the ankle is plantarflexed compared with neutral. Weightbearing radiographs are typically obtained with the ankle in a 90° position, whereas in a splint or cast the ankle may rest in a more plantarflexed position. This difference in positioning may lead to increased perceived stability on weightbearing radiographs compared with external rotation or gravity stress radiographs. Although this study did not evaluate the degree of plantarflexion within the cast or splint, at our institution ankles that are splinted in significant plantar flexion are called back to the emergency department for resplinting at the discretion of the attending surgeon. It is also possible that the increased rigidity of fiberglass casts better maintains the ankle in 90° of dorsiflexion, thereby limiting MCS widening. Figures 4 and 5 are examples of a short leg cast and short leg splint performed at our institution.

Short leg cast constructed with approximately 3-4 layers of 3M Fiberglass, extending from the tibial tubercle to the toes.

Short leg splint constructed with a posterior slab and a U-stirrup extending proximally to the level of the tibial tubercle and the posterior slab extending distally just past the toes. Ten to 12 layers of Gypsona plaster are used for both the posterior slab and U components of the splint. It is overwrapped with elastic bandage.
In patient populations at high risk for noncompliance or loss to follow-up, the ability of casting to maintain an appropriate reduction may have greater clinical importance. At-risk populations who cannot follow up may result in a loss of reduction, dislocation, and irreversible degenerative changes. This study demonstrates that casting holds the reduction without increased risk of complication, specifically soft tissue wounds, suggesting a superior treatment approach for vulnerable populations who struggle to access, or maintain access, to routine health care.
This is the first study to directly compare outcomes related to initial immobilization of unstable Weber B ankle fractures in nonbivalved casts vs splints. Stable Weber B fractures, as defined by no MCS widening on stress radiographs, are well established as nonoperative injuries, whereas unstable Weber B fractures with MCS widening have traditionally been more likely to require surgery. When analyses combine stable and unstable Weber B patients together, this obscures the clinical outcomes and surgical rate findings in the unstable Weber B patient subset, where the initial immobilization method may affect surgical planning. A previous meta-analysis that examined both stable and unstable Weber B fractures together reported lower complication and reoperation rates with nonoperative vs operative treatment. 15 However, because this study did not stratify patients by fracture stability, its findings do not capture the distinct treatment course of unstable Weber B fractures, which often require surgical fixation and may differ in optimal initial immobilization method. Our study explicitly isolates unstable Weber B injuries as the population of interest.
This study has several limitations. First, selection bias is introduced as the choice of initial immobilization was left to the discretion of the treating, on-call orthopaedic resident, so individual preferences or familiarity with splinting or casting may have influenced treatment selection. Additionally, subjective preference of the on-call attending surgeon may impact the choice of immobilization type, introducing further selection bias. Second, as a single-institution retrospective review, the generalizability is limited and larger multicenter studies may strengthen external validity; however, the study was conducted at a level 1 trauma center serving a large metropolitan catchment area with a diverse patient population. Finally, although the sample size allows meaningful comparisons, the study may still be underpowered to detect less common complications or differences in subgroups.
Strengths of the study include the long capture period of 8 years and the involvement of 6 fellowship-trained foot and ankle and trauma surgeons, each of whom trained at different institutions.
Conclusion
Initial immobilization with a cast in unstable Weber B ankle fractures appears to provide more stable radiographic alignment following reduction and throughout follow-up. Patients treated with casts were more likely to maintain acceptable alignment over time, indicating that casting supports a more durable reduction. Importantly, this improved stability was not associated with higher complication rates, even among patients traditionally considered higher risk, though the study may have been underpowered to detect a difference in safety profiles given the small sample size. These findings suggest that casting may offer a safe initial management option associated with greater protection against loss of reduction. For patients, this may translate to more reliable early outcomes without added morbidity. For providers, casting may represent a practical approach that may be particularly beneficial for individuals who face challenges with consistent follow-up. Further prospective, multicenter research is needed to refine and standardize immobilization protocols for unstable Weber B fractures.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114261438476 – Supplemental material for Impact of Initial Immobilization Method on Outcomes in Unstable Weber B Ankle Fractures: A Retrospective Cohort Study
Supplemental material, sj-pdf-1-fao-10.1177_24730114261438476 for Impact of Initial Immobilization Method on Outcomes in Unstable Weber B Ankle Fractures: A Retrospective Cohort Study by Isabella Rubin, Gianna Guarino, Meghan Lauzé, Antonio Lobao and Abhay Patel in Foot & Ankle Orthopaedics
Footnotes
Ethical Considerations
Ethical approval for this study was obtained from the UMass Chan Institutional Review Board (STUDY00002107).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Disclosure forms for all authors are available online.
Data Availability Statement
The data sets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.