
Abstract
Background:
In previous clinical studies of Achilles tendon (AT) ruptures, there are few reports measuring the AT length after conventional non-operative treatment without early functional rehabilitation. This study reviewed the outcomes of non-operative treatment for AT ruptures and assessed tendon length using magnetic resonance imaging (MRI).
Methods:
Patients with acute AT rupture who underwent non-operative treatment were included in this retrospective study. In our department, conventional non-operative treatment without early functional rehabilitation is used to avoid excessive tendon lengthening in patients with AT rupture. Patients wore a below-the-knee cast and performed non-weight-bearing walking for 4 weeks. Subsequently, the cast was removed, and an ankle-foot orthosis was applied for 4-6 weeks. The mean follow-up period was 28 months. Clinical outcomes were assessed using the Japanese Society for Surgery of the Foot (JSSF) ankle-hindfoot scale and the AT Total Rupture Score (ATRS). The tendon length and morphology were evaluated using MRI.
Results:
Sixty-four patients (42 men, 22 women; mean age, 44 years) with acute AT rupture underwent non-operative treatment. The mean JSSF score and ATRS were 97 and 91 points, respectively. Among 43 athletes, 36 (83.7%) returned to their pre-injury level of sports participation. Tendon re-rupture occurred in 2 of 64 patients (3.1%). T2-weighted MRI revealed fusiform-shaped tendon thickening and homogeneous low-signal changes in all patients. The mean AT length measured by MRI after treatment was 66.4 mm.
Conclusion:
Conventional non-operative treatment without early functional rehabilitation has a low re-rupture rate and favorable clinical outcomes, and MRI findings indicated good tendon healing in all patients. In our non-operative treatment, tendon lengthening increased up to 6 months post-injury. Overall, these results indicate that casting and non-weight-bearing for 4 weeks may represent a safe and effective treatment option associated with limited excessive tendon lengthening and re-rupture.
Level of Evidence:
Level IV, retrospective cohort study.

Introduction
Prior studies have reported that re-rupture rates for patients with Achilles tendon (AT) rupture are higher following non-operative treatment than operative treatment.1,2 However, several studies have shown that operative and non-operative treatment of acute AT rupture achieve equivalent re-rupture rates when the non-operative treatment protocol includes early functional rehabilitation.3,4 Yet, a recent study reported a higher number of re-ruptures in the nonoperative group, but it was not statistically significant. 5 Furthermore, a critical analysis of evidence suggests that true equivalence cannot be concluded and a clinically meaningful surgical benefit of lower re-rupture rate cannot be ruled out. 6 Current treatments for acute AT rupture involve early functional rehabilitation,3,4,7 but we believe caution is warranted when non-operative treatment is combined with early functional rehabilitation. 7 Hutchison et al 7 previously reported a re-rupture rate of 0.9% in 211 patients managed conservatively. Although early functional rehabilitation was used in the treatment protocol, these authors emphasized the importance of a strict physiotherapy protocol, patient compliance, and understanding of the injury. Thus, we believe that early functional rehabilitation administered by physicians or medical staff without expertise in conservative treatment may increase the risk of re-rupture and requires caution. More recent studies have reported that early functional rehabilitation provided no benefit in the clinical score or re-rupture rate when compared to immobilization in non-operative treatment of AT rupture.8,9 Therefore, the optimal rehabilitation protocol for the non-operative treatment of AT rupture remains controversial.
From the perspective of biologic healing, AT healing following immobilization with non-operative treatment corresponds to second-intention healing. 10 Tendon healing comprises inflammatory, proliferative, and remodeling phases.11,12 In the early healing phases, the tendon is histologically immature and mechanically weak; therefore, functional rehabilitation may cause AT lengthening.12,13 Ankle plantar flexion weakness following AT rupture is a serious complication and may result from AT lengthening.13,14 Furthermore, AT lengthening causes biomechanical adaptations that can negatively affect higher-demand patients. 15 From the perspective of preventing tendon lengthening in the early healing phase, early functional treatment may cause tendon lengthening.
A recent study using magnetic resonance imaging (MRI) reported a mean AT length of 42.1 mm. 16 As the average normal AT length is established, the degree of AT lengthening can be estimated by measuring the AT length during or after treatment. We believe that not only the re-rupture rate but also the extent of tendon lengthening should be evaluated; however, few studies have evaluated the AT length during and after treatment. Our non-operative treatment is based on a strict physiotherapy protocol. To compare the treatment outcomes of our conventional non-operative therapy with those reported in previous studies, it is necessary to evaluate clinical outcomes and measure the tendon length using MRI.
Therefore, in this study, we aimed to review the outcomes of conventional non-operative treatment without early functional rehabilitation for AT rupture and to evaluate the degree of tendon lengthening and tendon shape using MRI. The hypotheses of this study were as follows. First, the results of our conventional non-operative treatment would be favorable. Second, non-operative treatment without early functional rehabilitation would result in less tendon length than previously reported non-operative treatment with early functional rehabilitation.
Methods
Study Design and Population
All patients provided informed consent via an opt-out process with public notification and the opportunity to decline participation, and the study was approved by our institutional review board (receipt no. 2020-059-1). Between July 2002 and March 2020, 65 patients with acute AT rupture underwent conventional non-operative treatment without early functional rehabilitation in our department by a single physician. To prevent tendon lengthening in the early healing phase, our department performs non-operative treatment of acute AT rupture using cast immobilization and non-weight-bearing for 4 weeks.
The inclusion criteria were (1) interval from injury to the initial outpatient visit ≤1 week, (2) ultrasonographic findings showing no gaps in the ruptured tendon stumps when the ankle joint was in full plantar flexion, and (3) follow-up period >2 years. The exclusion criteria were (1) AT re-rupture and (2) use of quinolone or corticosteroid therapy for other illnesses.
Overview of the Non-operative Treatment Protocol
Outpatient treatment was provided to all eligible patients (Table 1). At the first visit, ultrasound examination confirmed that the tendon stumps were approximated and that the gap disappeared when the ankle was held at the maximal plantar flexion. Patients wore a below-the-knee cast and maintained non-weight-bearing walking for 4 weeks. During the first 2 weeks, the cast held the ankle in the maximal plantar flexion (Figure 1), after which it was adjusted to a 30° plantar flexion angle. After 4 weeks, the cast was removed, and an ankle-foot orthosis with several heel wedges (Figure 2) was applied. Partial weight-bearing walking and range-of-motion exercises were initiated, with 1 heel wedge removed every 1-2 weeks. Full weight-bearing walking and double heel-rise exercises were conducted at 7 weeks. The orthosis was removed at 8-10 weeks. When patients could perform double heel-rise exercises, they were allowed to jog and perform single-heel rise exercises. Return to sports was permitted when patients met the following criteria: (1) ability to perform 10 single-leg heel lifts on the affected side, (2) MRI showing fusiform-shaped thickening and homogeneous low-signal alterations of the AT on T2-weighted images, and (3) a calf circumference difference between the affected and unaffected legs of <1 cm.
Non-operative Treatment Protocol.


During the first 2 weeks, the patients wore a cast that held the ankle in the maximal plantar flexion position.

At 4 weeks, the cast has been removed and an ankle-foot orthosis with several heel wedges is used instead.
Clinical Evaluation
Subjective outcomes, including pain, functional deficits (walking and climbing stairs), and return to sports, were evaluated. Objective outcomes included ankle range of motion, ability to perform a single-heel rise, and calf circumference. To assess the function of the gastrocnemius–soleus-AT complex, patients were asked to perform 10 single-leg heel lifts on the affected side and were evaluated as either able or unable to complete the task. Clinical results were further evaluated using the Japanese Society for Surgery of the Foot (JSSF)17,18 ankle-hindfoot scale score and the AT Total Rupture Score (ATRS) at the final follow-up.19,20 The JSSF scale has demonstrated high validity and reliability in patients with foot and ankle disorders.17,18 The Japanese version of the ATRS was used, and 40 of 64 patients completed the ATRS questionnaire.
MRI
Fifty-two patients underwent MRI to evaluate tendon length, contour, and signal intensity at 3, 6, and 12 months post-treatment. Patients were positioned supine, with the ankles supported in a neutral position at 0° and the knees at a 0°. MRI of the ankle joint was performed using 1.5-tesla (T) and 3.0-T SIGNA HDxt (version 16; GE Healthcare) and 3.0-T Ingenia scanners (release 5.4; Philips Medical Systems). Axial and sagittal T1- and T2-weighted images (T1WI and T2WI) were obtained. A single observer measured the AT length, as previously described,16,21 and calculated as the number of slices between proximal and distal points of the AT multiplied by slice thickness on axial T1WI (Figure 3). The proximal point shows the most proximal slice that does not contain the soleus muscle. The distal point shows the most proximal slice in which the AT is attached to the calcaneus. 16 Interobserver reliability for tendon length measurement was previously reported with the intraclass correlation coefficient of 0.969, corresponding to an “almost perfect” level of agreement according to Landis and Koch.16,22
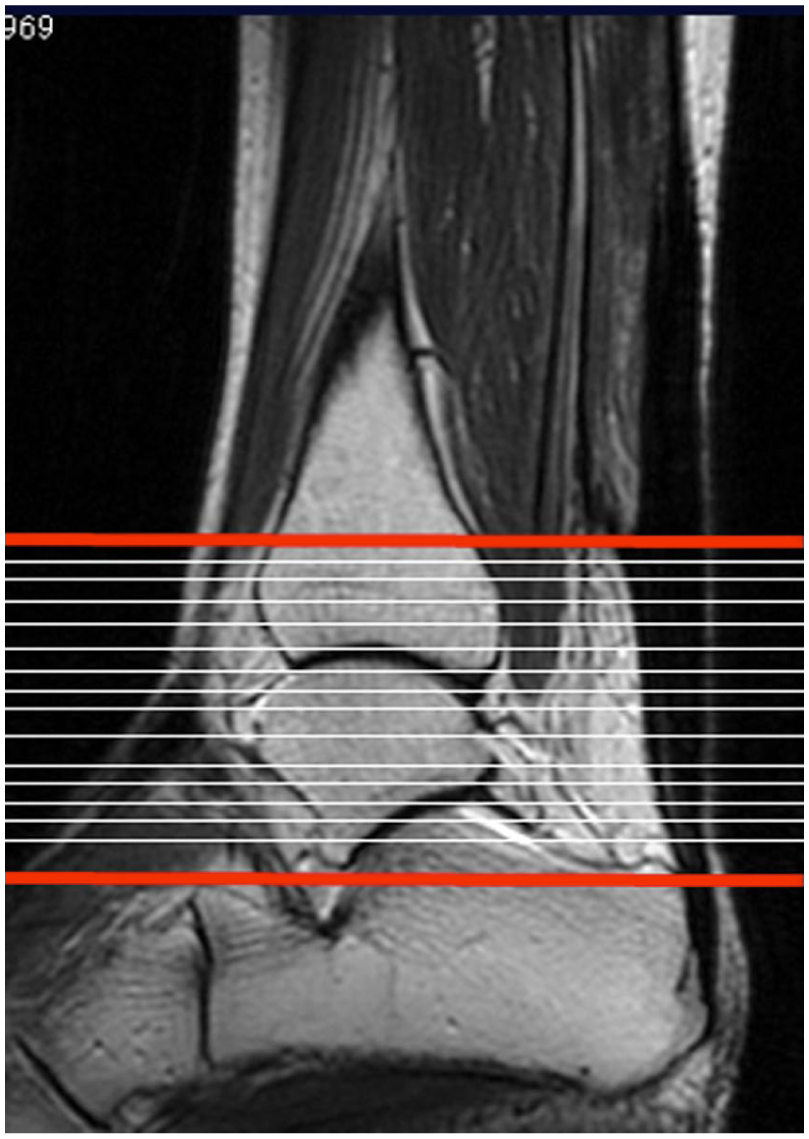
The Achilles tendon (AT) length was calculated as the number of slices between the proximal and distal points of the AT, multiplied by the thickness of 1 slice on axial T1-weighted images.
Statistical Analysis
AT lengths at 3, 6, and 12 months post-treatment are reported as mean ± SD and 95% CI. Repeated measures analysis of variance was used to assess the effects of time. If sphericity was violated, a Greenhouse-Geisser correction was applied. Analysis of variance revealed a significant time effect (P < .05) with partial η² = 0.095 (small-medium). Post hoc comparisons (3 vs 6, 6 vs 12, and 3 vs 12 months) were conducted using paired t tests with Bonferroni correction, and the Cohen d was reported for effect sizes. Analyses were performed using R (version 4.4.0; R Foundation for Statistical Computing) with the “ez” (4.4-0), “emmeans” (1.11.2), and “effectsize” (0.8.6) packages.
Intraobserver and interobserver reliability were evaluated for AT length measurements. Two foot and ankle orthopaedic surgeons independently measured AT length on 20 randomly selected MR images, performing 2 measurements each with a 4-week interval. Intraclass correlation coefficients were calculated to assess intraobserver and interobserver reliability using SPSS software (version 25; IBM Corp). Postoperative clinical scores and tendon lengths were compared between the athlete and non-athlete groups using the Mann-Whitney U test with JMP software (version 18; SAS Institute Inc).
Results
Participant Selection and Characteristics
One patient (1 foot) was lost to follow-up because she could not be contacted (Figure 4). The remaining 64 patients (64 feet) included 42 men and 22 women, with a mean age of 44 years (range, 17-82). The cohort included 43 athletes (9 badminton players, 9 basketball players, 7 volleyball players, 7 tennis players, 4 kendo athletes, and 7 others). Patients were followed for a mean of 28 (range, 24-40) months.

Flow diagram of participants.
Clinical Results
At the final follow-up, no patients reported difficulty walking or climbing stairs. All patients could perform a double-limb heel rise at a mean of 3 months (range, 2-4 months), and all except 3 patients could perform a single-limb heel rise at a mean of 5.7 months (range, 3-9). Three patients could not perform a single-limb heel rise at the final follow-up. The mean difference in circumference between affected and unaffected calves was 0.9 (range, 0-4) cm. Regarding ankle range of motion, increased dorsiflexion of the involved ankle compared with the uninvolved ankle was observed in 3 patients. No restrictions in dorsiflexion or plantar flexion were identified in any patient.
The mean JSSF score and ATRS were 97 and 91 points, respectively. In post hoc exploratory analysis, the mean JSSF score of athletes and non-athletes were 99 and 96 points, respectively. The mean ATRS of athletes and non-athletes were 94 and 87 points, respectively. Both JSSF scores (P = .035) and ATRS (P = .001) were significantly higher in the athletes group. Among the 43 athletes, 36 (83.7%) returned to sports participation between 5 months and 12 months post-injury. The remaining 7 athletes did not return to sports because of a fear of re-rupture.
Tendon re-rupture occurred in 2 of 64 patients (3.1%), both of whom were athletes. One patient experienced re-rupture after returning to badminton 4 months post-injury and underwent surgery at his request; he is currently doing well. The other patient re-ruptured after a fall down the stairs, was treated conservatively again, and returned to playing football 8 months after re-injury. No other complications, including deep vein thrombosis, were observed.
MRI Findings
T2-weighted MRI showed fusiform-shaped tendon thickening with diffuse high-signal alterations at 3 months post-injury (Figure 5A). Longitudinal high-intensity bands were observed throughout the tendons. By 6 months, all patients showed fusiform-shaped tendon thickening with homogeneous low-signal alterations (Figure 5B). In 1 patient with tendon re-rupture, local high-signal alterations were observed 3.5 months post-injury (Figure 6); this patient returned to badminton at 4 months and experienced tendon re-rupture.

(A) T2-weighted magnetic resonance imaging (MRI) of the tendon at 3 months after injury: T2-weighted MRI shows fusiform-shaped tendon thickening with diffuse high-signal alteration at 3 months after the injury. Longitudinal high-intensity bands (white arrow) can be observed throughout the tendons. (B) T2-weighted MRI of the tendon at 6 months after injury; T2-weighted MRI shows fusiform-shaped tendon thickening; a homogeneous low-signal alteration of the tendons is visible 6 months after the injury.

In a patient with tendon re-rupture, fusiform-shaped tendon thickening and local high-signal alterations (white arrow) of the tendon substance are observed at 3.5 months after injury.
The intraobserver intraclass correlation coefficients for the 2 examiners were 0.963 and 0.974. The interobserver intraclass correlation coefficients for the first and second measurements were 0.972 and 0.962, respectively. According to the system of Landis and Koch, these values corresponded to an almost perfect level of agreement. 22
The mean AT length measured by MRI after treatment was 66.4 (range, 24-105) mm. Mean AT lengths at 3, 6, and 12 months post-treatment were 63.3 ± 16.5 mm (95% CI: 58.7-67.9), 65.9 ± 18.4 mm (95% CI: 60.7-71.0), and 66.4 ± 19.1 mm (95% CI: 61.1-71.7), respectively (Table 2). Significant differences were observed between 3 and 12 months (P = .0087, d = −0.343) and between 3 and 6 months (P = .0365, d = −0.366); however, with the numbers available, no significant difference could be detected between 6 and 12 months (P = 1.000, d = −0.095) (Table 3). The mean AT length in athletes and non-athletes were 65.8 and 67.0 mm, respectively. With the numbers available, no statistically significant difference in tendon length could be detected between the groups (P = .830).
Achilles Tendon Length on MRI at 3, 6, and 12 Months After Injury

Comparison of the Achilles Tendon Length at Each Time Point

Discussion
The optimal rehabilitation protocol for the non-operative treatment of AT rupture remains controversial.3,4,7,8,9 We believe that maintaining tendon length during the inflammatory and proliferative phases is critical, particularly in patients undergoing non-operative treatment. To minimize tendon lengthening during the early healing phase, our department performs non-operative treatment of acute AT rupture using cast immobilization and non-weight-bearing for 4 weeks, corresponding to the inflammatory and initial proliferative phases of AT healing.
Here, conventional non-operative treatment without early functional rehabilitation has a low re-rupture rate (3.1%). Previous meta-analyses and systematic reviews have reported re-rupture rates in operative treatment groups of 3.5% and 3.6%, respectively.1,2 Thus, the re-rupture rate in our study is similar to that of previously reported surgical treatments. Furthermore, the JSSF scores and ATRS were 97 and 91 points, respectively, and MRI findings indicated good tendon healing in all patients. Based on these clinical and MRI findings, casting and non-weight-bearing for 4 weeks is an effective treatment option, supporting our first hypothesis.
We investigated the AT length over time during treatment using MRI. Significant differences were observed between 3 and 12 months and between 3 and 6 months, whereas no significant differences were found between 6 and 12 months. This indicates that non-operative treatment allows tendon lengthening for up to 6 months post-injury. Therefore, during conservative treatment, careful attention must be paid to tendon lengthening during the first 6 months.
The mean normal AT length is a useful value to assess tendon lengthening in various clinical studies of AT rupture. 16 A previous study investigating the AT lengths using MRI reported that the mean length of ruptured ATs treated non-surgically with early functional rehabilitation was 87.9 mm. 23 The mean AT length in the present study was 66.4 mm, which was 21.5 mm shorter than that reported for non-surgical treatments combined with early functional rehabilitation. Hence, our method was associated with substantially less tendon lengthening than non-operative treatment combined with early functional rehabilitation, a finding consistent with our second hypothesis.
Recent studies have reported a relationship between the extent of AT lengthening and clinical outcomes following operative treatment. Okoroha et al 24 measured AT lengthening, and all 18 patients had significant tendon lengthening after surgery, with a mean of 15.9 mm. The mean ATRS of the patients with accelerated rehabilitation was 85.4 points. Furthermore, Aufwerber et al 25 reported that mean AT elongation at 1 year was 17.3 mm for the early functional mobilization group and 16.7 mm for the standard treatment group following AT rupture repair. The ATRS were 79.6 and 78.9 points, respectively. Conversely, Svensson et al 14 reported that soleus tendon lengthening of 37.9 mm was associated with persistent functional loss following AT rupture. These findings indicate that the extent of AT lengthening is related to clinical outcomes; however, acceptable values of AT lengthening have not been established.
A recent study reported a mean AT length of 42.1 mm in 100 asymptomatic patients. 16 In the present study, the mean AT length was 66.4 mm, representing a mean increase of 24.3 mm. Tendon lengthening in the present study was greater than that reported in previous surgical treatments.21,24,25 However, because our present study is not a comparative one, caution is required when comparing our results with those of previously reported surgical treatments. We selected a cohort where the tendon stumps contact at maximal plantar flexion of the ankle joint. This selection criterion likely represents a more favorable biological subgroup. Thus, direct comparisons of tendon elongation magnitude or clinical outcomes should be interpreted with caution.
The observation of an AT that is thickened and fusiform-shaped with diffuse high-signal changes on T2WI indicates that the tendon contains dense collagen fibers with fibroblasts and vascularization, reflecting good tendon healing. 26 In contrast, if T2WI reveals an AT with focal high-signal changes at the rupture site, as in our re-rupture case (Figure 6), tendon healing is delayed. In the present study, diffuse high-intensity signal alterations at 3 months resolved over time. In one patient with tendon re-rupture, focal high-intensity signal changes at the rupture site were observed. Therefore, MRI findings are important when determining readiness for athletes to return to sports.
This study has certain limitations. Its retrospective design may have introduced bias. However, our study was conducted according to a well-established protocol, and it included a large number of participants, many of whom were athletes. Furthermore, using MRI to measure the AT length at different time points is a strength of this study. A randomized controlled trial of surgically repaired AT ruptures with a similar design has been reported 27 ; however, we evaluated non-operative treatment and therefore have independent value. Additionally, the acceptable values of AT lengthening in a clinical setting could not be determined. The observed mean difference in AT length from 3 to 12 months was approximately 3 mm, and its clinical relevance is unclear. Further studies investigating the relationship between AT lengthening and clinical outcomes are required. Furthermore, substantial individual variation in normal AT length makes it difficult to estimate the degree of tendon lengthening when measuring individual tendon lengths. Consequently, we were unable to categorize participants according to low or high lengthening and compare outcomes between these subgroups. We also did not perform isokinetic testing to assess muscle strength. Instead, we investigated double-limb heel rise, standing single-limb heel rise while standing, and calf circumference. Furthermore, 3 patients (4.7%) were unable to perform a single-limb heel rise at final follow-up, indicating that a minority of patients may experience persistent functional deficits despite otherwise favorable aggregate clinical scores. Finally, we used the Japanese version of the ATRS, and although the validity and reliability of the English and Turkish versions have been demonstrated,19,20 the Japanese version has not yet been validated.
Conclusion
Conventional non-operative treatment without early functional rehabilitation has a low re-rupture rate and favorable clinical outcomes, and MRI findings indicated good tendon healing in all patients. Furthermore, the present study has shown the tendon lengthening to increase until 6 months post-injury under this non-operative protocol. Overall, these results suggest that casting and non-weight-bearing for 4 weeks may represent a safe and effective treatment option associated with limited excessive tendon lengthening and re-rupture.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114261436395 – Supplemental material for Non-operative Treatment for Acute Achilles Tendon Rupture: Evaluation of Clinical Results and Tendon Lengthening on Magnetic Resonance Imaging
Supplemental material, sj-pdf-1-fao-10.1177_24730114261436395 for Non-operative Treatment for Acute Achilles Tendon Rupture: Evaluation of Clinical Results and Tendon Lengthening on Magnetic Resonance Imaging by Toshito Yasuda, Kosho Togei, Ken Tanaka, Masatoshi Takashima, Hiroaki Shima and Shuhei Otsuki in Foot & Ankle Orthopaedics
Footnotes
Acknowledgements
The authors express their deep gratitude to Professor Yuri Ito and Dr. Tatsuhiko Matsumoto of the Department of Medical Statistics, Research & Development Center, Osaka Medical and Pharmaceutical University, for their invaluable assistance with the statistical analyses.
ORCID iDs
Ethical Considerations
All patients provided informed consent to participate, and the study was approved by our institutional review board (receipt no. 2020-059-1).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Disclosure forms for all authors are available online.
Data Availability Statement
In accordance with institutional and ethical requirements, data are available upon reasonable request from the corresponding author.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.