
Abstract
Background:
First metatarsophalangeal (MTP) arthrodesis can effectively alleviate pain and correct deformity of the great toe but may introduce unique limitations to an active patient population, particularly in alpine-specific sports including Nordic and alpine skiing, snowboarding, hiking, trail running and biking. Limited literature evaluates return to these specific activities after first-MTP arthrodesis. This study aims to better define the ability to return to physical activity, with a focus on alpine sports and footwear modifications.
Methods:
Adults undergoing MTP arthrodesis with ≥1-year follow-up at a single academic institution were retrospectively reviewed. Demographic data, surgical complications, and radiographic union were recorded. A custom sports questionnaire was administered preoperatively and postoperatively across >20 sports, including outdoor and alpine sports, to assess return to activity. Paired t tests compared pre- to postoperative changes in patient-reported outcomes, with significance set to P <.05.
Results:
The mean age was 58.8 years, and 57.3% were female. Ninety-six percent (43/45) of patients returned to sport by 12 months postoperatively, whereas 24.4% required more than 12 months to reach their maximum activity level. Nordic and alpine skiers and snowboarders were all able to return to the same or higher level of sport, but nearly half (40%) required boot modifications. Similarly, 42% of all patients in this study required some level of shoe modification for their respective sport.
Conclusion:
First-MTP arthrodesis supports high return-to-sport rates, including demanding alpine activities including skiing, snowboarding, and hiking. Up to 1 year is often required to reach maximum performance. Patients should be counseled on the potential need for footwear modification after surgery. These findings outline guidance for counseling of highly active patient populations. Further studies can help elucidate which factors contribute to the lack of return to sport for specific patients and sports.
Level of Evidence:
Level IV, retrospective case series
Introduction
Degenerative arthritis of the first metatarsophalangeal (MTP) joint, commonly known as hallux rigidus, is the most common arthritis affecting the foot with a typical age of onset between 43 and 50 years.1,2 First-MTP arthrodesis is a well-established surgical option for patients with first-MTP arthritis, hallux valgus, and hallux varus. First-MTP arthrodesis is associated with high rates of union, reported to be 90% to 100% in the literature, along with marked improvements in functional outcome measures.3 -5
Despite high rates of success and reliable pain relief, many active patients and athletes are hesitant to undergo first-MTP arthrodesis out of concern for potential limitations of returning to activity and sports. Prior studies have shown excellent and consistent return to activities of daily living but variable return to sports and physical activity after first-MTP arthrodesis. 3 It is imperative to appropriately counsel patients on the likelihood of success and return to their desired level of activity after a procedure. Furthermore, educating patients on the possible need for modifications to their shoe wear or sport-specific gear, such as ski or snowboard boots and hiking or running shoes, should be part of preoperative counseling. The geographic location of our academic center serves a patient population with a high prevalence of alpine activity participation, providing a unique opportunity to evaluate these activities in our analysis.
To our knowledge, no studies have evaluated the need for shoe wear or sports gear modification after first-MTP arthrodesis, specifically in alpine athletes. We aimed to define a clear timeline for return to sport and to evaluate specific parameters for expected return to sports such as mileage, speed, incline, and terrain difficulty. This expands on prior studies, which have used generalized descriptions of return to sports.1,6 The goal of this study was to better define the ability to return to sport, the level of return to sport, and the need for footwear or gear alterations after first-MTP arthrodesis, with an emphasis on alpine sports. We hypothesized that most patients would return to their desired level of physical activity but that many would require footwear modifications.
Materials and Methods
Following institutional review board approval, all MTP arthrodesis operations between 2015 and 2022 at a multicenter academic institution were identified using Current Procedural Terminology (CPT) code 27850. Patients >18 years of age and with ≥1-year clinical follow-up were included for analysis. Exclusion criteria included concomitant forefoot/hindfoot procedures and revision surgeries. Patients with a nonunion or surgical site infection requiring repeat operation were included in the descriptive summary of our cohort, but because our goal was to evaluate participation in activity after successful union, they were excluded from subsequent analysis.
Demographic data, surgical details, and postoperative complications were recorded by retrospective chart review. When available, preoperative radiographs were used to assess osteoarthritis grade in accordance with the Coughlin and Shurnas 2 radiographic classification. Two foot and ankle fellowship–trained orthopaedic surgeons assessed and agreed on radiographic bony fusion.
Sports Questionnaires
A custom sports questionnaire was administered to qualifying patients via email or verbally over a phone call. Responses were collected through a HIPAA-compliant electronic data capture system (REDCap).
Return to sports and physical activity was evaluated through a retrospective sports/activity specific questionnaire, which was modified from a previously developed version that has been used as an assessment tool following foot and ankle surgery.1,7 This questionnaire asked patients about their preoperative and postoperative participation in more than 20 common and alpine-specific sporting activities including running, biking, hiking, alpine and Nordic skiing, and snowboarding. Patients rated their perceived level of difficulty and participation compared to before surgery on a 5-point Likert scale. They were also surveyed on whether they required any shoe wear or equipment modifications, the amount of time required for return to activity, and the amount of time required for return to maximum level of activity.
Several sports prompted more specific questions. For road running and walking, patients were asked if they were able to achieve the same mileage and speed after surgery. For trail running, biking, and hiking, patients were asked about mileage, speed, and level of incline. For skiing and snowboarding, patients were asked if they were able to traverse terrain of the same difficulty after surgery.
Statistical Analysis
Statistical analysis was performed using the R statistical package (v. 4.2.1). The cohort was descriptively summarized. Categorical variables were reported as frequencies and proportions, and numerical variables were reported as mean and SD. Survey responses were tabulated and similarly reported. Patients with incomplete surveys and missing data were excluded from analysis. Paired t tests were used to compare differences in preoperative patient-reported outcomes (PROs) to measures collected in the follow-up survey. A P value <.05 was considered significant.
Results
Patient Population
A total of 96 patients met the inclusion criteria. The mean age of patients at the time of surgery was 58.8 years (SD ± 10.6), and 57.3% (n = 55) of the patients were female (Table 1). The most common indication for first-MTP arthrodesis was hallux rigidus (70.5%, n = 67), and most patients (61.5%, n = 59) had Coughlin and Shurnas grade 3 or 4 MTP joint arthritis at the time of surgery. The mean length of follow-up was 3.25 (±1.9) years.
Patient Demographics (N = 96).

MTP arthrodesis was performed by 4 different foot and ankle fellowship–trained orthopaedic surgeons. Operative technique varied by surgeon, but all constructs included either a plate-and-screw construct or screw-only fixation. Postoperative protocols also varied between surgeons, with most restricting weightbearing for 2-4 weeks and then allowing progressive and protected weight bearing until 6-8 weeks.
Of the 96 patients included in demographic review, 3 patients (3.1%) had nonunion or delayed union, and 5 patients (5.2%) developed a surgical site infection. Three of the 8 patients with nonunion or infection required surgical intervention, and these patients were excluded from further analysis.
Sports and Physical Activities
Forty-five patients (48.4% of eligible patients) responded to the survey. Most respondents participated in outdoor recreational activities including walking, hiking, and road biking followed by alpine skiing and road running (Table 2). Eleven patients (24.4%) reported an inability to continue participating in 1 or more of their preferred sports. Road running (n = 4) and trail running (n = 3) had the highest incidence of inability to return to sport. There was no difference (P = .94) in age between patients able to return to sport after surgery (56.9 years) and those who could not return to sport (56.8 years). There was no significant difference (P = .4) in the age of patients able to return to running after surgery (49.5 years) and those not able to return (53.8 years).
Sport/activity participation before and after surgery and the rate of shoe wear modification. Percentage of patients unable to participate in sport following surgery and those needing shoe wear modifications represent total participants in each respective sport prior to surgery.
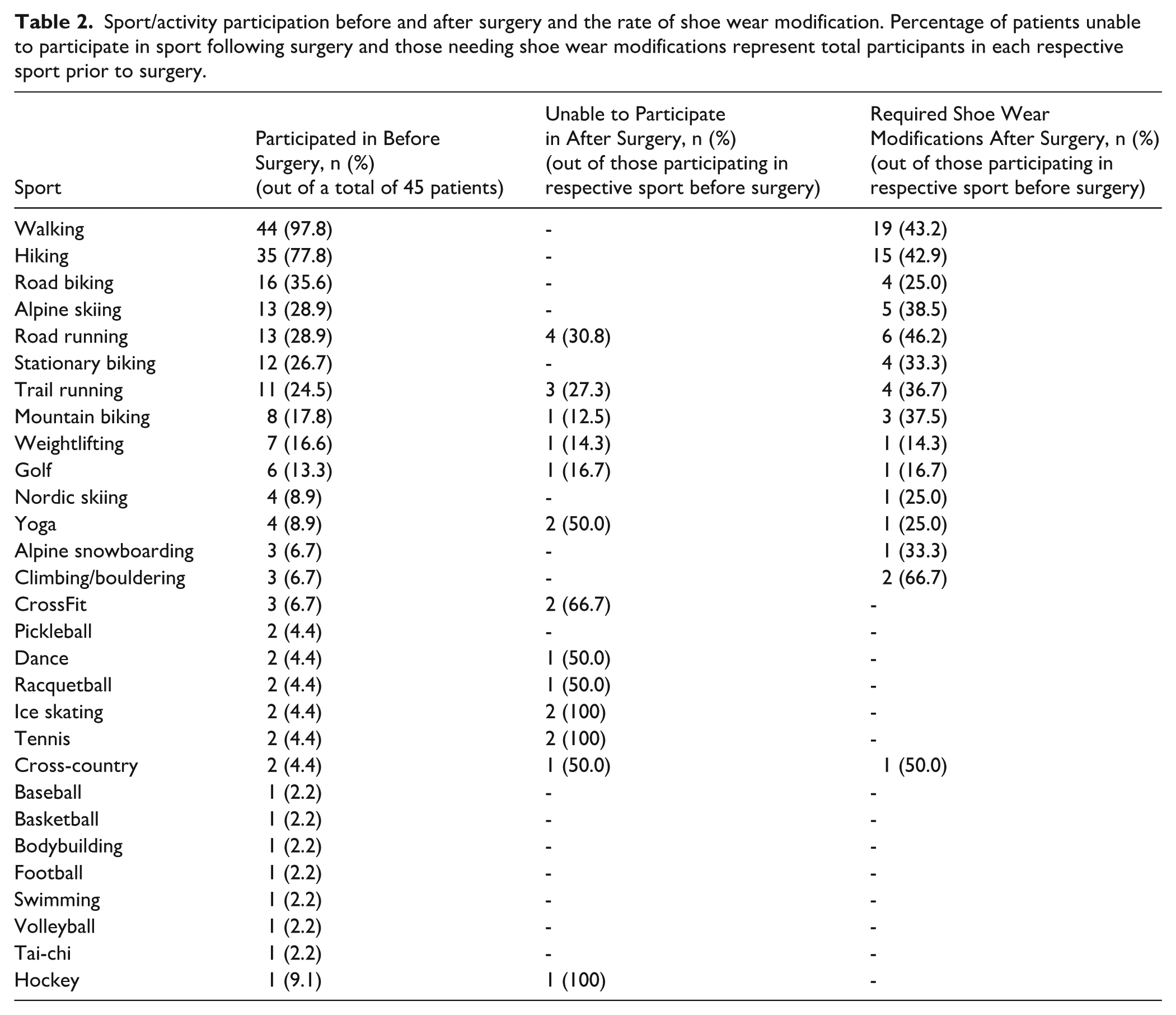
Shoe wear or gear modifications were reported for 42.2% of patients (n = 19) after surgery (Table 2). The most reported modifications were the need for a custom orthotic (n = 6, 13.3%) or wearing a shoe with a bigger toe box (n = 6, 13.3%). Other modifications were using a better-quality or cushioned shoe (n = 4, 8.9%), and a flatter/stiffer shoe (n = 1, 2.3 %). Two patients (10.5%) stated a need for modifications of ski boots but not regular shoes.
Functional postoperative changes regarding speed, mileage, and incline for walking, hiking, running and biking are described in Table 3. Most patients had similar or increased postoperative function. Postoperative mileage for walking, road running, and hiking was the parameter most likely to increase, with 18 hikers (52%) noting an increase in mileage after surgery. Speed for walking, road running, hiking, and trail running was the parameter most likely to decrease postoperatively, with road running speed decreasing for 6 runners (50%).
Postoperative Function Following Metatarsophalangeal Fusion Relative to Preoperative Function for Common Outdoor Recreational Sports. a

Percentages are out of each row total, respectively.
Most patients (68.9%, n = 31) returned to their preoperative level of activity by 6 months after surgery (Figure 1). Eleven patients (24.4%) were able to return to activity within the first month, whereas most patients returned to their preferred activities between 3 and 6 months (44.4%, n = 20). Reaching maximum activity level required greater than 12 months postoperatively for 24.4% of patients (n = 11).
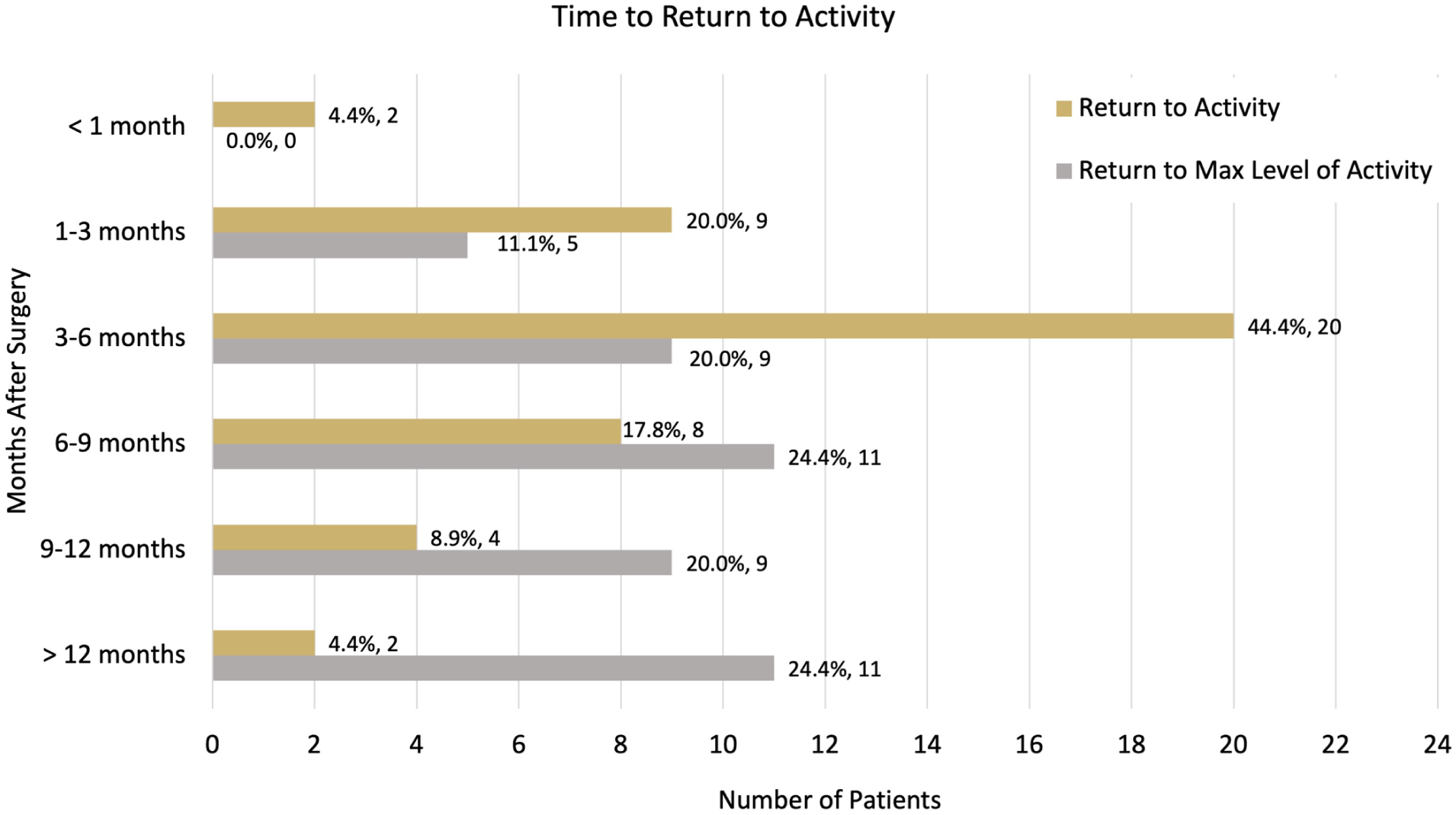
Length of time required for return to activity and return to maximum level of activity following metatarsophalangeal arthrodesis.
Thirty-two patients (71.1%) reported an improved or much improved level of participation after surgery, whereas 4 (8.9%) reported impaired participation. Thirty-five patients (77.8%) reported less perceived difficulty in their activity or sport compared with their preoperative state, and 3 (6.7%) reported more difficulty after surgery (Figure 2).

Postoperative changes in the level of participation (A) and the perceived difficulty (B) in patients’ preferred sport or activity following metatarsophalangeal fusion.
Thirty-five patients (77.8%) were satisfied or very satisfied with their surgery with regard to return to physical activity, and 10 (22.2%) were neutral, unsatisfied, or very unsatisfied with return to physical activity (Figure 3). The one patient very unsatisfied with their return to physical activity hiked and walked post fusion but required an orthotic and cited their dissatisfaction with the lesser toes not functioning as well after surgery.
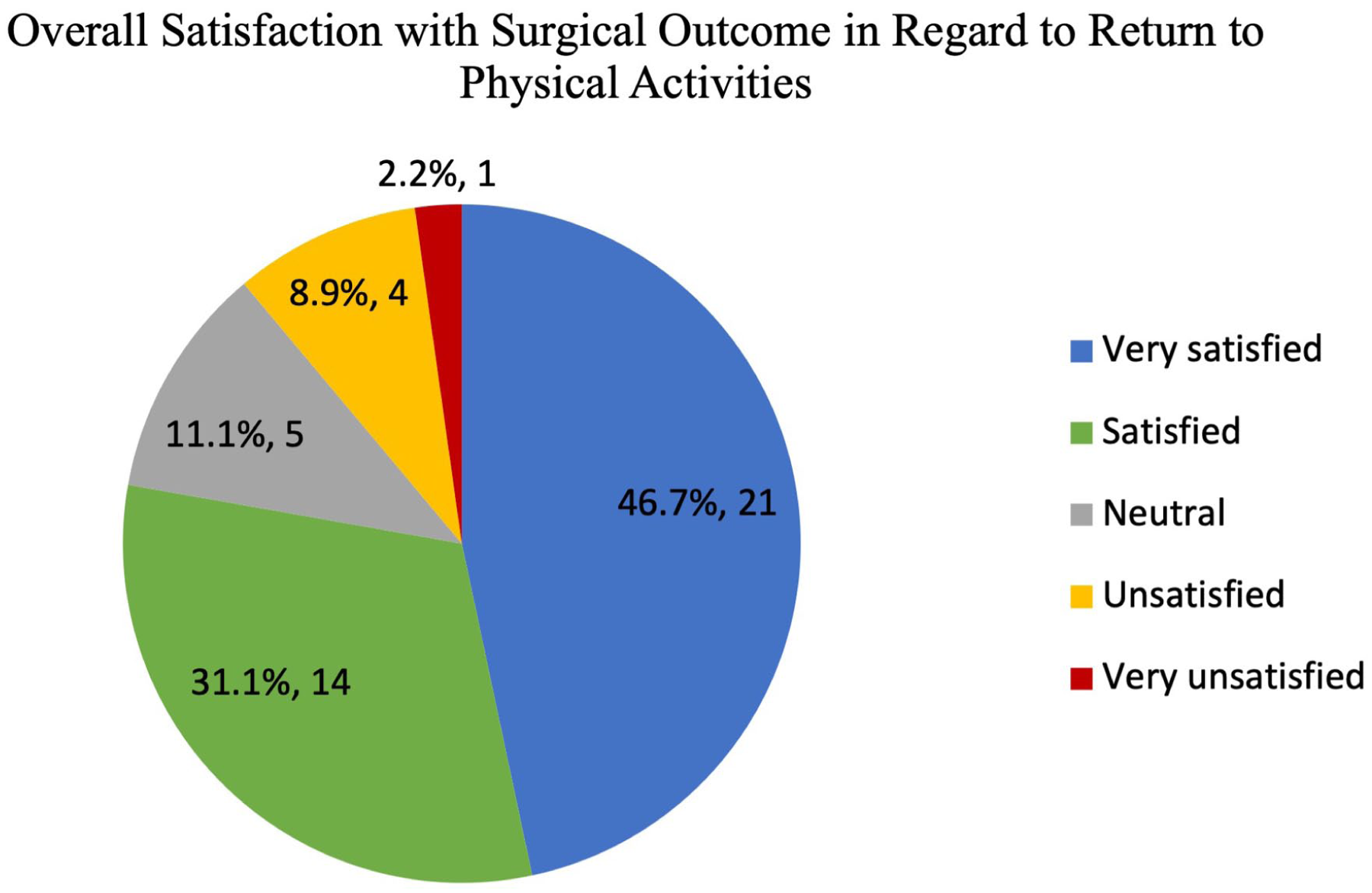
Level of patient satisfaction with return to physical activity following metatarsophalangeal arthrodesis.
Skiing and Snowboarding
Fifteen patients participated in alpine skiing and/or snowboarding. Boot modifications were needed for 40% of these patients (n = 6, 5 skiers and 1 snowboarder), and all patients were able to ski the same difficulty of terrain or greater than prior to surgery. Two of the 6 modifications included total customization of a new 2-system boot—including a soft primary boot component that clicks into a hard exoskeletal frame—in order to address the traditional mobility concerns with a rigid ski boot. The 2-system boot allowed for easier entry and exit from the boot and more flexibility within the endoskeleton boot component. One patient self-reported the need for fully customized boots to address comfort concerns but did not elaborate further on specific customizations. The other 3 patients require size and fit modifications that would accommodate personalized orthotics. Most patients (n = 10, 66.7%) returned to sport by 6 months. The time to maximum level of participation varied with 20% of patients (n = 3) reported returning to maximum level greater than 1 year (Figure 4).

Time required for return to activity and return to maximum level of activity following first-metatarsophalangeal arthrodesis for alpine skiing and snowboarding.
Four patients participated in Nordic or cross-country skiing both before and after surgery. One patient required postoperative ski boot modifications, and all patients reported an increase or same level of function postoperatively. Three of the patients (75%) returned to Nordic skiing within 6 months of their operation, whereas 1 reported returning more than 1 year postoperatively. Return to maximum level of activity required greater than 1 year for 2 patients (50%), with 1 patient achieving this between 3 and 6 months.
Discussion
This study demonstrates that first-MTP arthrodesis reliably permits return to sport and physical activity, including alpine and mountain sports, with 96% of patients returning to activity by 1 year. We established an expected timeline for return to sport and described the need for shoe wear or gear modifications in patients undergoing first-MTP arthrodesis. We found that all patients were able to return to full activity in the top 4 most common activities: walking, hiking, road biking, and alpine skiing/snowboarding. Nearly half of walkers and hikers were able to increase their activity with regards to mileage and speed.
After surgery, most patients reported subjective improvement and satisfaction with their surgery. More than 70% of patients reported improved participation, less perceived difficulty, and high levels of satisfaction in their return to physical activity. A systematic review by Baumann et al 3 evaluated return to hiking, golf, running, yoga, tennis, elliptical, and biking after first-MTP arthrodesis and found that the vast majority of patients (>90%) were able to return to these sports with a trend toward increased sport activity. Furthermore, for those specific sports ~10% to 30% of patients stated activity was easier after MTP arthrodesis whereas ~2% to 9% stated it was more difficult depending on the sporting activity. This reflects our results where only 6.7% of patients stated increased difficulty in returning to sport after surgery.
Although most patients were able to maintain or increase activities, 24.4% were unable to return to one or more of the sports or activities they participated in preoperatively. Road and trail runners were least likely to return to preoperative activity, with running speed most affected by MTP arthrodesis. This could be due to the lack of forward propulsion with toe dorsiflexion. A gait analysis by DeFrino et al 4 found that after first-MTP arthrodesis, patients had a significantly shorter stride length and a decrease in plantar flexion and ankle power at push-off. A retrospective review of functional outcomes after first-MTP arthrodesis by Brodsky et al 8 reported a 75% rate of return to jogging after surgery. Conversely, Da Cunha et al 1 reported all patients, including 12 runners, 3 yoga athletes, and 1 ice skater, being able to return to their desired preoperative physical activity following first-MTP fusion. Our findings may differ because of an older patient population compared with that in Da Cunha’s study (58.8 vs 49.7 years). We observed that runners able to continue after surgery were on average 4.3 years younger than those unable, but this difference was not statistically significant. Ultimately, other factors may be more important such as foot strike patterns (forefoot vs midfoot or heel strike) and overall patient fitness. Further research is needed to determine what factors impact the ability to return to running after first-MTP arthrodesis.
When evaluating all sports, we found no difference in age between patients able to return to sport after surgery (56.9 years) and those unable to return to sport (56.8 years), supporting prior literature that age is generally not a determinant of return to sport or satisfaction.1,6,9 A recent matched case control study by Scheurer et al 10 compared patients <50 years old with those >60 years old after first-MTP arthrodesis and actually found greater pain relief in the younger cohort and equal functional outcomes in both groups. Furthermore, a prospective cohort of 16 elite athletes with a mean age of 27 years who underwent first-MTP arthrodesis found that 75% of the athletes were able to return to their original level of play by 1 year and all athletes were satisfied or very satisfied at final follow-up. 11
Most patients (96%) returned to their activities by 12 months postoperatively; 24% required longer to reach their maximum activity level. Similarly, Da Cunha et al 1 found that return to maximum level of activity was not achieved until greater than 13 months for 26.1% of sports/activities. This may be due to patients becoming accustomed to different loading characteristics or the need for continued footwear modifications as swelling subsides and gait normalizes. Patients can be educated preoperatively that they may continue to see improvement in physical activity participation greater than 1 year after surgery.
The younger cohort reported by Da Cunha et al 1 had a median time to return to activity of 6- 9 months. Our findings suggest a slightly earlier timeline for return to preoperative activity for some patients participating in alpine sports; however, our return to sport data had a wide range and is skewed by the seasonality of some sports. Most patients in this study returned to their preoperative level of activity by 6 months after surgery, and 11 patients (24.4%) were able to return to activity by 3 months, despite our older patient population. However, similar to Da Cunha, the recovery time needed to participate in maximal activity level could take up to a year.
One novel aspect of this study was the inclusion of alpine sports. To our knowledge this is the largest reported series of outcomes in skiers after first-MTP arthrodesis. One third of the study population participated in alpine skiing, snowboarding or Nordic skiing. Notably, all patients were able to ski, snowboard, and/or Nordic ski at the same or a more difficult level of terrain postoperatively. Return to skiing was variable with regard to timing, which we believe was due to the seasonality of the sport.
Another novel aspect of this study was the focus on shoe and gear modification for specific sports, which has not been described in detail in prior studies. Brodsky et al’s 8 retrospective review found that most patients had some limitation in shoe wear; 47% of their patient cohort required comfortable shoes with adequate depth and a low heel. Similarly, DeSandis et al 12 reported that 53% of patients had limitations in footwear, with 79% of patients limited to wearing comfort shoes only. In our study, 42.2% of the patients reported the need for footwear modifications, most common being a custom orthotic, larger shoe with a bigger toe box, better-quality or more cushioned shoe, and a flatter or stiffer shoe. Notably only 25% of road cyclists reported the need for shoe modification. Alpine skiers needed more boot modifications than snowboarders or Nordic skiers (38.5% vs 33.3% and 25%, respectively). Preoperative education on the possibility of footwear modifications is important to set appropriate expectations for the patient. This is particularly important for recreational runners, cyclists, hikers, and skiers given the cost of replacing existing equipment.
There are several limitations to this study. This study is limited by a response rate of less than 50%, introducing the potential for nonresponse bias, as respondents may differ systematically from nonrespondents. Additionally, the questionnaires were administered retrospectively, possibly leading to recall bias. We attempted to minimize recall error by using 3-month intervals for return to sport timelines. We are noticeably limited by the number of participants in certain sports, which may reduce the reliability of the data for those activities. However, given the limited data in the literature on these less popular sports, the information gained could be used as a point of further investigation in a larger study. Furthermore, risk factors for inability to return to sport could be identified with further studies.
Conclusion
This study supports prior literature findings of high satisfaction rates and high rates of return to activity, including alpine activities such as skiing, snowboarding, mountain biking, climbing, and hiking, after MTP arthrodesis, regardless of age. Most patients were able to return to activity 6 months after surgery, but full recovery and achievement of the maximum level of activity can take more than 1 year. The majority of patients, >70%, reported an improved level of participation in their desired sport and perceived their sport as less difficult after surgery. Walkers and hikers had the highest rates of increase in activity, with around 50% able to increase their mileage. Runners should be cautioned about the higher risk of inability to return to running and possible decline in speed. Nordic and alpine skiers and snowboarders were all able to return to the same or higher level of sport, but nearly half required boot modifications. Similarly, nearly half of patients in this study required some level of shoe modification, and patients should be counseled on this possibility. This study adds to the current body of literature supporting return to sport after first-MTP arthrodesis. Further studies can help determine better which factors contribute to the lack of return to sport for specific patients and sports.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114261433961 – Supplemental material for Return to Physical Activity and Footwear Modifications After First Metatarsophalangeal Joint Arthrodesis, Including Alpine Sports: A Retrospective Case Series
Supplemental material, sj-pdf-1-fao-10.1177_24730114261433961 for Return to Physical Activity and Footwear Modifications After First Metatarsophalangeal Joint Arthrodesis, Including Alpine Sports: A Retrospective Case Series by Stefan C. Garcia, Nathaniel E. Zona, Kenneth J. Hunt and Marissa D. Jamieson in Foot & Ankle Orthopaedics
Footnotes
Ethical Considerations
This study was designated as exempt from IRB review by the Colorado Multiple Institutional Review Board (IRB #22-2293).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Disclosure forms for all authors are available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.