
Abstract
Background:
Standard treatment of calcaneal fractures involves prolonged immobilization with partial weight-bearing, risking ankle stiffness and lower-leg deconditioning. The heel-unloader enables early full weight-bearing by redirecting axial load from the hindfoot to the midfoot, forefoot, and lower leg. This study compares radiologic and clinical outcomes of heel-unloader vs conventional cast immobilisation.
Methods:
We retrospectively analyzed 101 calcaneal fractures treated with cast immobilization and partial weight-bearing or a heel-unloader with early full weight-bearing. Böhler angle (BA) loss, evaluating macroscopic fracture displacement and heel height, was the primary endpoint; secondary outcomes were pain, ankle/subtalar motion, complications, and radiologically subtalar degeneration. Equivalence in BA loss was tested by 2 one-sided tests (TOST).
Results:
Overall, 16.8% of the fractures were managed non-operatively and 83.2% operatively, with similar distributions between the groups (P = .397). After 4 weeks of non-weight-bearing, 59 (58.4%) fractures continued in a heel-unloader and 42 (41.6%) with a cast. Baseline and fracture characteristics were comparable. Mean BA loss at 12 weeks was −4.7° ± 5.3° (heel-unloader group) vs −3.8° ± 5.5° (cast group) (P = .44), confirming equivalence (TOST P < .001). Other outcomes showed no significant differences.
Conclusion:
Early full weight-bearing with a heel-unloader yields radiologically and clinically equivalent macroscopic results to traditional casting and is a safe alternative for early mobilization.
Level of Evidence:
Level III, retrospective comparative study.
This is a visual representation of the abstract.
Keywords
Introduction
Calcaneal fractures account for approximately 2% of all fractures and represent about 60% of tarsal injuries, often affecting active, working-age individuals. 1 Despite numerous clinical and biomechanical studies, there is no universally accepted protocol regarding optimal weight-bearing and immobilisation strategies following non-operative and operative treatment. Traditionally, non-weight-bearing for up to 12 weeks using a below-knee cast has been the standard to prevent secondary displacement and allow for bony healing.2,3 However, prolonged immobilisation may lead to significant deconditioning, joint stiffness, and loss of independence, especially in elderly or polytraumatized patients.4,5
Heel-unloader orthosis represents a functional alternative that enables full weight-bearing while minimizing axial load on the calcaneus. First introduced as the Settner shoe in 1994, the orthosis redistributes force from the hindfoot to the midfoot and forefoot, enabling mobilisation without compromising fracture stability.6,7 Initial studies have demonstrated that patients using such orthosis may achieve improved early functional outcomes, such as higher AOFAS scores at 3 months post-injury.8,9 Moreover, the ability to walk without crutches and maintain daily activities may enhance quality of life and accelerate return to work.10,11
Nevertheless, concerns remain regarding the mechanical safety of early weight-bearing in terms of fracture subsidence or malalignment. This study aims to compare clinical and radiologic outcomes of early full weight-bearing using a heel-unloader orthosis to those of conventional cast treatment in patients with calcaneal fractures.
Methods
Patient Selection
This retrospective study includes all patients treated either operatively or non-operatively for calcaneal fractures at our institution between 2014 and 2025.
Heel-unloader orthosis was introduced as a standard component of treatment in 2018. Therefore, patients treated prior to 2018 received as standard treatment immobilisation with a lower leg cast for 12 weeks and partial weight-bearing. Since 2018, all patients have been treated with a heel-unloader, receiving a non-weight-bearing cast for the first 4 weeks, followed by full weight-bearing in the heel-unloader for 8 weeks.
Patients with calcaneal fractures treated either non-operatively or operatively were eligible for inclusion in this study. Two treatment modalities were considered: early full weight-bearing with a heel-unloader orthosis and prolonged partial weight-bearing using a traditional cast.
The aim of this study is to assess the effectiveness and equality of the heel-unloader orthosis in the treatment of calcaneal fractures.
Exclusion criteria comprised the absence of radiologic or clinical follow-up data, lack of general consent, and open fractures requiring skin grafting.
The primary outcome was secondary loss of macroscopic fracture reduction within 12 weeks of full weight-bearing in the orthosis, as seen on radiographic controls evaluating macroscopic displacement and heel height, with a resulting Böhler angle (BA) of <15°.5,12 Secondary outcome included the complication rate (pressure ulcers), the upper (dorsiflexion/plantarflexion) and lower ankle (inversion/eversion) joint mobility, and the development of subtalar osteoarthritis at 6 months and 1-year post-treatment, as seen on follow-up radiographs.
Demographics and Outcomes
All electronic records of the eligible patients were reviewed and the following data were abstracted and analyzed: demographics (age, gender, body mass index [BMI]), comorbidities (smoking, alcohol abuse); fracture classification according to Essex Lopresti 13 and Sanders classification 14 ; date of injury; time to definitive surgery (if applicable); presence of pain at 4, 8, and 12 weeks post-treatment; and need for revision surgery within the first 12 weeks post-injury.
Definitions and Measurements
The BA as the index of calcaneal height was measured in the lateral foot radiograph between a line joining the highest point of the anterior process of the calcaneus and the highest point of the posterior articular facet, and a line joining the highest point of the posterior articular facet with the highest point of the calcaneal tuberosity as seen in Figure 1. 15 The BA measured on the initial radiographs and subsequently on follow-up radiographs obtained at 4, 8, and 12 weeks, as well as at 1 year post-treatment, to assess fracture alignment and healing progression.

Lateral calcaneal radiograph showing Böhler angle, formed by a line from the anterior process to the posterior articular facet (light blue dotted) and a line from the posterior facet to the calcaneal tuberosity (blue dashed).
Radiographs at the 1-year follow-up were also evaluated for signs of degenerative changes of the subtalar joint concerning the Kellgren and Lawrence classification. 16 A distinction was made between classification grade 0 and >0.
All radiographic measurements were performed by a senior attending foot and ankle surgeon using standardized digital PACS measurement tools and predefined anatomical landmarks. A subset of measurements was re-evaluated to ensure internal consistency.
Treatment
At our clinic, all diagnosed closed calcaneal fractures are initially immobilised with a plaster cast as standard. A CT scan of the calcaneus is then performed to assess the fracture configuration accurately and decide between operative and non-operative treatment. The CT scan also aids in preoperative planning. Decision regarding indication for surgery was based on the fracture dislocation, alignment, and the general condition of the patient. Indication for surgery did not differ between the 2 study groups. The patients who underwent surgery were all treated via a sinus tarsi approach. The first 4 weeks after trauma, all patients were immobilised in a lower-leg cast without weight-bearing to allow soft tissue swelling to subside and to ensure proper postoperative wound healing.
Prior to 2018, patients received a lower leg plaster cast for 12 weeks at the start of treatment, with 4 weeks of non-weight-bearing, and 4 weeks with 10-kg and 4 weeks with 20-kg partial weight-bearing. Since 2018, immobilisation has been carried out for 4 weeks in a lower leg cast without weight-bearing, followed by full weight-bearing in the heel-unloader orthosis as seen in Figure 2 for a further 8 weeks. The heel-unloader orthosis is custom-fabricated using a digital scan of the lower leg up to knee height, followed by computer-aided modification and milling of a foam model. A carbon-fiber shell is then manufactured and combined with a specially prepared shoe component, incorporating a posterior heel cut-out filled with cushioning material to achieve targeted pressure relief. The final orthosis is completed with soft padding and Velcro straps to ensure patient comfort and secure fixation. The costs amount to approximately US$2900, which are covered by local health insurance companies.

Custom heel-unloader with carbon shell and posterior heel cut-out for targeted pressure relief.
Low-molecular-weight heparin is routinely administered for thromboembolism prophylaxis. Routine follow-ups for clinical and radiologic evaluation are set at 3, 6, 12, 24, and 52 weeks.
Statistical analysis
The patients were divided into 2 groups: heel-unloader group and cast group.
To assume sample size using power analysis, we used the results based on a previous study reporting a mean difference in BA loss of 0.4° 17 (2.4° vs 2.0°) with a pooled SD of 2.88°. Assuming an equivalence margin of ±5°, a 2-sided α level of .05, and a power of 80%, the required sample size was calculated to be 32 patients per group to demonstrate statistical equivalence.
The P values for categorical variables were derived from the Pearson χ2 or the 2-sided Fisher exact test. For continuous variables, the Student t test or the Mann-Whitney tests were deployed.
Statistical analyses were performed using standard parametric tests for group comparisons. To assess the equivalence of postoperative outcomes between groups, a two one-sided test (TOST) procedure was employed with predefined equivalence margins.
Values are reported as mean ± SD for continuous variables and as percentages for categorical variables. Differences were considered statistically significant when P ≤.05. The data were analyzed using R (R Foundation for Statistical Computing). 18
Ethical approval for this study was received by the local ethical committee 2023-00064.
Results
Between January 2014 and January 2025, a consecutive series of 124 adult patients with 139 calcaneal fractures were treated at our institution. A total of 33 patients with 38 fractures were excluded, resulting in a study cohort of 91 patients with 101 calcaneal fractures (Figure 3).
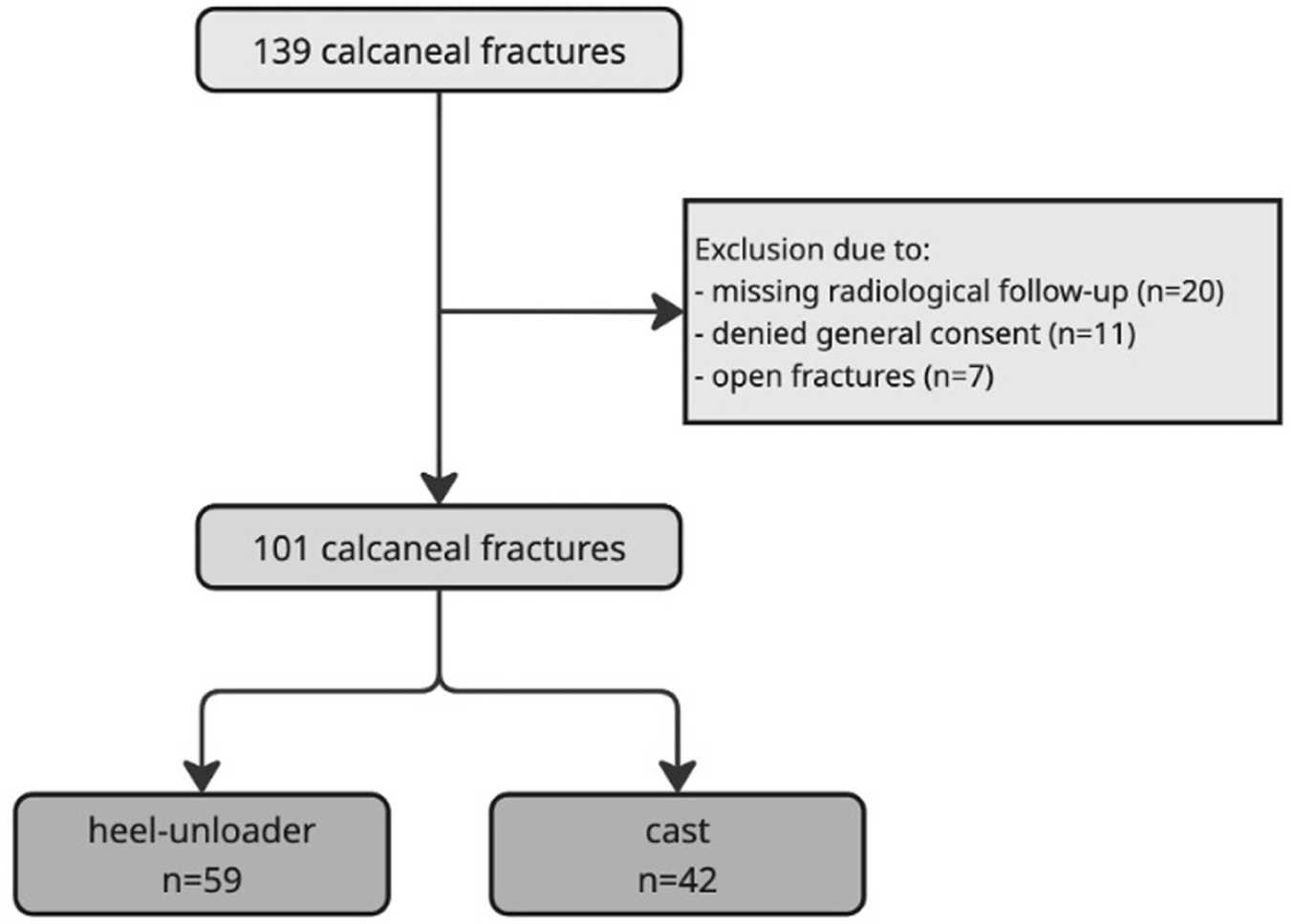
Flowchart.
The study cohort included 31 women and 60 men with a mean age of 46.3 ± 16.4 years (range 17.2-83.7 years). Overall, 16.8% of the fractures were treated non-operatively and 83.2% operatively. Of the 101 calcaneal fractures, 59 (58.4%) were treated with a heel-unloader, whereas 42 (41.6%) were treated with a cast.
Demographic factors and comorbidities were comparable between fractures treated with a heel-unloader and with a cast (Table 1). No statistically significant differences were found comparing age, operative or non-operative treatment, smoking, and alcohol abuse.
Comparison of the Two Groups Regarding the Demographic Characteristics and Comorbidities.

Furthermore, there was a homogeneous distribution of fractures across the 2 treatment groups, with no statistically significant differences in terms of fracture classification according to Sanders or Essex Lopresti. The most common fracture type according to the Sanders classification was type 2, accounting for 40.6% of cases, and according to Essex Lopresti, the joint depression type, accounting for 76.2%.
Analysis of the BA in the operatively treated fractures preoperative (22.6 ± 11.1 vs 18.7 ± 12.1; mean difference: 4.1°, 95% CI: −3.3° to 11.6°; P = .0997) showed no significant difference in the heel-unloader group and the cast group. There were no significant differences in the BA between the 2 groups immediately postoperative and at the beginning of the immobilisation (29.3 ± 6.36 vs 29.1 ± 8.1; mean difference 0.2°, 95% CI: −2.8° to 4.5°; P = .865) or at 4 (25.2 ± 7.4 vs 26.1 ± 8.9; mean difference −0.9°, 95% CI: −4.7° to 2.8°; P = .632), 8 (25.5 ± 8.2 vs 25.8 ± 9.0; mean difference −0.4°, 95% CI: −4.5° to 3.8°; P = .887), and 12 (24.5 ± 8.0 vs 25.9 ± 8.9; mean difference −1.4°, 95% CI: −5.2° to 2.4°; P = .400) weeks post-traumatic. Furthermore, the average BA was within the normal range 12 weeks after the trauma.
Both in the heel-unloader group (29.3 vs 25.2; mean loss 4.1°, 95% CI: 2.9°-6.8°; P < .001) and in the cast group (29.1 vs 26.1; mean loss 3.0°, 95% CI: 0.9°-5.1°; P = .002), there was a significant loss of the BA angle in the first 4 weeks after the start of treatment. In the following periods between 4 and 8 weeks and between 8 and 12 weeks, there was no significant loss of alignment (Figure 4, Table 2).

Progression of the Böhler angle (BA) over time from 0 to 12 weeks in the cast and the heel-unloader group.
Comparison of the Two Groups Regarding the Böhler Angle (BA) at 0, 4, 8, 12 Weeks and Their Significant Difference.
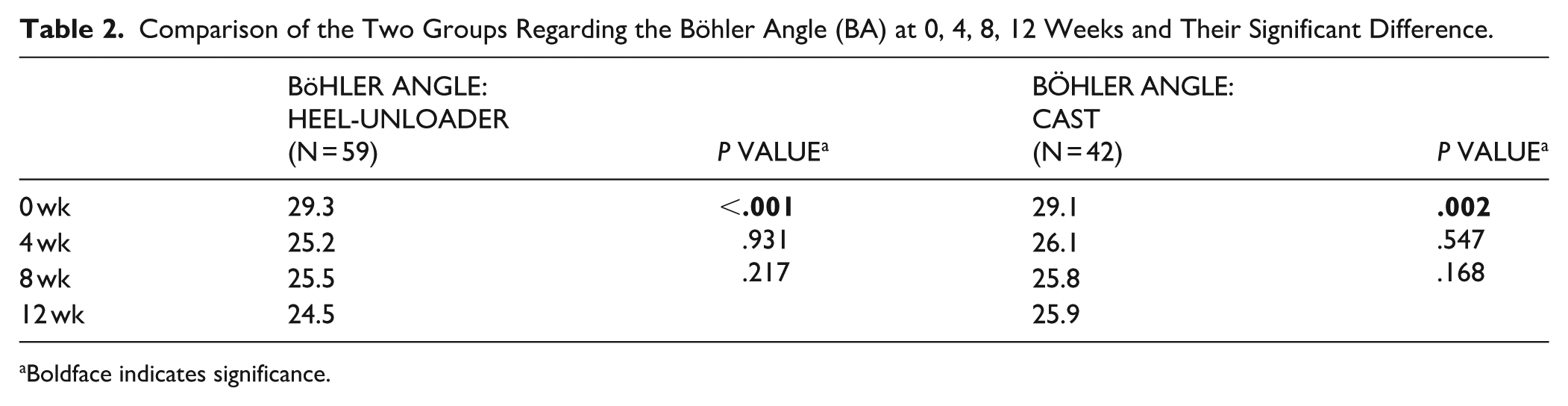
Boldface indicates significance.
The loss of BA over 12 weeks showed no significant difference between the heel-unloader group and the cast group (−4.7 ± 5.3 vs −3.8 ± 5.5; mean difference −0.9°, 95% CI: −0.3° to 5.6°; P = .4409).
An equivalence test (TOST procedure) confirmed that the difference in angle loss between the 2 groups was statistically equivalent within a predefined margin of ±5 degrees. Both 1-sided t tests were significant (t = 3.2, P = .001; t = −4.7, P < .00001), confirming that the observed difference is clinically negligible.
Functional ankle range of motion (ROM) did not differ significantly between the groups at 12 weeks. Mean plantarflexion was 26.9° ± 9.2° in the heel-unloader group and 23.9° ± 7.1° in the cast group (mean difference 3.0°, 95% CI: −2.3° to 7.4°; P = .197). Dorsiflexion averaged 12.6° ± 7.6° and 10.9° ± 7.0° in the heel-unloader and cast group (mean difference 1.7°, 95% CI: −2.5° to 5.9°; P = .394). The mean ROM was 39.4° in the heel-unloader group and 34.8° in the cast group, the difference was not statistically significant (mean difference 4.6°, 95% CI: −2.0° to 11.2°; P = .168). Subtalar joint mobility, quantified as a score between 0 and 1.0, was not significantly different between the groups (P = .695).
There were no statistically significant differences in the prevalence of reported pain between the heel-unloader and cast group at any follow-up time point. At 1 year, 18.9% vs 27.0% reported residual pain (mean difference 0.0, 95% CI: −0.08 to 0.08; P = .995).
Radiographic evaluation of subtalar osteoarthritis revealed no statistically significant differences between the groups. After 12 months, asymptomatic degenerative changes of the subtalar joint were present in 41 fractures (69.5%) treated with a heel-unloader and in 35 fractures (83.3%) treated with a cast (risk difference: −13.8 percentage points, 95% CI: −30.1% to 2.4%; P = .379). In total, 4.95% (5 of 101) of all treated calcaneal fractures underwent a subtalar arthrodesis during the follow-up period. Notably, all arthrodesis cases occurred exclusively in the operative treatment group among patients who did not receive heel-unloader treatment and were indicated due to symptomatic subtalar arthritis. Subtalar arthrodesis was performed at 1 year (n = 2), 1.5 years (n = 1), 2 years (n = 1), and 5 years (n = 1) postoperatively (mean 2.1 years), with 1 case performed at an external institution.
Pressure ulcers were observed in 1 fracture in each group with no significant difference (1.7% vs 2.4%, risk difference: −0.7 percentage points, 95% CI: −6.4% to 5.0%; P = 1.00).
Two calcaneal fractures (1.4%) required reoperation. One patient of the operatively treated heel-unloader group suffered another fall with loss of position. The second patient also belonged to the surgically treated heel-unloader group and suffered an intra-articular screw displacement.
Discussion
This study demonstrates that the use of a heel-unloader orthosis after calcaneal fracture, either operatively or non-operatively treated, results in radiographically macroscopic equivalent outcomes compared with conventional immobilisation with a cast and partial weight-bearing. Importantly, the predefined equivalence margin for BA loss was met, confirming that early full weight-bearing in the orthosis does not compromise fracture stability. Notably, our primary outcome evaluates only macroscopic fracture displacement and heel height, and equivalent BA does not mean the articular joint surface itself maintained perfectly equivalent reduction.
The heel-unloader orthosis was initially introduced in 1994 as the Settner shoe, with the goal of offloading the posterior heel and enabling early mobilisation by redirecting ground reaction forces to the forefoot and midfoot. 6 Clinical evidence supporting this concept has since evolved. Kagami et al 9 demonstrated improved functional outcomes at 3 months (69.6 vs 77.2; P = .004) in patients treated with a heel-unloader orthosis compared to a cast. In addition, this study did not show a significant statistical difference in the reduction of the BA over the time of treatment (5.1 vs 5.9; P = .529). Our findings support these data by showing that mechanical stability is not inferior when early full weight-bearing is permitted in an orthosis. The significant decrease in BA observed during the first 4 weeks in both groups is consistent with previous reports, indicating that most subsidence occurs early postoperatively.3,17 Beyond this point, no further significant loss of BA was detected in both groups, which suggests that early mobilisation in the heel-unloader does not contribute to progressive deformity. This is crucial in maintaining calcaneal height and restoring subtalar joint function, both of which correlate with long-term outcomes.7,19-21 In the literature, a mean BA loss of 4.9° has been reported at the 3-month follow-up; in our cohort, the heel-unloader group demonstrated a loss of 4.1°, whereas the cast group showed a loss of 3.2°, which is consistent with current evidence.14,22
The ROM of the ankle joint and subtalar joint did not differ significantly between the heel-unloader group and the cast group, but there was a tendency for the heel-unloader group to have better ankle joint mobility than the cast group. This is consistent with previous reports that early mobilization limits the long-term effects of immobilization on ROM.10,21,23 Furthermore, subtalar joint stiffness, often a sequela of intraarticular calcaneal fractures, appears to be influenced more by fracture morphology and postoperative joint congruity than by the type of postoperative immobilization.24-26 Thus, although the heel-unloader may have biomechanical advantages in terms of load redistribution, its impact on joint mobility appears limited in this context.
Persistent pain was reported in 18.9% and 27.0% of patients at 1 year, without a statistically significant difference between groups. The rate observed in our cohort lies within the lower range of previously reported incidences up to 14.9% to 42.2%,3,27,28 where persistent pain following calcaneal fractures has been described in up to 42.4%. It should be noted, however, that the present study did not assess the need for analgesic medication, which may have provided a more comprehensive evaluation of pain-related impairment.
The incidence of radiographic subtalar osteoarthritis observed in this study falls within the broad range reported in the literature (5%-100% following calcaneal fractures). The high proportion in our cohort is partly explained by the fact that we also included asymptomatic degenerative changes of the subtalar joint in our assessment. The rate of subtalar arthrodesis (4.95%) is at the lower margin of the reported 2.8% to 47% in the current literature.1-3
Nonetheless, certain limitations should be acknowledged. This was a retrospective single-center study with a limited sample size. Although the heel-unloader was introduced as standard treatment care in 2018, unmeasured biases related to treatment era or rehabilitation protocols cannot be excluded. Moreover, functional outcome measures such as AOFAS or return-to-work times were not the focus of this equivalence analysis but are currently under investigation in a subsequent follow-up study. Radiographic measurements were performed by a single senior attending foot and ankle surgeon; interobserver and intraobserver reliability were not formally assessed, which should be considered when interpreting the radiographic findings. A major limitation of our study is the exclusive reliance on lateral radiographs to measure BA without the use of post-operative CT scans or Broden view radiographs. CT scans (coronal and axial views) are considered the gold standard for verifying whether the articular cartilage surface is flush. Furthermore, other complementary lateral radiographic measurements, such as the angle of Gissane, which helps assess the downward slope of the posterior facet, were not used to evaluate the joint surface. In addition, the study population was heterogeneous, as both operatively and non-operatively treated calcaneal fractures were analyzed together. Although this reflects real-world clinical practice, differences in baseline fracture stability and mechanical support through internal fixation may influence tolerance to early weight bearing and limit direct comparability between subgroups.
In conclusion, the heel-unloader orthosis appears to provide a safe alternative to traditional immobilization in a cast following calcaneal fracture. It allows early full weight-bearing without increasing the risk of macroscopic fracture displacement, as reflected by equivalent loss of BA and similar clinical outcomes. These findings indicate that the heel-unloader could represent a reasonable option within post-fracture management, especially in clinical situations where early mobilisation is desirable.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114261434237 – Supplemental material for Early Full Weight-Bearing After Calcaneal Fracture Using a Heel-Unloader Orthosis: Equivalent Radiographic Outcomes Compared to Traditional Cast Treatment
Supplemental material, sj-pdf-1-fao-10.1177_24730114261434237 for Early Full Weight-Bearing After Calcaneal Fracture Using a Heel-Unloader Orthosis: Equivalent Radiographic Outcomes Compared to Traditional Cast Treatment by Verena Hecht, Fabian Krause and Helen Anwander in Foot & Ankle Orthopaedics
Footnotes
Ethical Considerations
Ethical approval for this study was obtained from Ethikkommission Bern (approval ID 2023-00064).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was financially supported by Orthoteam.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Disclosure forms for all authors are available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.