
Abstract
Background:
To determine the functional and radiographic outcomes, as well as complications, in patients diagnosed with Charcot neuroarthropathy (Sanders/ Frykberg types II, III, and IV; Eichenholtz stages II and III) treated with 1-stage arthrodesis using screw-based superconstructs, with a 1-year follow-up.
Methods:
Patients treated with the Caldiño method for Charcot neuroarthropathy who underwent 1-stage arthrodesis (panastragalodesis and triple arthrodesis) using screw-based superconstructs between January 2023 and August 2024 were followed. The visual analog scale (VAS) for pain were assessed preoperatively and postoperatively, clinical results and complications were analyzed along with patient satisfaction and the degree of radiographic consolidation at 1-year follow-up.
Results:
Twenty-four patients were included, with equal sex distribution and a mean age of 54.5 years. The right foot was affected in slightly more than half of cases. Panastragalodesis was performed in the majority of patients, whereas the remaining patients underwent triple arthrodesis with preservation of the tibiotalar joint. A significant postoperative reduction in pain was observed, with mean VAS scores decreasing from 6.2 preoperatively to 0.7 at final follow-up. Radiographic evaluation demonstrated advanced consolidation in most patients. Minor postoperative complications were observed in fewer than half of the cohort and consisted primarily of superficial wound complications, all of which were managed conservatively and resolved within the early postoperative period.
Conclusion:
In this case series, screw arthrodesis, using superconstruction principles for the management of Charcot neuroarthropathy, was associated with satisfactory radiographic consolidation at 1-year follow-up, a substantial reduction in pain between pre- and postoperative periods, and the restoration of a stable, aligned, and pain-free plantigrade foot in patients with Eichenholtz stages II and III Charcot neuroarthropathy. Although complications did occur, minor wound-related complications were the most frequent and could be managed with conservative treatment, without the need for reintervention. Screw arthrodesis is a viable limb-sparing option in selected patients with advanced Charcot deformity.
Level of Evidence:
Level IV, retrospective case series.

Introduction
Charcot neuroarthropathy was first described in 1868 by Jean-Martin Charcot as a progressive joint disorder, originally described in patients with syphilis; however, today most commonly associated with type 1 and type 2 diabetes in approximately 75% of patients. Other associated conditions include HIV infection, amyloidosis, alcoholism, renal dialysis, metabolic bone diseases, and various peripheral neuropathies.1 -9
The disease is characterized by progressive bone and joint destruction mediated by an inflammatory cascade that increases proinflammatory cytokines and osteoclastic activity, leading to fractures, joint dislocations, and severe deformity.1,3,6,9 This process is often triggered by minor trauma, infection, or surgical intervention.2,4,9 Although the pathophysiology is multifactorial, 2 main theories have been proposed: repetitive microtrauma related to neuropathy and a neurovascular mechanism involving hyperemia and accelerated bone resorption.4,10 -12
Peripheral neuropathy in patients with diabetes should be understood as a progressive continuum rather than an on-off phenomenon. Loss of protective sensation, as detected by the 5.07 Semmes-Weinstein monofilament, reflects advanced neuropathic involvement and is typically associated with long-standing diabetes, often exceeding 10 years. In this context, approximately 8.5% of patients with established peripheral neuropathy progress to Charcot neuroarthropathy.1,6 Reported prevalence ranges from 0.1% to 7.5% among patients with diabetic foot ulcers 4 and 0.3% in the general diabetic population, 13 with an average incidence of 1.06% to 1.97% in patients with type 1 diabetes and 0.42% to 0.60% in type 2 diabetes. 14 Bilateral involvement has been reported in up to 9% of cases. 15 Despite its clinical relevance, up to 95% of cases remain undiagnosed. 2
Diagnosis is primarily clinical and typically occurs 8-12 years after the onset of diabetes.4,16,17 The main treatment goals are to halt disease progression, achieve a stable and plantigrade foot, prevent ulceration, restore ambulation, and preserve the limb.11,15,18,19 Conservative management is preferred in the acute phase or in patients with high surgical risk, whereas surgical intervention is generally reserved for chronic stages with established deformity.1,3,11,20 Many authors recommend surgery during Eichenholtz stage II or III, when complication rates are lower and functional outcomes are more favorable. 11
The main indications for surgery are nonplantigrade deformity, chronic osteomyelitis, or pain, which in these patients would be interpreted as a pseudoarthrosis of their neuropathic process. 21 Surgical strategies include resecting infected bone, exostectomy, deformity correction, and limb salvage procedures.8,9,21 Screw-based arthrodesis using superconstruct principles has demonstrated favorable radiographic consolidation and functional outcomes, supporting its role as a viable limb salvage option.6,7,11
The purpose of this study was to evaluate the functional and radiographic outcomes of patients with Charcot neuroarthropathy in Eichenholtz stages II and III treated with triple arthrodesis or panastragalodesis using screw-based superconstruct fixation.
Methods
An retrospective case series study was conducted including 24 patients diagnosed with Charcot neuroarthropathy (Sanders/ Frykberg 21 types II, III, and IV; Eichenholtz 22 stages II and III) who underwent either triple arthrodesis or panastragalodesis using screw-based superconstructs, between January 2023 and August 2024. Eligible patients were required to have complete electronic medical records and a strict follow-up for at least 1 year. Patients lost to follow-up (2 patients), with incomplete records, or treated with other fixation methods were excluded.
No sample size calculation was performed, as all patients meeting the inclusion criteria during the study period were enrolled. Patients diagnosed with Charcot neuroarthropathy who underwent arthrodesis were selected, totaling 29 patients. Of these, 3 were excluded because they required fixation with a nail and intramedullary plate. Of the 26 patients who underwent screw fixation and remained in the study, 2 were excluded for discontinuing medical treatment in the first few months postoperatively. Therefore, 24 patients included in the study met the inclusion criteria and had a minimum follow-up of 1 year (Figure 1).

Patients diagnosed with Charcot neuroarthropathy who underwent arthrodesis were selected, totaling 29 patients. Of these, 3 were excluded because they required fixation with a nail and intramedullary plate. Of the 26 patients who underwent screw fixation and remained in the study, 2 were excluded for discontinuing medical treatment in the first few months postoperatively. Therefore, 24 patients included in the study met the inclusion criteria and had a minimum follow-up of 1 year.
Of these, 12 patients (50%) were male and 12 (50%) were female, with a mean age of 54.4 years (range, 25-67). The right foot was affected in 13 cases (54.2%) and the left in 11 (45.8%).
Patients were initially followed in the Foot and Ankle Service at the time of clinical diagnosis of Charcot neuroarthropathy, which was based on increased local temperature, edema, erythema, and radiographic evidence of bone destruction, being classified into Einchelhotz 22 stages I, II, and III. Baseline assessment included the visual analog scale (VAS) for pain score, as well as radiographic classification using the Sanders/Frykberg 21 staging system (Figure 2). Subsequently, patients were managed with the Caldiño method,18,19 consisting of total contact corrective casting with monthly follow-up in an average of 3 months, in addition to comprehensive management of comorbidities and metabolic control by internal medicine.

Preoperative radiographic and clinical images of a case. (A) Preoperative anteroposterior and lateral radiographic images of Charcot neuroarthropathy. (B) Clinical image of varus deformity in a patient with Charcot neuroarthropathy. (C) Lateral clinical image of a patient with Charcot neuroarthropathy.
After completing the first stage of Caldiño method,18,19 which averaged 3 months of treatment with full-contact corrective casts to achieve maximum reduction and joint alignment, surgical treatment was performed using superconstructs 7 with solid 4.0-mm or 6.5-mm screws. Surgery was offered to patients with severe deformities, unstable feet or ankles, or deformities affecting gait. All procedures were performed by the same experienced foot and ankle surgeon using a standardized technique. The choice between triple arthrodesis and panarthrodesis was individualized based on the affected region (according to the Sanders/Frykberg classification) and the clinical deformity. Triple arthrodesis was chosen for patients with midfoot involvement and a preserved talocrural joint, whereas panarthrodesis was chosen for patients with hindfoot involvement and talocrural joint involvement. A single lateral approach of approximately 5 cm with fibular osteotomy was used to access the involved joints. The articular surfaces were removed via oblique osteotomies according to the deformity, allowing for alignment and reduction, achieving sagittal and coronal alignment. All procedures were performed with solid stainless steel screws (4.0- or 6.5- mm) inserted percutaneously, following the principles of Superconstructs 7 : extending fixation beyond the injured area, shortening the limb to facilitate deformity reduction, using stronger and stiffer devices, and maximizing the mechanical function of the implants. In addition, 4.0- or 6.5-mm screws were used for arthrodesis of the calcaneocuboid and talonavicular joints, and 6.5-mm screws were used for the subtalar and tibiotalar joints, in a number of 2 to 3, depending on the intraoperative clinical stability obtained after placement of the second screw. Follow-up was conducted as follows: during the first week, the surgical wounds were inspected, and the patient was kept in an anti-edema dressing. From week 1 to week 4, the first full-contact cast was applied, and the sutures were removed. From week 4 to week 8, the second full-contact cast was applied, followed by a third cast from week 8 to week 12. After the 3 postoperative casts were completed, immobilization was changed to a long walking boot, with partial weight-bearing beginning on the operated limb at 12 weeks (Figure 3). The long walking boot was removed on observation of consolidation and clinical stability during examination, between 16 and 20 weeks postsurgery, at which time patients were advised to begin full weightbearing.
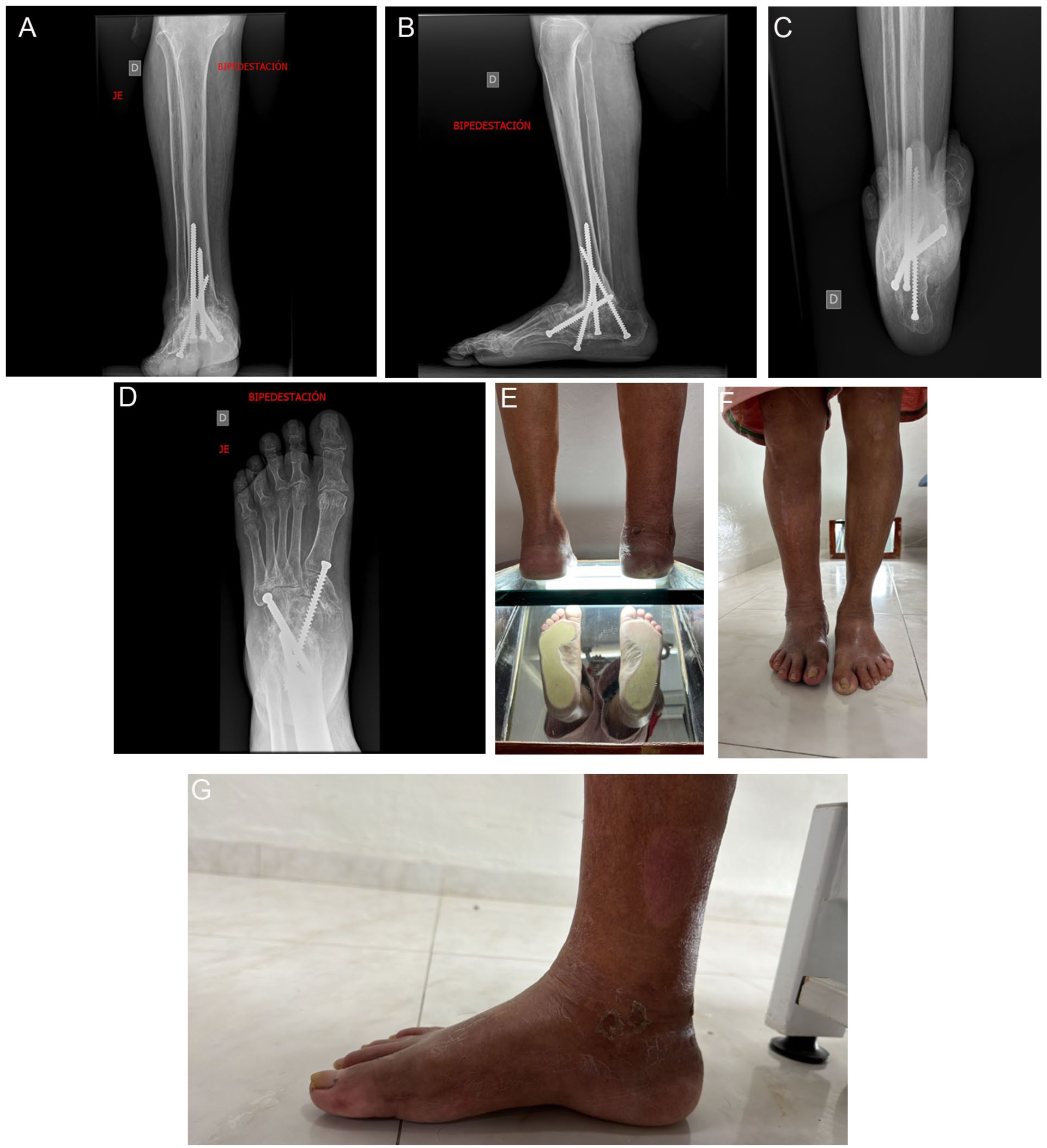
Preoperative radiographic and clinical images of a case. (A) Postoperative Saltzman projection radiograph. (B) Postoperative lateral radiograph. (C) Postoperative dorsoplantar radiograph. (D) Postoperative anteroposterior radiograph. (E) Clinical image of medial postsurgical wound. (F) Clinical image of lateral postsurgical wound. (G) Postoperative plantar clinical image.
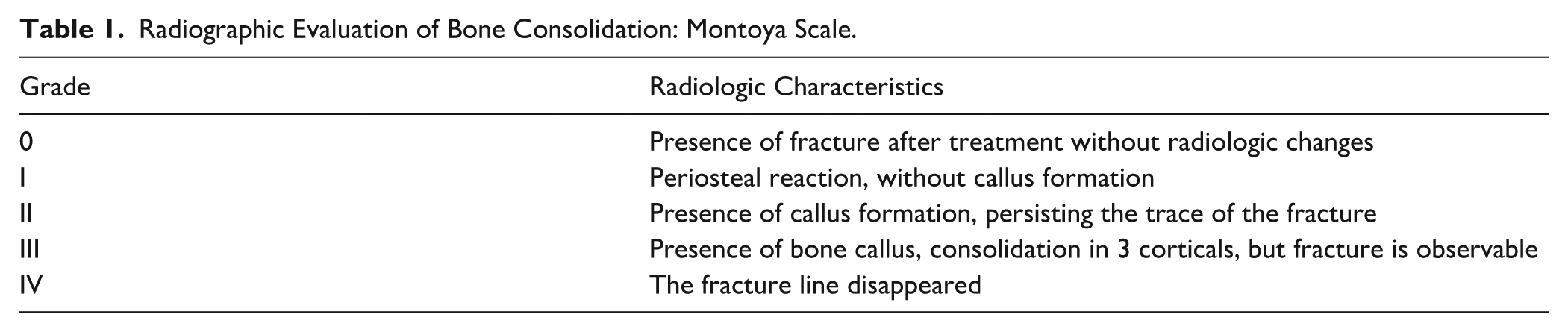
The VAS 23 was used for evaluating pain; this scale was used as a subjective and standardized method for measuring pain; however, it should be considered with caution because patients with diabetic foot may present alterations in perception as well as during the evolution of the disease, along with patient satisfaction using a Likert scale 24 (1 = not satisfied, 2 = slightly satisfied, 3 = neutral, 4 = very satisfied, 5 = completely satisfied) at the 1-year postoperative follow-up. Radiographic follow-up was performed at 3, 6, and 12 months, evaluating consolidation using the Montoya radiographic scale 32 Table 1. These findings guided therapeutic decisions regarding progression of weightbearing on the operated limb starting at 3 months postoperatively. The degree of radiographic consolidation at 1 year was recorded as the final consolidation outcome. All these measurements were performed by a single expert in foot and ankle surgery.
Radiographic Evaluation of Bone Consolidation: Montoya Scale.
Statistical Analysis
A database was created using the Agemed electronic records of the 24 patients and processed with IBM SPSS Statistics® version 25.0 (IBM®) to calculate standard descriptive statistics, including measures of central tendency, variance, frequencies, and proportions. Mean differences for VAS were analyzed using nonparametric Wilcoxon (Z test) for 2 paired variables as 2 related samples, considering a P value ≤.05 statistically significant, with a 95% CI.
Results
Demographic Results
The underlying etiology was type 2 diabetes mellitus in 87.5% (n = 21), type 1 diabetes mellitus in 8.3% (n = 2), and alcoholism in 4.2% (n = 1) (Table 2).
Demographic Information.

Abbreviations: DM, diabetes mellitus; DM1, diabetes mellitus type 1; DM2, diabetes mellitus type 2; HbA1c, glycated hemoglobin.
Unless otherwise noted, values are % (n).
Patients with diabetes mellitus had a mean of evolution of the disease of 16.83 years, ranging from 5 to 34 years.
Associated comorbidities were evaluated in all patients, with systemic arterial hypertension being the most common, observed in 37.5% (n = 9), followed by chronic kidney disease (CKD) in 8.3% (n = 2).
Preoperative glycated hemoglobin (HbA1c) was obtained for all patients as a marker of metabolic control, with a mean value of 8.67% (range, 5.50–12.20%), confirming poor preoperative metabolic control in this population.
As part of the described preoperative treatment protocol, patients were treated with total contact corrective casts. Of the 24 patients, 16 (66.7%) required three corrective casts, each lasting 1 month; 2 (8.3%) did not require casts due to rigid and irreducible deformities; and 6 (25%) required more than 3 casts, with an average of 4, because of persistent activation of the neuroarthropathy after the third total contact cast.
For classification of Charcot neuroarthropathy, 2 scales were used. According to the anatomical Sanders/Frykberg classification, 21 most cases were located in regions III and IV (37.5%), followed by regions II and III (29.2%), and region III alone (25%). Using the Eichenholtz classification, 22 50% of patients were in stage III, which corresponds to the underdiagnosed clinical and radiographic presentation of this condition (Table 3). Most patients showed radiographic signs of consolidation in previously destroyed areas; however, they presented with evidence of instability, along with significant residual deformities that required surgical treatment.
Distribution of Cases According to the Sanders/Frykberg and Eichenholtz Classifications.

Clinical and Radiographic Results
Of the 24 patients, 75% (n = 18) underwent panastragalodesis (tibiotalar, talonavicular, subtalar, and calcaneocuboid joints), and 25% (n = 6) underwent triple arthrodesis (talonavicular, subtalar, and calcaneocuboid joints), preserving mobility of the tibiotalar joint. Among the patients treated with triple arthrodesis (n = 6), 12.5% also underwent medial column arthrodesis, and 8.4% (n = 2) required Lisfranc joint arthrodesis because of instability of these joints.
Pain was evaluated with the VAS pre- and postoperatively. The mean preoperative VAS score was 6.2 (±1.95), which decreased to 0.7 (±1.13) postoperatively, representing a statistically significant improvement (Z = −4.216; P < .001).
Radiographic evaluation demonstrated grade IV consolidation in 79.2% of patients and grade III consolidation in 16.6%. Only 1 case (4.16%) of asymptomatic nonunion was reported, associated with hardware fatigue, which did not require reoperation because the deformity was corrected, resulting in a plantigrade foot, and it was stabilized with an external orthosis.
After 1 year of follow-up, patient satisfaction with the surgery was assessed using the Likert scale. 24 Overall, 70.8% of patients were completely satisfied, including the patient diagnosed with asymptomatic pseudoarthrosis, whereas 29.2% were very satisfied; none expressed dissatisfaction with their clinical or functional results. At the end of the follow-up period, 100% of patients were able to walk independently.
Complications
Postoperative minor complications were observed in 45.8% of patients (11/24). Among these, 20.8% (5/24) developed superficial infections and 20.8% (5/24) experienced delayed wound healing. All were managed in the outpatient clinic with standard dressings and wound care, without the need for surgical reintervention, and resolved within an average of 3.8 months. In addition, 4.2% (1/24) of patients experienced implant fatigue because of asymptomatic pseudoarthrosis, which did not require surgical reintervention.
Discussion
Charcot neuroarthropathy most frequently affects the midfoot and hindfoot, leading to progressive deformity, instability, and substantial impairment of function and quality of life.⁴ In advanced stages, surgical reconstruction is often required to restore alignment and achieve a stable, plantigrade foot that allows for ambulation and reduces the risk of ulceration, infection, and amputation.15,18 Despite these shared goals, the heterogeneity of the deformities and the progression of the disease make it difficult to standardize a single surgical approach or fixation method, and therefore multiple fixation strategies have been described.
In this case series, reconstruction was performed using screw arthrodesis following the principles of superconstructs. 7 The rationale for this approach lies in achieving stable internal fixation that allows for adequate consolidation, minimizing surgical morbidity, and achieving limb salvage. Compared with techniques that combine intramedullary nails, plates, and screws, screw-only fixation allows for multiaxial compression of the affected joints, preserves bone, and limits soft tissue dissection. These characteristics are particularly relevant in patients with Charcot neuroarthropathy, who often present with compromised soft tissues, poor bone quality, and an increased risk of wound complications.
Although intramedullary nails and plate fixation provide rigid fixation, they are associated with larger surgical incisions, greater implant volume, and potential stress on osteopenic bone. In contrast, screw superconstructs 7 extend fixation beyond the injured area, maintaining a less invasive internal fixation strategy, consistent with the biomechanical principles proposed for Charcot reconstruction. 7 The favorable radiographic consolidation and functional outcomes observed in this series suggest that, in selected patients, screw arthrodesis can achieve results comparable to those described with more rigid fixation methods.
The etiology of Charcot neuroarthropathy in our cohort was predominantly diabetes mellitus, consistent with previous reports. 25 The long duration of diabetes and poor metabolic control observed in our patients are comparable to those described by Hester et al, 10 Siebachmeyer et al, 26 and Regauer et al. 27 Although metabolic control is an important factor in surgical planning and postoperative risk stratification, it was not the primary focus of this study. Rather, these findings reflect the typical high-risk population in Charcot neuroarthropathy and underscore the need for fixation strategies that balance stability with surgical morbidity.
The complication rate observed in this study is consistent with that reported in the literature. Bajuri et al 11 reported complication rates of 37.5%, whereas Regauer et al 27 described rates close to 89% in patients treated with superconstructs. Gong et al 28 reported lower complication rates (5%-9%) with screw-based arthrodesis, whereas Wang et al 3 observed higher rates of both minor and major complications after Charcot arthrodesis. Importantly, in our series, complications were predominantly minor and superficial, did not compromise fixation or fusion, and were successfully managed with conservative treatment without requiring further surgery during our follow-up.
The clinical outcomes for pain, with significantly lower postoperative VAS scores, were comparable to those reported by Bajuri et al, 11 Gong et al, 28 and Chraim et al, 29 the latter using retrograde fixation with an intramedullary nail. These comparable results suggest that screw arthrodesis can achieve similar short-term clinical outcomes without the need for more extensive implants. Limb preservation was achieved in all patients, consistent with previous reports on the use of internal fixation systems.11,26,30 The consolidation rate observed at 1 year (79.2%) is comparable to that reported by López-Gavito 16 and Vasukutty 30 and is consistent with consolidation rates described using other internal fixation techniques.15,25 Waldecker et al 15 reported favorable results with screw osteosynthesis, including higher fusion and ulcer remission rates compared with the external fixation methods described by Fragomen et al. 31
Limitations of this study include its retrospective design, small sample size, lack of a control group, and relatively short follow-up period. However, this case series demonstrates that screw arthrodesis using superconstruct principles can provide stable fixation, acceptable consolidation rates, and significant clinical improvement in patients with advanced Charcot neuroarthropathy. Taken together, these findings support screw arthrodesis as a viable and less invasive limb-sparing option in selected patients, offering results comparable to other fixation methods while potentially reducing surgical morbidity.
Limitations
The limitations of this study included the relatively small number of patients and the follow-up period, which did not allow long-term evaluation of late complications, ulcer recurrence, or delayed implant failure. A multicenter randomized controlled trial would be the optimal approach to standardize the best fixation system for this population and to achieve more robust functional outcomes. Among the limitations, it was found that the intermediate evaluations of the patients were performed at different times, so only the presurgical measurements and the 1-year follow-up are reported. There was only 1 expert evaluator for the clinical and radiographic measurements.
Conclusions
Surgical treatment of Charcot neuroarthropathy remains a challenge for foot and ankle surgeons because of compromised bone quality and the high risk of postoperative complications. Given these limitations, the results of this case series suggest that single-stage arthrodesis with screw fixation can provide reliable stabilization and correction of deformity in patients with stage II and III Eichenholtz disease.
In our cohort, screw arthrodesis was associated with high rates of radiographic consolidation, marked pain improvement, and adequate clinical correction, resulting in plantigrade feet that allowed for ambulation. Notably, all limbs were salvaged during the follow-up period. Although postoperative complications were relatively frequent, they were predominantly minor and did not compromise fixation or consolidation, resolving with conservative management.
From a technical perspective, screw fixation of the superstructure offers several practical advantages, such as internal fixation with minimal soft tissue disruption, the ability to generate multidirectional compression at the joints, and the possibility of avoiding bulkier implants or prolonged external fixation. These characteristics can be advantageous in patients with soft tissue damage or when minimizing surgical morbidity is a priority.
The findings of this study should be interpreted considering its limitations; however, this case series contributes to the growing body of evidence supporting screw arthrodesis as a viable limb-sparing strategy in selected patients with advanced Charcot neuroarthropathy. Further prospective studies with larger cohorts and longer follow-up are needed to better define patient selection criteria and compare fixation strategies in this complex population.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114261434007 – Supplemental material for Radiographic and Clinical Outcomes in Patients With Charcot Neuroarthropathy Undergoing 1-Stage Screw Arthrodesis: 1-Year Follow-up
Supplemental material, sj-pdf-1-fao-10.1177_24730114261434007 for Radiographic and Clinical Outcomes in Patients With Charcot Neuroarthropathy Undergoing 1-Stage Screw Arthrodesis: 1-Year Follow-up by Tamara Hernádez Bermúdez, Itzel Caldiño Lozada and Ramón Ignacio Esperón Hernández in Foot & Ankle Orthopaedics
Footnotes
ORCID iDs
Ethical Considerations
Ethical approval for this study was obtained from Research Committee of the Orthopedic Hospital, Mexican Red Cross IAP, Approval Number COFEPRIS 20 CI 31 050 016.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Disclosure forms for all authors are available online.