
Abstract
Background:
This study aimed to compare the effectiveness of artificial intelligence (AI)-generated, personalized video-based exercise instructions with traditional paper-based leaflets in improving exercise adherence and accuracy among patients with Achilles tendinitis and plantar fasciitis, and to evaluate whether this approach can serve as a practical tool for home exercise education that enables physicians and physiotherapists to easily create customized exercise programs without the need for advanced technical expertise or external resources.
Methods:
159 patients diagnosed with Achilles tendinitis or plantar fasciitis were randomized into 2 groups, with 103 completing the study in the paper exercise group (n = 47) and video exercise group (n = 56). The video group received exercise instructions created using the Google Veo 3 AI platform, whereas the paper group received standard AAOS/OrthoInfo leaflets. Exercise adherence was assessed using the Exercise Adherence Rating Scale (EARS), and exercise accuracy was evaluated through a 3-stage scoring system for 4 specific foot stretching exercises.
Results:
There was no significant difference between the groups in overall exercise adherence rates (71% vs 73%, P = .276). The mean EARS scores were 18.4 ± 3.1 for the paper group and 18.9 ± 3.4 for the video group (P = .412). However, the video group demonstrated significantly higher accuracy in complex exercises, particularly the Towel Curls (2.82 ± 0.27 vs 2.23 ± 0.31, P < .001). Subgroup analysis revealed that educational level affected adherence in the paper group (P = .012), whereas no such difference was observed in the video group (P = .624).
Conclusion:
AI-generated video instructions demonstrate comparable effectiveness to traditional printed leaflets in supporting short-term exercise adherence and may enhance exercise accuracy, particularly for complex, multistep movements. This low-cost approach may enable health care professionals to readily create personalized exercise programs without copyright concerns or the need for advanced technical skills - offering a practical and scalable adjunct to conventional home exercise education.
Level of Evidence:
Level II, randomized controlled trial.

Keywords
Introduction
Exercise programs have become a fundamental component of both therapeutic and preventive practices in modern medicine.1,2 They play a crucial role in the management of musculoskeletal disorders, not only during the treatment process but also in maintaining effective rehabilitation afterward.3 -6 However, in practice, it is often not feasible to provide one-on-one exercise training to every patient. Therefore, exercise leaflets are provided to patients for home use to support the treatment process. Traditionally, these leaflets consist of printed visuals and instructions, but in recent years, with the widespread use of smartphones, video-based applications and digital platforms have begun to replace them. Video-based exercise programs facilitate the correct performance of movements and enhance patient engagement in the process. Increasing evidence in the literature indicates that these methods improve patient adherence and therapeutic effectiveness compared with conventional approaches.7,8
There are various international guidelines and programs developed to define exercise movements and standardize patient practice. 9 In addition, some exercise content sponsored by medical companies is also made available for clinicians. However, because of the individualized nature of clinical practice, these fixed-content materials can sometimes be insufficient or cause confusion. The creation of customized exercise programs by physicians or physiotherapists in visual or video format often faces obstacles such as the need for professional graphic design support, funding, or copyright issues. Therefore, the development of accessible, customizable exercise production tools that can directly meet clinical needs would provide a significant contribution to the field.
Artificial intelligence (AI) technologies are increasingly being used across many fields, including medicine. Numerous studies have investigated the effectiveness of AI-supported systems in health care services.10,11 In recent years, AI-based content generation tools have also begun to offer innovative solutions in areas such as health communication and patient education. In this context, Veo 3, an AI-powered video generation platform developed by Google, has gained attention. Veo 3 enables users to create highly realistic videos using only text prompts, without requiring professional video production expertise. This feature opens a new avenue for clinicians to efficiently produce personalized patient education materials, such as customized exercise programs.
Achilles tendinitis and plantar fasciitis are common musculoskeletal disorders that significantly affect patients’ quality of life. 12 In the conservative management of these conditions, particularly in the early stages, stretching exercises targeting the ankle and plantar surface are considered a cornerstone of treatment.13,14 In our study, patients presenting to our clinic with a diagnosis of plantar fasciitis or Achilles tendinitis were provided with exercise videos created using the AI-powered Veo 3 platform. These patients were compared with a control group that received only traditional exercise leaflets containing written and visual instructions. Although video-based exercise applications have been evaluated in previous studies, our study offers an innovative approach by utilizing videos that can be easily produced by clinicians themselves using AI, without copyright issues and at minimal cost. These videos, created with only basic computer skills, were shown to have a positive effect on patients’ exercise adherence. Furthermore, this approach demonstrates potential applicability not only for musculoskeletal disorders but also for various other areas of medicine, providing a scalable and personalized solution for patient education.
Materials and Methods
This study was conducted prospectively following the approval of the local ethics committee and in accordance with the principles of the Declaration of Helsinki. Patients who were examined by the researchers at our center and diagnosed with Achilles tendinitis or plantar fasciitis were included. In our routine clinical practice, these patients are prescribed medical treatment along with foot and ankle stretching exercises, which are usually provided through illustrated exercise leaflets. Between June 1, 2025, and July 15, 2025, patients diagnosed with Achilles tendinitis or plantar fasciitis by the researchers were randomly assigned into 2 groups: the paper exercise group, who received exercises via a traditional leaflet with images and written instructions, and the video exercise group, who received exercises through video instructions. The educational status of the participants was recorded. After obtaining informed consent, patients were given a separate follow-up form to record their adherence to the prescribed exercise program. Patients were randomly allocated to the 2 study groups using a computer-generated randomization list (1:1 ratio).
We performed an a priori sample size calculation for the primary outcome of exercise adherence, measured with the Exercise Adherence Rating Scale (EARS; range 0–24). Based on previous outpatient experience and pilot variability in similar musculoskeletal cohorts, we assumed a common SD of 3.2 points and set a minimal clinically important difference (MCID) between groups of 2.0 points. For a 2-sided 2-sample t test with α = 0.05 and 80% power, the required sample size was 41 participants per group (82 total). Accounting for attrition, we aimed to recruit at least 100 participants. In total, 81 patients were assigned to the paper exercise group, and 78 patients to the video exercise group. All participants were scheduled for a follow-up examination 15 days later. A 15-day follow-up period was selected to primarily assess early exercise adherence and accuracy while minimizing patient attrition. In routine outpatient settings, longer follow-up intervals are associated with higher loss to follow-up, which could compromise the reliability of adherence assessments. A total of 103 patients completed the study and attended the follow-up control examination (47 in the paper exercise group and 56 in the AI-video group). Given the loss to follow-up, baseline characteristics of patients who completed the 15-day follow-up were compared with those of noncompleters to assess potential attrition bias. Because of the inability to assess outcomes in patients who did not attend follow-up, analyses were conducted using a complete-case approach. The patient flow and attrition are detailed in the CONSORT flow diagram (Figure 1). Exercise accuracy was independently assessed by 2 orthopaedic specialists who were blinded to group allocation. Interrater reliability for exercise accuracy scores was evaluated using the intraclass correlation coefficient (ICC), based on a 2-way random effects model with absolute agreement (ICC [2,1]).
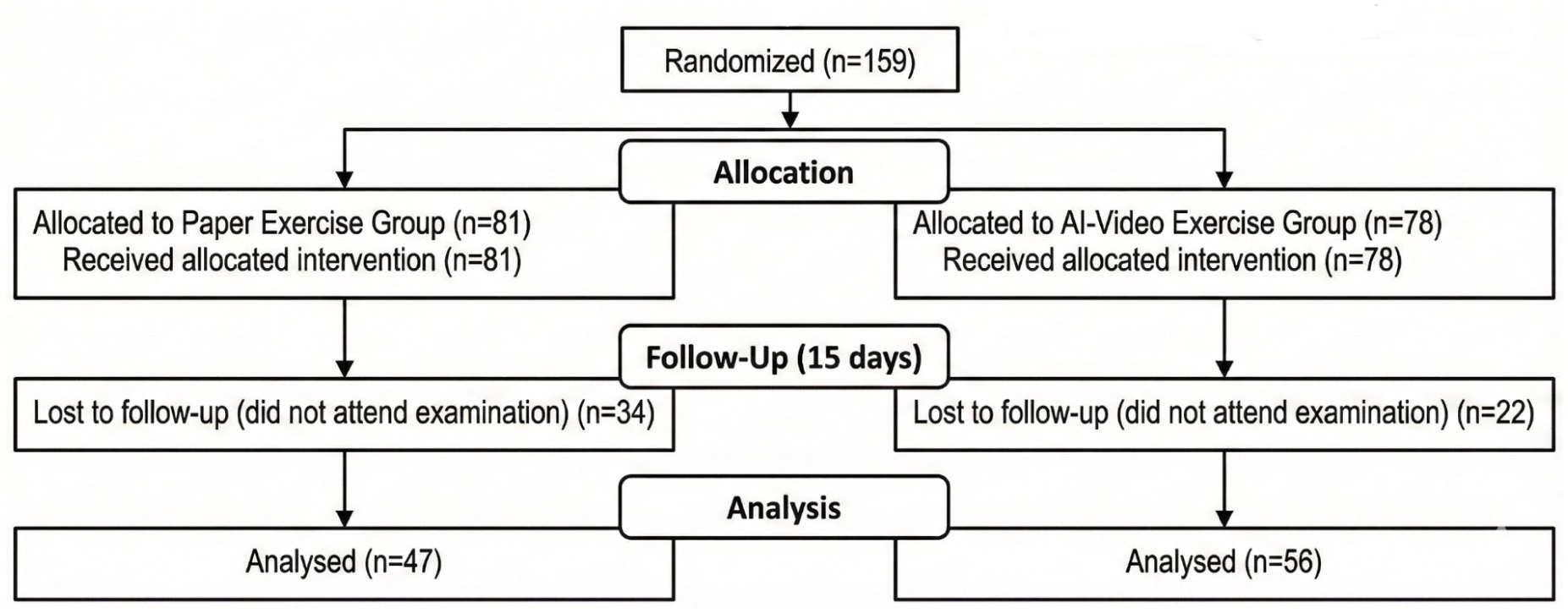
CONSORT flow diagram illustrating patient randomization, allocation to study groups, follow-up at 15 days, loss to follow-up, and final analysis.
Four main stretching exercises were selected for the study: Heel Cord Stretch, Golf Ball Roll, Towel Stretch, and Towel Curls. These exercises were chosen based on the AAOS/OrthoInfo foot and ankle exercise program. 15 Because golf balls are less common in our region, patients were instructed to use a cold 0.5-L plastic bottle instead. Heel Cord Stretch and Towel Stretch exercises were recommended to be performed in 2 sets of 10 repetitions per day, Ball Roll once per day for 2 minutes, and Towel Curls once per day for 20 repetitions. For the paper exercise group, the leaflet was prepared using images and content from the AAOS/OrthoInfo program (Figure 2).

The 4 exercises included in the study, adapted from the AAOS/OrthoInfo foot and ankle exercise program: (A) Heel Cord Stretch, (B) Golf Ball Roll, (C) Towel Stretch, and (D) Towel Curls.
In the video exercise group, instructional videos were produced using the Google Veo 3 AI-based video generation platform. The researchers, who were basic computer users without professional software support, generated the videos by writing prompts based on the AAOS/OrthoInfo exercise program. Multiple iterations were required to achieve the desired quality, with a total of 27 attempts. The Heel Cord Stretch required the highest number of attempts with 11, whereas the Towel Stretch was completed with only 2 attempts. Veo 3 currently limits videos to 8 seconds, so only the exercise movements were shown, whereas repetition counts and set information were provided separately on a printed sheet. Access to videos was provided through a QR code printed on the same sheet (Figure 3). To minimize potential barriers related to age or digital literacy, access to the QR code and video content was demonstrated to all participants during the outpatient visit. Patients were assisted in opening the videos on their personal smartphones, and instructions were repeated as needed to ensure successful access.

The 4 stretching exercises evaluated in the study and generated using the Veo 3 AI-based video platform: (A) Heel Cord Stretch, (B) Plantar fascia rolling using a cold 0.5-L bottle, (C) Towel Stretch, and (D) Towel Curls. This figure is provided to visually illustrate the exercises assessed for accuracy, including the multistep movements. The exercises were adapted from the AAOS/OrthoInfo foot and ankle exercise program.
At the 15-day follow-up visit, exercise adherence was assessed using the Exercise Adherence Rating Scale (EARS). 16 This scale evaluates both the quantitative and qualitative aspects of adherence and has been validated for use in musculoskeletal disorders. The EARS consists of 6 items, each scored from 0 (strongly disagree) to 4 (strongly agree), with total scores ranging from 0 to 24, where higher scores indicate better adherence. In addition, patients reported the number of sessions completed using their follow-up forms. Exercise accuracy was evaluated during the follow-up visit by the researchers. Each of the 4 exercises was divided into 3 stages, and a maximum score of 3 points was awarded for correct performance. Group comparisons were then made based on these scores.
All data were analyzed using IBM SPSS Statistics (version 26.0.0.0). The Kolmogorov-Smirnov test was used to assess normality of distribution for continuous variables. Normally distributed data were presented as mean ± SD, whereas nonnormally distributed data were reported as median (minimum-maximum). Categorical variables were presented as numbers and percentages. Comparisons between groups for EARS scores were performed using the independent samples t test or Mann-Whitney U test, depending on normality. χ2 or Fisher exact tests were used for comparisons of exercise accuracy rates. The adherence percentage calculated from follow-up forms was also compared as a supportive analysis. For statistically significant between-group comparisons, standardized effect sizes were calculated using Cohen d to aid interpretation of the magnitude of observed differences. A P value <.05 was considered statistically significant. For between-group comparisons, mean differences with 95% CIs were calculated to provide effect estimates in addition to P values. No formal multiplicity correction was applied for secondary outcome analyses; therefore, findings related to exercise accuracy were considered exploratory.
Results
The study was completed with a total of 103 patients, including 47 in the paper exercise group and 56 in the video exercise group who attended the follow-up examination. Baseline characteristics were comparable between patients who completed follow-up and those lost to follow-up, with no significant differences in age, sex, educational level, diagnosis, or group allocation (all P > .05), suggesting a low risk of attrition bias. Because 82% of the participants were female, gender-based comparisons were not performed (Table 1). During the 15-day follow-up period, the frequency of performing the 4 exercises was evaluated. In both groups, Ball Roll and Towel Stretch were the most frequently performed exercises, whereas Heel Cord Stretch was the least performed. The exercise adherence rate was calculated as 71% in the paper exercise group and 73% in the video exercise group, with no statistically significant difference between the groups in terms of exercise adherence (P = .276). Interrater reliability for exercise accuracy assessment was high (ICC = 0.87; 95% CI, 0.74-0.88).
Demographic and Baseline Characteristics of the Study Participants.

Each patient’s performance was evaluated separately for the 4 different exercises: Heel Cord Stretch, Ball Roll, Towel Stretch, and Towel Curls. Exercises were scored in 3 stages, with a maximum score of 3 for each exercise. The mean scores for the paper exercise group vs the video exercise group were as follows: Heel Cord Stretch (2.51 vs 2.64), Ball Roll (2.49 vs 2.66), Towel Stretch (2.72 vs 2.88), and Towel Curls (2.23 vs 2.82). According to Mann-Whitney U test results, there were no statistically significant differences between the groups for Heel Cord Stretch (P = .353), Ball Roll (P = .239), or Towel Stretch (P = .054). However, a significant difference was observed for the Towel Curls exercise, with the video group demonstrating higher accuracy scores (P < .001) (Table 2). The corresponding mean differences (video minus paper) were 0.13 points for Heel Cord Stretch (95% CI, −0.15 to 0.41), 0.17 points for Ball Roll (95% CI, −0.11 to 0.45), 0.16 points for Towel Stretch (95% CI, −0.01 to 0.33), and 0.59 points for Towel Curls (95% CI, 0.48 to 0.70). The video exercise group demonstrated significantly higher accuracy in the Towel Curls exercise compared with the paper exercise group, corresponding to a large effect size (Cohen d = 1.98).
Comparison of Exercise Adherence Rates and Accuracy Scores Between the Paper Exercise Group and the Video Exercise Group.
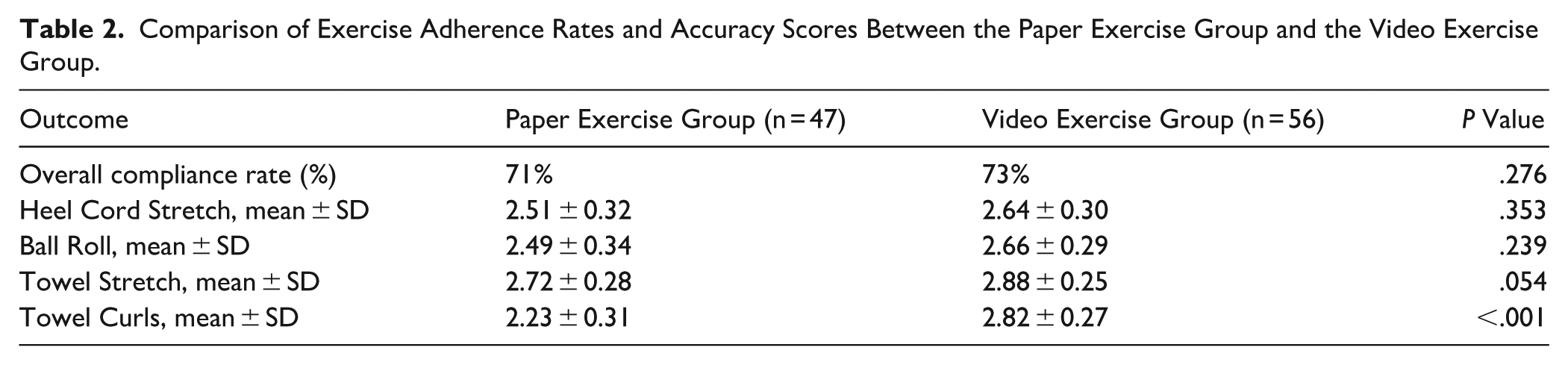
The mean EARS score was 18.4 ± 3.1 in the paper exercise group and 18.9 ± 3.4 in the video exercise group, and the difference between the groups was not statistically significant (P = .412), indicating that both methods provided similar short-term exercise adherence levels. The mean difference in EARS scores between the video and paper exercise groups was 0.5 points (95% CI, −0.7 to 1.6; P = .412).
Patients were divided into 2 groups based on educational level: university graduates and nongraduates. In the paper exercise group, university graduates demonstrated significantly higher performance in both exercise adherence and exercise accuracy. The mean EARS score was 19.3 ± 3.1 for university graduates and 16.8 ± 3.2 for nongraduates (P = .012). The mean exercise accuracy score was 2.81 ± 0.24 for university graduates and 2.54 ± 0.28 for nongraduates (P = .029). In contrast, in the video exercise group, performance levels were similar between educational subgroups. The mean EARS score was 18.7 ± 3.2 for nongraduates and 18.9 ± 3.1 for university graduates, with no statistically significant difference (P = .624). Similarly, the mean exercise accuracy score was 2.73 ± 0.26 for university graduates and 2.71 ± 0.27 for nongraduates (P = .587). Educational level had a significant impact on both exercise adherence and accuracy in the paper exercise group (Cohen d = 0.78 for adherence and 0.91 for accuracy), whereas no such educational-level differences were observed in the video exercise group, suggesting that video-based instruction may mitigate education-related disparities (Table 3).
Comparison of EARS Scores and Exercise Accuracy Between Participants With and Without a University Degree in the Paper Exercise and Video Exercise Groups.

Discussion
Exercise plays an important role in the conservative management of musculoskeletal disorders.4 -6 Physicians and physiotherapists typically recommend exercises either by demonstrating them directly to patients or through printed leaflets and digital materials. Although the use of mobile applications and video platforms for exercise recommendations has increased with the widespread adoption of smartphones, printed leaflets remain commonly used in outpatient settings. With the growing integration of AI technologies into health care, it has become possible for users to generate content without requiring advanced technical skills. One such technology is platforms capable of producing realistic videos from simple text commands. Google Veo 3 is among the most popular tools that allow the creation of exercise videos using only basic computer skills. To address the need for accessible patient education materials, in this study, we compared the usability of exercise videos generated using Google Veo 3 with that of traditional printed exercise leaflets. We selected foot stretching exercises frequently recommended in our outpatient clinic, and our findings demonstrate that this technology enables physicians and physiotherapists to easily prepare personalized exercise programs at minimal cost and without copyright issues.
In our study, it was observed that patients in the video group performed the exercises more accurately compared to those in the paper group. While no significant difference was noted between the groups for simple, single-step exercises, patients in the video group demonstrated greater accuracy in complex and multistep exercises. Similarly, Gupta and Sehgal 17 and Thiengwittayaporn et al 18 reported that digitally delivered exercise programs significantly improved the correct execution of movements compared to paper-based methods. These findings support the results of our study. In our research, videos were generated using the Google Veo 3 platform. Currently, the video production time in Veo 3 is limited, which is why relatively simpler and shorter exercises were selected. As the complexity of exercises increases, the impact of video-based education is expected to become even more pronounced. With future advancements in AI-driven video generation platforms, it will be possible to create longer and more precisely tailored videos, allowing patients to perform their exercises more effectively and accurately. Moreover, the integration of applications that organize and remind patients about their exercise programs could help establish a comprehensive and efficient exercise regimen.
In the study conducted by Chung et al, video-guided home exercise programs were shown to be superior to paper-based programs in terms of exercise adherence and functional outcomes. This study indicated that video content helped patients perform the exercises more accurately and completely while also increasing motivation. 7 Similarly, in a systematic review by Lang et al, 8 digital and video-based interventions were reported to significantly improve participation and continuity in home exercise programs. The data from these studies demonstrated that digital content particularly strengthens exercise adherence during long-term follow-up and facilitates the integration of exercise into patients’ daily routines. In contrast, studies by Svingen et al 19 and Van Reijen et al 20 reported no significant differences in exercise adherence when using digital exercise instructions. Consistent with these findings, our study also found no significant difference between the paper-based and video-based exercise groups in terms of adherence to the prescribed exercise program.
The elimination of education-level differences in the video group in our study indicates that video-based exercise materials provide a significant advantage for individuals with low health literacy. It is well known that, with paper-based exercise programs, individuals with lower education levels often face difficulties in understanding and regularly performing the exercises correctly. Zangger et al 21 reported that video-based exercise education is more effective among individuals with low health literacy. Video content combines visual and auditory elements, presenting movements in a clearer and more comprehensible way, thereby reducing the performance gap related to education level.
An important and clinically relevant finding of this study was the influence of educational level on exercise performance in the paper exercise group, where higher educational attainment was associated with better adherence and accuracy. Notably, this education-related disparity was not observed in the video exercise group, suggesting that AI-generated video instructions may help mitigate barriers related to health literacy and educational background. This finding has practical implications for improving equity in home exercise education, particularly in diverse patient populations.
AI-based video generation is still in the early stages of development. Although the videos produced today are limited in terms of duration, resolution, and content, with the rapid advancement of technology, it will soon be possible to create longer, higher-quality, and fully personalized videos. Therefore, it is crucial for physicians to become familiar with such technologies at an early stage and closely follow developments. The integration of AI-based video generation tools into health care has the potential to save time for physicians in patient education and rehabilitation processes, reduce costs, and make treatment plans more effective and accessible. This approach could provide significant convenience in medical practice, while also enhancing patient engagement and satisfaction with their treatment.
Our study has several limitations. First, the follow-up period was limited to 15 days, which prevented the evaluation of the long-term sustainability of exercise adherence. Additionally, because of the current video duration limitations of the Google Veo 3 platform, only simple exercises were included in this study. Results may differ as the complexity of the exercises increases. Exercise adherence was primarily assessed based on patient self-report, which restricts the objectivity of the measurements, and introduces potential recall and social desirability biases. Patients without access to a smartphone or those unable to use mobile devices despite assistance were not included in the study, which may limit the generalizability of the findings to populations with very low digital literacy. The relatively short follow-up period limited the assessment of long-term adherence and clinical outcomes; however, it allowed a more reliable evaluation of early adherence and exercise accuracy with minimal loss to follow-up. Pain outcomes were not analyzed, as the short 15-day follow-up period may not be sufficient to detect meaningful clinical changes in pain for Achilles tendinitis or plantar fasciitis. Future studies with longer follow-up may explore the relationship between exercise education methods and pain-related outcomes. In addition, the secondary analyses of exercise accuracy should be interpreted as exploratory, as no formal adjustment for multiple comparisons was applied. Furthermore, the study was single-centered, and the majority of participants were female (82%), which limits the generalizability of the findings to broader populations. Future studies may further compare AI-generated exercise videos with provider-created or professionally guided video content, rather than printed materials alone, to better delineate the relative educational effectiveness of different video-based approaches.
Conclusion
In this study, exercise videos created with the Google Veo 3 artificial intelligence platform were compared with traditional paper-based exercise leaflets for patients with Achilles tendinitis and plantar fasciitis. The findings demonstrated that exercise adherence was similar between the 2 groups, while patients in the video group showed improved exercise accuracy, particularly for more complex and multistep exercises. These results highlight the potential of video-based instructions to enhance the quality of home exercise performance without altering overall adherence.
AI-generated video content offers a cost-effective, customizable, and copyright-free alternative for health care professionals, enabling them to create personalized exercise programs without advanced technical skills. As AI technology continues to evolve, longer and higher-quality videos will become feasible, further enhancing the effectiveness of patient education and rehabilitation. Integrating such technologies into clinical practice could significantly improve treatment accessibility and adherence, especially in populations with limited health literacy or low socioeconomic status.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114261436388 – Supplemental material for AI-Generated Exercise Videos vs Traditional Leaflets: A Novel Approach to Home Exercise Education in Achilles Tendinitis and Plantar Fasciitis: A Randomized Controlled Trial
Supplemental material, sj-pdf-1-fao-10.1177_24730114261436388 for AI-Generated Exercise Videos vs Traditional Leaflets: A Novel Approach to Home Exercise Education in Achilles Tendinitis and Plantar Fasciitis: A Randomized Controlled Trial by Nuri Koray Ülgen, Ali Said NazlıgÜl, Nihat Yiğit, Arslan Kağan Arslan and Mehmet Orçun Akkurt in Foot & Ankle Orthopaedics
Footnotes
Acknowledgements
The authors would like to thank the patients who participated in this study.
Ethical Considerations
This study was conducted in accordance with the principles of the Declaration of Helsinki and was approved by the local ethics committee, Sincan Training and Research Hospital Scientific Research Ethics Board (study no. BAEK-2025-86).
Consent to Participate
Written informed consent was obtained from all participants before inclusion in the study.
Consent for Publication
Written informed consent was obtained from all participants for the publication of anonymized data.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Disclosure forms for all authors are available online.
Data Availability Statement
The datasets generated and/or analyzed during the current study are available from the corresponding author upon reasonable request.