
Abstract
Background:
Controversy exists regarding mandatory hindfoot varus in Müller-Weiss disease (MWD).
Methods:
This retrospective cohort study examined weightbearing computed tomography (WBCT) in 22 feet with MWD. Measurements included hindfoot moment arm (HMA), middle facet subluxation in coronal (MFSC) and sagittal (MFSS) planes, posterior facet uncoverage, and angles between inferior and superior talar surfaces (inftal-suptal) at 33%, 50%, and 67% of the way moving from anterior to posterior along the posterior facet.
Results:
From the cohort consisting of 14 patients (22 feet, mean age 51.14 ± 13.90 years), based on a neutral zero HMA, 10 feet were designated as varus-offset and 12 as valgus-offset. Mean MFSC in valgus-offset (49.3 ± 6.3%) is significantly greater than in varus-offset feet (28.2 ± 6.1%) (P = .022). Greater MFSS and posterior facet uncoverage in valgus-offset feet are not statistically significant. Based on inftal-suptal angles, 2 groups of talar configurations are identified, each with increased predisposition towards either varus or valgus offset. In talus configurations with inftal-suptal angles open laterally at all 3 levels, the predominant heel offset is varus (89%), whereas in talus configurations featuring an inftal-suptal angle open medially, the predominant heel offset is valgus (85%) (P = .002). As HMA changes from varus to valgus, inftal-suptal angles change from open laterally to open medially at all 3 levels, reaching greatest significance at the 67% mark (P < .001).
Conclusion:
To our knowledge, this is the largest WBCT study of MWD to date. In these patients, we identified significantly greater MFSC in valgus-offset feet and different talus configurations, which may explain the more frequent 55% incidence of valgus offset. Because universal heel varus is not always the rule, caution is advised in advocating lateral displacement calcaneal osteotomy for all MWD feet.
Level of Evidence:
Level IV, retrospective cohort study.

Keywords
Introduction
Müller-Weiss disease (MWD) is a condition of undetermined etiology that primarily affects the navicular bone with secondary involvement of the perinavicular joints. Although considered rare, it is becoming increasingly recognised worldwide.1 -3 It frequently manifests with chronic midfoot pain and can lead to progressive deformity if left untreated. Maceira and Rochera 4 coined the term “paradoxical pes planus varus” to characterize the medial arch collapse sometimes encountered in conjunction with hindfoot varus, particularly in late stages of the disease. They postulated that, as the medial pole of the navicular subluxes medially when its lateral part undergoes increasing compression and eventually fragmentation, the talus rotates laterally, thereby causing the calcaneus to perforce shift medially since both talus and calcaneus form part of the coxa pedis. As a result, the notion of mandatory heel varus persists in the literature, even though the heel has been reported in both neutral and valgus alignment in patients with MWD.5 -9
In a study comprising 68 MWD feet, Wong-Chung et al 10 used 2-dimensional conventional hindfoot alignment view radiographs, as described by Saltzman and El-Khoury, 11 to determine hindfoot position. Varus heel offset was present in only 33%. The combination of flatfoot and heel varus, which would match the description of “pes planus varus,” was present in just 26%, the commonest combination being of heel valgus and medial arch collapse at 56%.
Three-dimensional weightbearing computed tomography (WBCT) has recently gained acceptance as a more accurate tool for assessment of complex foot and ankle deformities. 12 Compared to progressive collapsing foot deformity (PCFD), its application in MWD has been limited.13,14 The present study aimed to use WBCT imaging to ascertain the more frequent patterns of hindfoot alignment and overall multiplanar deformity in MWD. In addition, it sought to determine possible deformity pattern combinations that could potentially predispose the hindfoot to be positioned either in varus or valgus malalignment. Our hypothesis was that, by enabling a better understanding of the multiplanar deformities, WBCT would demonstrate valgus offset to be the most common presentation of hindfoot alignment in MWD and provide a biomechanical explanation for valgus heel disposition when present.
Methods
In this retrospective dual-center study conducted with institutional review board approval, WBCT was performed on 22 consecutive feet with MWD between February 2022 and May 2024, in 8 women and 6 men aged 21-73 (mean, 51.14 ± 13.90) years, using a cone-beam computed tomography scanner (PedCAT or HiRise; CurveBeam AI). The main inclusion criterion for diagnosis of MWD was radiologic compression of the lateral portion of the navicular with a resultant comma- or hourglass-shaped bone and secondary asymmetrical arthritis of the talonavicular joint (TNJ). Excluded were concentric TNJ arthritis, residual clubfoot, Charcot neuropathy and systemic arthritis through appropriate clinical evaluation, blood investigations, and nerve studies. PCFD, in which the talus rotates medially instead of laterally with respect to the navicular, was not included. Stress fractures were excluded based on location, configuration, and direction of the fracture line.15 -17 Hindfoot varus was not considered a prerequisite because this is exactly what the study sets out to verify. Disease was bilateral in 8 and unilateral in 6 cases. Patients were instructed to weight-bear in a natural standing position with feet pointing forward and apart at shoulder width, and to distribute weight evenly between the 2 lower limbs.
Two fellowship-trained foot and ankle orthopaedic surgeons at 2 different centers performed multiple manual measurements using CubeVue software (Curvebeam AI), and each repeated the measurements 8 weeks apart (Table 1). In the coronal plane, hindfoot moment arm (HMA) was measured as the mediolateral distance between the distal extension of the longitudinal axis of the tibia at ground level and the most inferior voxel of the calcaneal tuberosity as verified in all 3 planes (Figure 1, A-F). 18 To improve accuracy of localization of the midpoint of the tibia, the slab tools function in CubeVue is useful for visualizing its widest diameter (Figure 1B). 19 WBCT-derived HMA has been shown to be a reliable and reproducible metric for assessing hindfoot alignment.20 -22 Based on a neutral zero HMA, feet with negative HMA values were designated as varus-offset and feet with positive values as valgus-offset.
Weightbearing Computed Tomographic Measurements. a
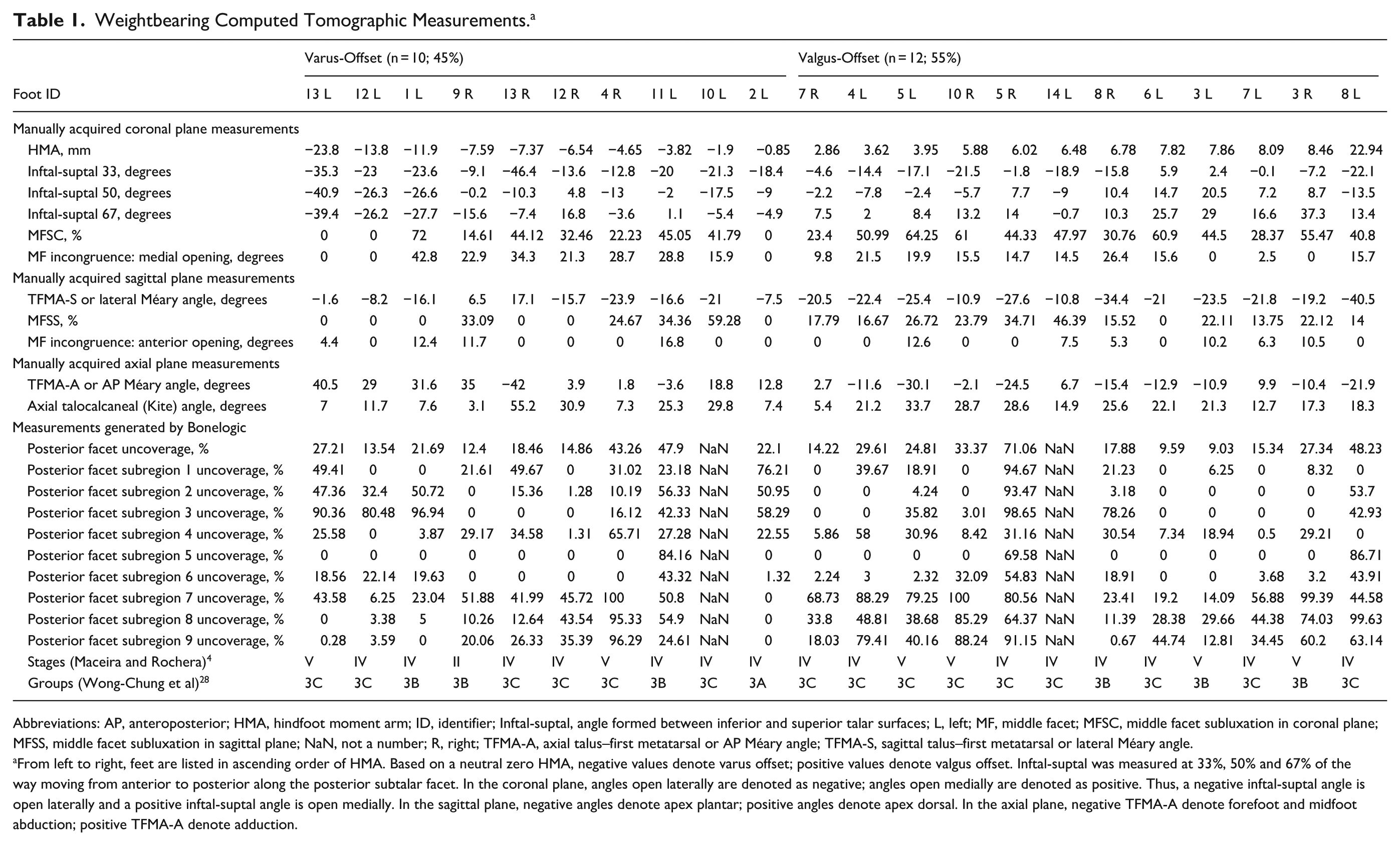
Abbreviations: AP, anteroposterior; HMA, hindfoot moment arm; ID, identifier; Inftal-suptal, angle formed between inferior and superior talar surfaces; L, left; MF, middle facet; MFSC, middle facet subluxation in coronal plane; MFSS, middle facet subluxation in sagittal plane; NaN, not a number; R, right; TFMA-A, axial talus–first metatarsal or AP Méary angle; TFMA-S, sagittal talus–first metatarsal or lateral Méary angle.
From left to right, feet are listed in ascending order of HMA. Based on a neutral zero HMA, negative values denote varus offset; positive values denote valgus offset. Inftal-suptal was measured at 33%, 50% and 67% of the way moving from anterior to posterior along the posterior subtalar facet. In the coronal plane, angles open laterally are denoted as negative; angles open medially are denoted as positive. Thus, a negative inftal-suptal angle is open laterally and a positive inftal-suptal angle is open medially. In the sagittal plane, negative angles denote apex plantar; positive angles denote apex dorsal. In the axial plane, negative TFMA-A denote forefoot and midfoot abduction; positive TFMA-A denote adduction.

(A-F) Measurement of hindfoot moment arm. (A) In the coronal plane, the midpoint of the tibia is marked at 5 and 10 cm above the ankle joint surface. (B) Accuracy is enhanced by using the slab tools function in CubeVue to visualize the widest diameter of the tibia. (C-E) The most inferior voxel of the calcaneus is confirmed on all planes. (F) Hindfoot moment arm is the distance between the most plantar weightbearing point of the calcaneus and the distal extension of the tibial anatomical axis at ground level (green line with tick marks). (G-J) Measurement of inftal-suptal angles at (G) 33%, (H) 50% and (I) 67% of the way moving from anterior to posterior along the posterior facet, as denoted by light-blue tick marks. The coronal plane image is synchronized with the sagittal view by aligning the crosshairs formed by the vertical blue line and horizontal red line with the appropriate tick mark. The inftal-suptal angle is the angle between the superior and inferior surfaces of the talus. (J) Diagram illustrating varus and valgus inftal-suptal angles. Inftal-suptal angle (
Also in the coronal plane, the angle between the inferior and superior talar surfaces (inftal-suptal) was measured at 3 different levels along the posterior facet of the subtalar joint as described by Probasco et al. 23 Instead of 25%, 50% and 75% from posterior to anterior, we selected 33%, 50% and 67%, moving from anterior to posterior along the posterior subtalar facet, to match the “one-third marks” measurement tool available on the software (Figure 1, G-I). By convention, a negative inftal-suptal angle (open laterally) indicates varus orientation of the heel, and a positive value (open medially) indicates valgus orientation of the heel (Figure 1J). 23
Middle facet subluxation in the coronal plane (MFSC) was measured, as described by de Cesar Netto et al.24,25 Percentage subluxation equals [lateral subluxation (mm) ÷ width of talar middle facet joint surface (mm)] × 100 (Figure 1, K-L). MFSC of >17.9% has been shown to be a strong predictor of symptomatic PCFD, with 100% specificity and 96.7% sensitivity. 24 In addition, mediolateral incongruence (medial opening) of the middle facet was measured (Figure 1M).
On sagittal plane images, sagittal talus–first metatarsal (TFMA-S) angle, percentage middle facet subluxation (MFSS), and anteroposterior incongruence (anterior opening) of the middle facet were measured (Figure 1, N-P).
On axial plane images, the axial talus–first metatarsal (TFMA-A) and axial talocalcaneal (Kite) angles were determined (Figure 1, Q-U).
Additionally, a fully automatic segmentation software (Bonelogic 2 Ortho Foot and Ankle, Disior; Paragon 28) calculated 3D distance and coverage mapping to evaluate coverage of the 9 subregions of the posterior subtalar facet.26,27 Subchondral bone-to-bone distances of 1 to 4 mm indicate expected normal joint contact, whereas inter-bone distances greater than 4 mm signify joint uncoverage and inter-bone distances of under 1 mm denote joint space narrowing or impingement.
All feet were classified into stages according to TFMA-S angle as described by Maceira and Rochera 4 and into groups according to the affected midfoot joints as described by Wong-Chung et al. 28
Statistical analysis was carried out using IBM SPSS Statistics for Windows, version 29. All data were tested for normality using the Shapiro-Wilk test plus visual evaluation of histogram. All data were found to be normally distributed, with the Shapiro-Wilk test being non-significant. To account for clustering of bilateral and unilateral cases, continuous variables were assessed with mixed model analysis where independent and bilateral measurements were identified as one factor along with varus/valgus directions as a second factor. Estimated marginal means, SE, 95% CIs were reported with effect size as represented by Cohen d and P values in relation to varus and valgus directions. Bonferroni post hoc testing was carried out for all comparisons to account for repeated measures and adjusted P values reported. Frequency of varus and valgus offset between 2 groups with different talar configurations was compared using χ2 analysis. Statistical significance was set at P <.05. Intraclass correlation coefficients (ICCs) were obtained to evaluate consistency of measurements. Based on a 95% confident interval, ICC values of >0.9, between 0.75 and 0.9, between 0.5 and 0.75, and <0.5 indicate excellent, good, moderate and poor reliability, respectively.
Results
Based on a neutral zero HMA, 12 (55%) feet were valgus-offset and 10 (45%) were varus-offset. At the middle facet, subluxation occurred laterally in the coronal plane in all valgus-offset feet and posteriorly in the sagittal plane in all except 1. In the 10 varus-offset feet, no coronal plane subluxation occurred in 3 and no sagittal plane subluxation in 6. In both varus-offset and valgus-offset feet, subluxation always took place laterally and posteriorly, and never medially or anteriorly.
In the coronal plane, mean MFSC in valgus-offset feet (49.3 ± 6.3%) was significantly greater than in varus-offset feet (28.2 ± 6.1%) (P = .022) (Figure 2A). Effect size, as measured by Cohen d, was 0.99, indicating a large effect. Mediolateral incongruence, by which the middle facet opens medially, was greater in varus-offset (20.0 ± 3.9 degrees) than in valgus-offset feet (14.7 ± 4.0 degrees) (P = .338) (Table 2).

Middle facet. (A) In the coronal plane, percentage middle facet subluxation increases significantly as hindfoot moment arm (HMA) (black solid line) changes from varus (negative values) to valgus (positive values). (B) Similarly, although not significantly, subluxation in the sagittal plane increases as HMA changes from varus to valgus.
Middle Facet Subluxation and Inftal-Suptal Angles in Varus-Offset and Valgus-Offset Feet. a

Abbreviations: HMA, hindfoot moment arm; Inftal-suptal, angle formed between inferior and superior talar surfaces; MFSC, middle facet subluxation in coronal plane; MFSS, middle facet subluxation in sagittal plane.
Inftal-suptal was measured at 33%, 50% and 67% of the way, moving from anterior to posterior along the posterior subtalar facet.
Using neutral zero HMA as reference.
Boldface indicates significance (P < .05).
In the sagittal plane, mean MFSS was greater in valgus-offset (22.0 ± 5.7%) than in varus-offset feet (15.4 ± 5.5%) (P = .393) (Figure 2B). Anteroposterior incongruence, by which the middle facet opens anteriorly, was not different between varus- and valgus-offset feet (Table 2).
Although clearly noticeable in 1 varus-offset (Foot 4R) and 2 valgus-offset (4L, 10R) (Figure 3A), superior displacement at either end of the posterior subtalar facet proved difficult to reliably measure on CubeVue in most cases. Instead, 3D distance and coverage mapping using Bonelogic demonstrated greatest uncoverage of the 3 posterior subregions of the posterior facet (Figure 3B), with posterior-medial subregion 7 attaining maximum uncoverage (52%) followed by posterior-middle subregion 8 (39%) and posterior-lateral subregion 9 (37%). The middle segments remained well covered, especially the middle-middle subregion (12%). In the lateral region, the middle-lateral subregion 6 stayed relatively well-covered (13%) compared to the posterior-lateral (37%) and anterior-lateral (32%) subregions (Figure 3C).

Posterior subtalar facet. (A) Superior displacement of the calcaneus at both anterior (curved arrow) and posterior (straight arrow) ends clearly evident in Foot 10R. (B) In the same foot, Bonelogic demonstrates greatest uncoverage of the 3 posterior subregions of the posterior facet (purple). (C) Overall percentage uncoverage of the 9 subregions of the posterior facet mapped out over the superior surface of a talus bone. Greatest uncoverage occurs at posterior subregions 7, 8 and 9 (red boxes). (D) Uncoverage of posterior-medial subregion 7, posterior-middle subregion 8 and posterior-lateral subregion 9 of the posterior facet of the subtalar joint increases as hindfoot moment arm (HMA) (black solid line) changes from varus to valgus.
Uncoverage of the 3 posterior subregions increased as HMA changed from varus to valgus offset (Figure 3D). Overall uncoverage of the entire posterior subtalar facet increased from 24.8 ± 5.6% in varus-offset to 27.5 ± 5% in valgus-offset feet (P = 0.724; Cohen d = 0.17; 95% CI = 0.7-1). By subregion, uncoverage decreased at subregions 1 to 4 as HMA changes from varus to valgus, while increasing at subregions 5 to 9, especially at posterior-medial subregion 7 and posterior-middle subregion 8. However, none of these increases were statistically significant.
Placing the feet in order from varus to valgus, inftal-suptal angles change from negative (open laterally) to positive (open medially) (Figure 4). These changes increase, moving from anteroinferior to posterosuperior along the posterior facet, reaching maximal values at the 67% level. Differences in inftal-suptal angles between valgus-offset and varus-offset feet are statistically significant at all 3 levels, most notably at the 67% level (P < .001) (Table 2).

Inftal-suptal angles progressively change from negative (open laterally) to positive (open medially) as hindfoot moment arm (HMA) (black solid line) changes from varus to valgus. Significance of these changes increase, moving upwards from anterior to posterior at 33%, 50% and 67% along the posterior facet.
Of 9 feet with varus inftal-suptal angles at all 3 levels, 33%, 50% and 67% of the way along the posterior facet (group 1, configuration A), the prevalent HMA offset was varus at 89% with only 11% offset in valgus. In group 2 (13 feet), which featured valgus inftal-suptal angles at either all 3 levels (configuration B), at the 50% and 67% marks (configuration C) or at the 67% mark only (configuration D), the prevalent HMA offset was valgus at 85% with 15% offset in varus (P = .002) (Table 3).
Relationship Between Talus Configuration and Heel Offset. a

At either the 33%, 50% or 67% mark along the posterior facet, configuration of the talus is designated as varus-favorable when the inftal-suptal angle is open laterally at that level. Conversely, configuration of the talus is designated as valgus-favorable, when the inftal-suptal is open medially at that level. Thus, configuration A is characterized by varus 33-50-67, meaning a varus-favorable configuration at all 3 levels.
The TFMA-A angle measures the degree of mid- and forefoot abduction. In 11 feet, the longitudinal axis of the first metatarsal passed lateral to that of the talus, indicating abduction and denoted as negative (Table 1). In the other 11 feet, the first metatarsal axis passed medial to that of the talus, indicating adduction and denoted as positive. Acknowledging that abduction takes place by varying degrees of mediolateral subluxation and angulation at various levels across the talonavicular, naviculocuneiform and tarsometatarsal joints, by using the first metatarsal distally to reference the position of the talus proximally, TFMA-A applied in reverse may indirectly serve as an approximate overall index of axial rotation of the talus. Thus, as talar rotation changes from medial (TFMA-A negative) to lateral (TFMA-A positive), mean Kite angle decreases from 26.7 ± 3.5 degrees to 20.5 ± 3.2 degrees (P = .177) (Cohen d = .659; 0.2 to 1.5) (Figure 5). Kite angle ranges from 3.1 to 55.2 (mean 19.77 ± 11.98 degrees). Fourteen (64%) feet have Kite angle of less than 25 degrees, 7 (32%) between 25 and 40 degrees (normal range), and 1 greater than 40 degrees.

Kite anteroposterior talocalcaneal angle decreases as talar rotation changes from medial to lateral. The axial talus–first metatarsal (TFMA-A) or anteroposterior Méary angle is used as a reverse index of talar rotation. In Foot 5L (inset top left) with forefoot abduction (TFMA-A negative), the longitudinal axis of the first metatarsal passes lateral to the longitudinal axis of the talus (red solid straight line). In Foot 13L (inset top right) with forefoot adduction (TFMA-A positive), the longitudinal axis of the first metatarsal passes medial to the longitudinal axis of the talus (green solid straight line). Moving from forefoot abduction (TFMA-A negative) to forefoot adduction (TFMA-A positive) is denoted by dotted black arrow pointing from left to right. As talar rotation changes from medial (referenced by solid red line) to lateral (referenced by solid green line), the Kite angle decreases.
There were 4 feet with advanced Maceira stage V disease in the valgus-offset group compared with 2 in the varus-offset group (P = .646). Similarly, 9 of the valgus-offset feet were classed as group 3C according to Wong-Chung et al, compared with 6 in the varus-offset group (P = .652). Otherwise, stage IV disease and group 3B were approximately equal in both groups.
Discussion
Based on a neutral zero HMA, the present WBCT study demonstrates a 55% incidence of valgus-offset and 45% incidence of varus-offset feet in MWD. Middle facet subluxation in the coronal plane (MFSC) is significantly greater in valgus-offset than in varus-offset feet (P = .022). Significant differences in inftal-suptal angles exist at all levels between valgus-offset and varus-offset feet. In a talus configuration with varus inftal-suptal angles at all 3 levels along the posterior facet, prevalent offset is varus at 89%, whereas in talus configurations featuring a valgus inftal-suptal angle, prevalent offset is valgus at 85% (P = .002) (Table 3).
It contributes towards settling the ongoing controversy regarding mandatory heel varus in MWD, whereby its proponents maintain that hindfoot varus constitutes a hallmark and prerequisite of the disease14,29 -32 whereas others have proposed that the heel is not always in varus based on clinical examination and plain weightbearing radiographs.5 -10
Additionally, this study provides 2 possible explanations as to why the hindfoot is not always varus-offset but instead valgus-offset in MWD. Firstly, greater degrees of lateral displacement and rotation take place in valgus-offset than in varus-offset feet, mostly at the middle facet of the subtalar joint. Secondly, different configurations of talar anatomy may predispose and favor the hindfoot to be positioned towards either varus or valgus offset.
The literature contains very few studies on the use of WBCT in MWD, likely due to rarity of the condition and limited access to WBCT. Welck et al 13 found WBCT useful for estimating the size of calcaneal osteotomy required to correct varus hindfoot malalignment in 3 patients. Using WBCT, Li et al 14 compared 17 feet with MWD against 10 feet with PCFD and 10 normal feet. MWD, PCFD and normal patients demonstrated average HMA values of −3.44, 15.75 and 3.19 mm, and MFSC of 14%, 45% and 23%, respectively, leading the authors to conclude that hindfoot varus is a typical feature of MWD. In MWD feet, MFSC was said by those authors to have taken place medially, in a direction opposite to that of peritalar subluxation in PCFD. In the present study, MFSC always occurred laterally and never medially.
Maceira and Rochera postulated that the calcaneus, being part of the coxa pedis, must automatically move into varus when the talar head lateralizes towards the center of the foot, just like the calcaneus shifts into valgus when the talar head displaces medially in PCFD. 4 This proposed mechanism to explain mandatory heel varus in MWD assumes that the talus and calcaneus move together as one connected block and the Kite talocalcaneal angle remains constant. These authors also described a decrease in the Kite angle, which was presumed to be caused by the talus rotating laterally and coming more in line with the calcaneus. However, the latter explanation for a decrease in the Kite angle assumes that the calcaneus has remained stationary and contradicts the former assumption that Kite angle remains constant for the posterior aspect of the calcaneus to rotate medialward as the talus rotates lateralward. A more plausible explanation for the decrease in Kite angle, as also noted in other publications4,10,28.31 and confirmed in this study using WBCT, is that the calcaneus must shift and rotate laterally in 3 dimensions beneath the talus in varying degrees. It can only do so at the subtalar joint through its various facets (Figure 6, A-D).

Decrease in Kite angle as the talar head rotates laterally. (A, B) Partially superimposed axial images of Foot lL. The solid red line represents the longitudinal axis of the talus and has been extrapolated posteriorly for measuring the Kite angle. The talar head has rotated laterally with an axial talus–first metatarsal (TFMA-A) or anteroposterior Méary angle of +27.9 degrees. Kite angle measures 27.3 degrees at the contralateral normal right foot. If, as part of the coxa pedis, the calcaneus was to rotate medially hand in hand with the laterally rotating talar head, the Kite angle would have been expected to remain constant. Instead, the Kite angle decreased to 14.3 degrees, that is, 13 degrees less than on the opposite normal side. By inference, the calcaneus must have shifted laterally toward valgus to a certain degree. It can only do so through the facets of the subtalar joint: (C) lateral (solid red arrows) and (D) posterior (dashed white arrow) middle facet subluxation, and superior subluxation at the posterior facet (solid white arrow). Note also the associated medial and anterior opening of the middle facet joint. The greater degree of lateral subluxation observed at the medial than at the lateral aspect of the middle facet suggests a 3-dimensional rotatory displacement rather than a uniplanar lateral shift. Varus hindfoot in talus configuration A (varus 33-50-67). Inftal-suptal angles open laterally at all 3 levels, (E) 33%, (F) 50% and (G) 67%, as designated by orange tick marks moving from anterior to posterior along the posterior facet. Despite 72% lateral middle facet subluxation, a combination of marked lateral talar rotation and varus-favorable talus configuration resulted in (H, I) a varus hindfoot moment arm of −11.92 mm (green tick marks and text). 3D volume rendering WBCT image confirms left heel varus.
Significantly greater degree of middle facet subluxation in the valgus-offset feet, particularly in the coronal plane, may partly account for how these heels compensate for the varizing moment caused by concurrent lateral rotation of the talus, displacing instead toward valgus offset. The lesser degree of lateral subluxation in the varus-offset feet is not sufficient to compensate for the varizing vector arising from lateral talar rotation, hence the residual hindfoot varus. This is despite a greater degree of medial opening of the middle facet in the varus-offset feet, which may thus represent a greater attempt at limiting hindfoot varus in these feet (Table 2).
At the posterior subtalar facet, although uncoverage of the most uncovered subregions 7, 8 and 9 is greater in valgus-offset than in varus-offset feet, the differences are not statistically significant. The situation is analogous to PCFD, where although uncoverage is increased at all 3 subtalar facets, it is only significant at the middle, but not at the anterior and posterior facets. 26 In another study of PCFD, significantly greater subluxation occurs at the middle than at the posterior facet (median difference, 17.7%) with a 1.6-fold increase in MFSC for every corresponding 1% increase in posterior facet subluxation. 25 By subregion, highest decreases in coverage of the middle-lateral and posterior-lateral subregions in PCFD do not reach statistical significance either.
Of the 3 posterior subregions in MWD, posterior-medial subregion 7 has the maximum uncoverage. Middle-middle and middle-lateral subregions 5 and 6 remain relatively well covered, whereas anterior-lateral subregion 3 is the most uncovered of the 3 anterior subregions. This pattern of decreased coverage indicates a rotatory lateral, superior and posterior subluxation of the calcaneus in MWD, with the center of rotation located at the level of the middle-middle subregion 5 (Figure 3).
Cody et al 33 documented significant differences in inftal-suptal angles at the 50% mark along the posterior facet between PCFD (21.2 ± 6.7 degrees) and normal feet (10.7 ± 6.4 degrees) (P < .001). Only 2 of 27 normal controls (7.4%) had angles greater than 17 degrees compared with 33 of 45 feet with PCFD (73.3%). Feet with an inftal-suptal angle of greater than 17 degrees were hence deemed to be at high risk of collapse and development of symptoms, deserving of special attention, such as early operative treatment and greater medialization of the calcaneal tuberosity at surgery. They also detected significant correlations between inftal-suptal angles and measures of PCFD such as TFMA-S (P < .001) and hindfoot alignment angles (P = .004). Because inftal-suptal angles should not be affected by age or progression of deformity, the authors hypothesized that patients born with a more inclined posterior subtalar facet have an intrinsic inherent factor that places them at higher risk of developing PCFD. Similarly, Probasco et al 23 had previously proposed that valgus orientation of the subtalar joint could predispose to development of PCFD.
Along the same lines, our results indicate that a talar configuration with varus inftal-suptal angles (open laterally) at all 3 levels is more conducive towards varus offset (Figure 6, E-I). Conversely, with valgus inftal-suptal angles (open medially) at all 3 levels, no varus offset occurs with 100% in valgus offset (Figure 7). The incidence of valgus offset in talus configurations with valgus inftal-suptal angles at the 50% and 67% marks is 80% (Figure 7), and 83% with valgus inftal-suptal angles at the 67% mark alone (Figure 8). Thus, a valgus-favorable inftal-suptal angle at the 67% mark alone may be as important as a valgus-favorable configuration at both 50% and 67% marks, in determining hindfoot position. In fact, differences in inftal-suptal angles between varus-offset and valgus-offset feet are statistically more significant at the 67% mark (P < .001) than at the 50% mark (P = .005) (Figure 4).

Valgus hindfoot in talus configurations B and C. Foot 3L. (A) Compression and fragmentation of lateral navicular with formation of talo-cuneiform pseudo-articulation and dorsal extrusion of the lateral navicular fragment (Maceira stage V disease). The longitudinal axis of the talus passes medial to the long axis of the first metatarsal forming a TFMA-A or anteroposterior Méary angle of −10.9°. (B) Middle facet subluxation of 44.5% with associated degenerative changes. Talus configuration B (valgus 33-50-67) with inftal-suptal angles open medially at all 3 levels, (C) 33%, (D) 50% and (E) 67%, as designated by green tick marks. (F, G) Valgus hindfoot moment arm (HMA) of +7.86 mm (green text and tick marks). Note also the different talus configuration C (varus 33; valgus 50-67) shown in black dotted lines at opposite Foot 3R which has a valgus HMA of +8.46 mm (valgus). 3D volume rendering WBCT images corroborate the valgus offset of both heels.

Valgus hindfoot in talus configuration D. Foot 7R. (A) Compression of lateral navicular bilaterally with fragmentation at the right foot. (B) Middle facet subluxation of 23.4%. Talus configuration D (varus 33-50; valgus 67) with inftal-suptal angles open laterally at (C) 33% and (D) 50% levels and inftal-suptal angle open medially at (E) 67% level. (F, G) Valgus hindfoot moment arm of +2.86 mm (green text and tick marks). 3D volume rendering WBCT image corroborates the right heel valgus.
The range of normal HMA varies widely in the literature. Saltzman and El-Khoury reported a neutral range of 0 ± 15 mm, based on 2-dimensional hindfoot alignment radiographic views in 57 asymptomatic adults. 11 Based on WBCT in 375 patients, Arena et al 22 reported a neutral range of −7.5 to 19.7 mm, whereas Choi et al 34 from analysis of a large series of 1128 feet quoted a normal range of 0.9 to 11.34 mm. We have presented our findings based on a neutral zero HMA partly because surgical reconstruction would aim for a near zero postoperative HMA with slight overcorrection. 35 Accordingly, 10 (45%) feet with negative HMA values are designated as varus-offset and 12 (55%) with positive HMA values as valgus-offset. Using the neutral HMA range of 0.9 to 11.34 mm, the same 10 varus-offset feet would be classed in varus malalignment. Of the 12 valgus-offset feet, 11 (92%) would be classed in neutral alignment, and only 1 foot in valgus malalignment. When comparing between the 10 varus-offset vs the 12 valgus-offset feet, and between the 10 varus-malaligned vs the 11 neutrally aligned feet, statistics for all parameters are almost identical, in particular, MFSC and inftal-suptal angles, the pertinent measurements with significant differences.
A strength of this study is its use of advanced WBCT imaging techniques for more accurate measurements of a comprehensive set of radiographic parameters in the largest series of MWD feet to date (Table 4). It offers novel and valuable insight into alignment of the various hindfoot joints in MWD. However, a major limitation is lack of correlation with clinical measures. Future studies should seek to correlate clinical assessment parameters and outcomes with radiographic findings to more clearly guide treatment and prognosis, according to disease stage and the perinavicular joints involved.4,28 This requires global collaboration for the larger number of cases necessary to attain statistical significance, because although increasingly more recognized, MWD remains relatively rare compared with PCFD and access to WBCT is still not readily available even in many major centers worldwide. Additionally, rotation of the lower limb influences weightbearing imaging foot measurements as demonstrated by hindfoot alignment radiographs obtained in natural radiographic vs straight radiographic position. 11 The patients in this study were instructed to weight bear in a natural standing position. Because patients with MWD frequently have concomitant varus malalignment above ankle level, 4 future WBCT imaging should perhaps include the knee and hip to account for any angular or rotational malalignment arising above the ankle.
Intraobserver and Interobserver Reliability for Manual Measurements, Expressed as ICC Values and 95% CI. a

Abbreviations: AP, anteroposterior; ICC, intraclass correlation coefficient; Inftal-suptal, angle formed between inferior and superior talar surfaces; TFMA-A, talus–first metatarsal angle in axial plane; TFMA-S, talus–first metatarsal angle in sagittal plane.
Inftal-suptal was measured at 33%, 50% and 67% of the way, moving from anterior to posterior along the posterior subtalar facet.
Conclusion
The present research constitutes the largest cohort of MWD feet to have been analyzed in detail using WBCT imaging and validated parameters such as HMA and MFSC. It demonstrates that hindfoot is not always offset in varus in MWD. It also sheds some light on possible reasons for valgus offset to happen more frequently by confirming prior reports of decreased Kite angle in MWD, which can only happen with the calcaneus displacing laterally beneath the talus. It does so by varying degrees through the 3 facets of the subtalar joint, especially the middle facet (Supplemental Video). We also observe that different intrinsic alignments of the posterior subtalar facet (in valgus or varus) significantly influence the hindfoot deformity pattern found in MWD.
Importantly, our findings confirm that the appellation of “paradoxical pes planus varus” does not equate to mandatory heel varus. The term should hence be restricted to when both flatfoot and heel varus are present. Of clinical relevance, lateral displacement calcaneal osteotomy, as advocated by some authors,29 -31 should only be considered after confirming that hindfoot alignment is really in varus.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114261436393 – Supplemental material for Weightbearing Computed Tomography Reveals Why Heel Varus Is Not Always the Rule in Müller-Weiss Disease
Supplemental material, sj-pdf-1-fao-10.1177_24730114261436393 for Weightbearing Computed Tomography Reveals Why Heel Varus Is Not Always the Rule in Müller-Weiss Disease by John Wong-Chung, Wolfram Grün, Roslyn Cassidy, Erik Jesús Huánuco Casas, Robert Alistair Wilson and Cesar de Cesar Netto in Foot & Ankle Orthopaedics
Footnotes
ORCID iDs
Ethical Considerations
Ethical approval for this study was obtained from our institutional review board (Approval Number/ID: Pro00113556).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: John Wong-Chung, MCh, FRCSI, reports general disclosures of Paragon 28 (consultant); Foot and Ankle Surgery (associate editor). Robert Alistair Wilson, MB, FRCS(Orth), reports general disclosures of Stryker UK (education). Cesar de Cesar Netto, MD, PhD, reports general disclosures Paragon 28 (consultant, medical advisory board, royalties), CurveBeam AI (consultant, shareholder), Ossio (consultant), Zimmer (consultant), Stryker (consultant), International WBCT Society (co-founder, past president), Exactech (consultant), Arthrex (consultant), TayCo Brace (shareholder), Extremity Medical (consultant), AOFAS committee member, Foot Ankle Clinics editor-in-chief. Disclosure forms for all authors are available online.
Supplemental Material
Supplementary material is available online with this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.